World Tuberculosis Day: unite, invest and deliver to end TB
Tuberculosis (TB) and HIV are intricately linked, and they present profound challenges for global health. In 2023, 1.25 million people lost their lives to TB, including 161 000 people living with HIV. As the leading life threating comorbidity of HIV infection, TB accounted for nearly one third of all deaths among people living with HIV in 2023. Despite the progress made in the TB and HIV responses, antiretroviral treatment coverage for people with HIV/TB co-infection was only at 58% in 2023…

UNAIDS Executive Director Message on World TB Day – Yes, we shall and we can end TB among people living with HIV!
Today, on World TB Day, we must recognize the urgent need to end the TB epidemic around the world, especially among people living with HIV.

Impact of COVID-19 hits hard as TB deaths among people living with HIV rise for the first time since 2006
On World Tuberculosis Day 2022, UNAIDS is calling for urgency in diagnosing and treating TB as TB deaths among people living with HIV rise for the first time after years of progressive decline

TB disease and deaths declining among people living with HIV, but there have been some reversals due to the COVID-19 pandemic
While progress has been achieved in recent years, there have been some reversals due to the COVID-19 pandemic. There has been a steady decline in the estimated number of incident TB cases among people living with HIV. However, just 48% of the estimated 787 000 TB episodes globally among people living with HIV in 2020 were diagnosed and notified. This reflects a decline for the first time since 2004 in the percentage of estimated incident TB cases among people living with HIV that were notified,…

First Lady of Côte d’Ivoire sponsors national consultation on paediatric HIV and tuberculosis
Children living with HIV are particularly susceptible to tuberculosis (TB), one of the leading causes of AIDS-related deaths. In 2020, according to government statistics, 9400 people died of AIDS-related illnesses in Côte d’Ivoire, including 800 children under the age of 14 years. There were 21 000 people under the age of 15 years living with HIV in the country—only 49% had access to antiretroviral therapy. How to correct such an inequality was the question at the heart of a national…

Positive Women with Disabilities in Uganda puts people at the centre during COVID-19 pandemic
The World Health Organization estimates that, globally, more than 1 billion people (15% of the world’s population) have a disability. Disability is increasing in prevalence due to ageing populations, trauma, accidents and chronic health conditions, including HIV, tuberculosis (TB) and COVID-19.
Tuberculosis deaths among people living with HIV are declining globally, but worrying gaps in TB care persist
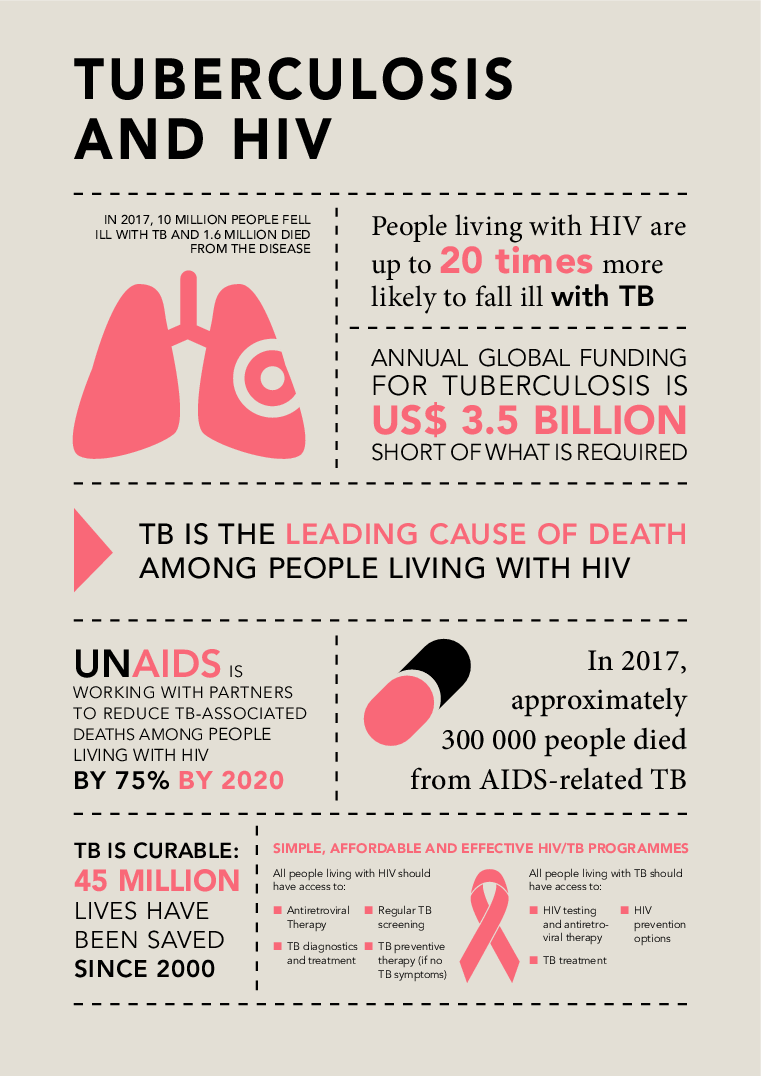
Globally, the number of people living with HIV who died from tuberculosis (TB), a curable and preventable disease, has fallen from almost 600 000 deaths in 2010 to just over 200 000 in 2019, a fall of 63%. In 2016, a global target was set by the United Nations to reduce TB deaths among people living with HIV by 75% between 2010 and 2020. Nine countries (Djibouti, Eritrea, Ethiopia, India, Malawi, South Africa, Sudan, Thailand and Togo) achieved or exceeded the global target by the end of 2019,…
Huge gaps in TB care for people living with HIV in some countries
All (100%) of people living with HIV newly started on antiretroviral therapy should receive either tuberculosis (TB) preventive treatment (blue bar) or TB treatment (orange bar)—together, they represent “optimal TB care”. The green bar shows the percentage of people newly started on antiretroviral therapy who did not receive optimal TB care and are vulnerable to falling ill or dying from TB.

Monitoring HIV/TB services in the Democratic Republic of the Congo
UCOP+, the Congolese Union of Organizations of People Living with HIV, through funding and technical support from UNAIDS, set up the Observatory project, designed to collect and analyse data to guide action to improve the quality of HIV services.

Tuberculosis testing gap among people living with HIV is narrowing
The risk of developing tuberculosis among the 38 million people living with HIV in 2019 was 18 times higher than in the rest of the world’s population. Tuberculosis remains the single largest cause of premature death among people living with HIV.