A new website that enables people to identify national laws and policies related to the AIDS response has been launched by UNAIDS.
Covering areas as diverse as a country’s ability to diagnose HIV among young babies, the existence of laws that discriminate against transgender people and whether people are prosecuted for carrying condoms, the Laws and Policies Analytics website aims to give a full overview of a country’s laws and policies related to the HIV response. It also allows to view policy data jointly with other data on the HIV epidemic and response.
“We must better understand legal and policy environments to drive effective responses to the HIV epidemic. This new tool will provide access to data on national laws and policies and allow for joint analysis with data on the epidemic and response, so that we can drive more deeply-informed decision-making,” said Shannon Hader, UNAIDS Deputy Executive Director, Programme.
Under the 2016 United Nations Political Declaration on HIV and AIDS, countries committed to accelerate efforts to significantly increase the availability of high-quality data on HIV. The information used on the new website was reported since 2017 and most recently in 2019 through the National Commitments and Policy Instrument (NCPI), a part of the Global AIDS Monitoring mechanism through which countries report their progress against the commitments they made in the 2016 Political Declaration.
Data were provided by national authorities, civil society organizations and other nongovernmental partners engaged in the AIDS response. Data on HIV-related laws and policies compiled from other external official documents complement the nationally supplied data. UNAIDS carries out a thorough validation of all policy data included to ensure their accuracy. Data will be updated annually.
The website hosts data from over 140 countries. Users can search by country or region through an interactive map or can select a specific topic.
Through making policy data widely available, UNAIDS seeks to promote transparency and an increased use of policy data in analyses of the HIV epidemic and the response to HIV in countries worldwide.
UNAIDS calls for greater urgency as global gains slow and countries show mixed results towards 2020 HIV targets
16 July 2019
16 July 201916 July 2019
Impressive advances in some countries, troubling failures in others as available resourc
Impressive advances in some countries, troubling failures in others as available resources for HIV fall by nearly US$ 1 billion
ESHOWE/GENEVA, 16 July 2019—The pace of progress in reducing new HIV infections, increasing access to treatment and ending AIDS-related deaths is slowing down according to a new report released today by UNAIDS. UNAIDS’ Global AIDS Update, Communities at the centre, shows a mixed picture, with some countries making impressive gains while others are experiencing rises in new HIV infections and AIDS-related deaths.
“We urgently need increased political leadership to end AIDS,” said Gunilla Carlsson, UNAIDS Executive Director, a.i., “This starts with investing adequately and smartly and by looking at what’s making some countries so successful. Ending AIDS is possible if we focus on people, not diseases, create road maps for the people and locations being left behind, and take a human rights-based approach to reach people most affected by HIV.”
The report shows that key populations and their sexual partners now account for more than half (54%) of new HIV infections globally. In 2018, key populations—including people who inject drugs, gay men and other men who have sex with men, transgender people, sex workers and prisoners—accounted for around 95% of new HIV infections in eastern Europe and central Asia and in the Middle East and North Africa.
However, the report also shows that less than 50% of key populations were reached with combination HIV prevention services in more than half of the countries that reported. This highlights that key populations are still being marginalized and being left behind in the response to HIV.
Mary Mahy UNAIDS Special Adviser, Epidemiology and Monitoring
Globally, around 1.7 million people became newly infected with HIV in 2018, a 16% decline since 2010, driven mostly by steady progress across most of eastern and southern Africa. South Africa, for example, has made huge advances and has successfully reduced new HIV infections by more than 40% and AIDS-related deaths by around 40% since 2010.
However, there is still a long way to go in eastern and southern Africa, the region most affected by HIV, and there have been worrying increases in new HIV infections in eastern Europe and central Asia (29%), in the Middle East and North Africa (10%) and in Latin America (7%).
The report was launched at a community event in Eshowe, South Africa, by Ms Carlsson and David Mabuza, the Deputy President of South Africa. It contains case studies and testimonies identifying community programmes that can quicken the pace of the response to HIV.
“South Africa has a rich history of communities being at the centre of the AIDS response, so it is fitting that we launch the 2019 UNAIDS Global AIDS Update in this country, in Eshowe, in KwaZulu-Natal, where a community-based service delivery model, with HIV at its centre, is showing results,” said Deputy President Mabuza.
Financing
Disconcertingly, the report shows that the gap between resource needs and resource availability is widening. For the first time, the global resources available for the AIDS response declined significantly, by nearly US$ 1 billion, as donors disbursed less and domestic investments did not grow fast enough to compensate for inflation. In 2018, US$ 19 billion (in constant 2016 dollars) was available for the AIDS response, US$ 7.2 billion short of the estimated US$ 26.2 billion needed by 2020.
To continue progress towards ending AIDS, UNAIDS urges all partners to step up action and invest in the response, including by fully funding the Global Fund to Fight AIDS, Tuberculosis and Malaria with at least US$ 14 billion at its replenishment in October and through increasing bilateral and domestic funding for HIV.
Jose Antonio IzazolaUNAIDS Special Adviser, Resource Tracking and Finances
Treatment and the 90–90–90 targets
Progress is continuing towards the 90–90–90 targets. Some 79% of people living with HIV knew their HIV status in 2018, 78% who knew their HIV status were accessing treatment and 86% of people living with HIV who were accessing treatment were virally suppressed, keeping them alive and well and preventing transmission of the virus.
Communities at the centre shows however that progress towards the 90–90–90 targets varies greatly by region and by country. In eastern Europe and central Asia for example, 72% of people living with HIV knew their HIV status in 2018, but just 53% of the people who knew their HIV status had access to treatment.
“I’ve been on treatment for 16 years, am virally suppressed and doing well,” said Sthandwa Buthelezi, founder of Shine, an organization in Eshowe that addresses stigma and discrimination in the community. “But stigma and discrimination are still widespread, particularly in health care settings. As an activist, I encourage everyone, including community leaders, to talk openly about HIV so that people can live positively and shine.”
AIDS-related deaths
AIDS-related deaths continue to decline as access to treatment continues to expand and more progress is made in improving the delivery of HIV/tuberculosis services. Since 2010, AIDS-related deaths have fallen by 33%, to 770 000 in 2018.
Progress varies across regions. Global declines in AIDS-related deaths have largely been driven by progress in eastern and southern Africa. In eastern Europe and central Asia however, AIDS-related deaths have risen by 5% and in the Middle East and North Africa by 9% since 2010.
Children
Around 82% of pregnant women living with HIV now have access to antiretroviral medicines, an increase of more than 90% since 2010. This has resulted in a 41% reduction in new HIV infections among children, with remarkable reductions achieved in Botswana (85%), Rwanda (83%), Malawi (76%), Namibia (71%), Zimbabwe (69%) and Uganda (65%) since 2010. Yet there were nearly 160 000 new HIV infections among children globally, far away from the global target of reducing new HIV infections among children to fewer than 40 000 by 2018.
More needs to be done to expand access to treatment for children. The estimated 940 000 children (aged 0–14 years) living with HIV globally on antiretroviral therapy in 2018 is almost double the number on treatment in 2010. However, it is far short of the 2018 target of 1.6 million.
Women and adolescent girls
Although large disparities still exist between young women and young men, with young women 60% more likely to become infected with HIV than young men of the same age, there has been success in reducing new HIV infections among young women. Globally, new HIV infections among young women (aged 15–24 years) were reduced by 25% between 2010 and 2018, compared to a 10% reduction among older women (aged 25 years and older). But it remains unacceptable that every week 6200 adolescent girls and young women become infected with HIV. Sexual and reproductive health and rights programmes for young women need to be expanded and scaled up in order to reach more high-incidence locations and maximize impact.
HIV prevention
Communities at the centre shows that the full range of options available to prevent new HIV infections are not being used for optimal impact. For example, pre-exposure prophylaxis (PrEP), medicine to prevent HIV, was only being used by an estimated 300 000 people in 2018, 130 000 of whom were in the United States of America. In Kenya, one of the first countries in sub-Saharan Africa to roll out PrEP as a national programme in the public sector, around 30 000 people accessed the preventative medicines in 2018.
The report shows that although harm reduction is a clear solution for people who inject drugs, change has been slow. People who inject drugs accounted for 41% of new HIV infections in eastern Europe and central Asia and 27% of new HIV infections in the Middle East and North Africa, both regions that are lacking adequate harm reduction programmes.
Men remain hard to reach. Viral suppression among men living with HIV aged 25–34 years is very low, less than 40% in some high-burden countries with recent surveys, which is contributing to slow progress in stopping new HIV infections among their partners.
Stigma and discrimination
Gains have been made against HIV-related stigma and discrimination in many countries but discriminatory attitudes towards people living with HIV remain extremely high. There is an urgency to tackle the underlying structural drivers of inequalities and barriers to HIV prevention and treatment, especially with regard to harmful social norms and laws, stigma and discrimination and gender-based violence.
Criminal laws, aggressive law enforcement, harassment and violence continue to push key populations to the margins of society and deny them access to basic health and social services. Discriminatory attitudes towards people living with HIV remain extremely high in far too many countries. Across 26 countries, more than half of respondents expressed discriminatory attitudes towards people living with HIV.
Communities
The report highlights how communities are central to ending AIDS. Across all sectors of the AIDS response, community empowerment and ownership has resulted in a greater uptake of HIV prevention and treatment services, a reduction in stigma and discrimination and the protection of human rights. However, insufficient funding for community-led responses and negative policy environments impede these successes reaching full scale and generating maximum impact.
Laurel SpragueUNAIDS Special Adviser, Community Mobilization
In KwaZulu-Natal in South Africa, one in four adults (aged 15–59 years) were living with HIV in 2016. To advance the response, Médecins Sans Frontières managed a community-based approach to HIV testing that links people to treatment and supports them to remain in care. By 2018, the 90–90–90 targets were achieved in Eshowe town, rural Eshowe and Mbongolwane, well ahead of the 2020 deadline.
Another study in South Africa and Zambia enrolled hundreds of Community HIV Care Providers (CHIPS) over five years to visit homes, provide information about HIV and offer HIV testing and linkage to care. The study found that areas with CHIPS communities had around 20% fewer new HIV infections each year and the proportion of people living with HIV who knew their HIV status, were on antiretroviral therapy and were virally suppressed increased from 54% to more than 70%.
UNAIDS urges countries to live up to the commitment made in the 2016 United Nations Political Declaration on Ending AIDS for community-led service delivery to be expanded to cover at least 30% of all service delivery by 2030. Adequate investments must be made in building the capacity of civil society organizations to deliver non-discriminatory, human rights-based, people-centred HIV prevention and treatment services in the communities most affected by HIV.
In 2018, an estimated:
37.9 million [32.7 million–44.0 million] people globally were living with HIV
23.3 million [20.5 million–24.3 million] people were accessing antiretroviral therapy
1.7 million [1.4 million–2.3 million] people became newly infected with HIV
770 000 [570 000–1.1 million] people died from AIDS-related illnesses
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Malawi has become the latest country to launch a health situation room, a software platform desig
Malawi has become the latest country to launch a health situation room, a software platform designed to help the government make informed decisions about policies and programmes related to health, including HIV.
The innovative tool bolsters national information systems through real-time visualization of information from multiple data sets. It will enable leaders and programme managers to improve health programmes to achieve the 90–90–90 targets, whereby 90% of people living with HIV know their HIV status, 90% of people who know their HIV-positive status are accessing treatment and 90% of people on treatment have suppressed viral loads by 2020.
Malawi is making good progress in its response to HIV. In 2017, 90% of people living with HIV in the country knew their status, 71% of people living with HIV had access to treatment and 61% of people living with HIV had a suppressed viral load. Around 1 million people are living with HIV in Malawi, with new HIV infections in 2017 down by 40% since 2010. However, HIV infections among young women and adolescent girls aged 15–24 years remain high and account for more than one in four new infections per year.
In his speech at the launch of the health situation room in the capital, Lilongwe, the President of Malawi, Arthur Peter Mutharika, said the tool was an important step forward.
“The health situation room is a demonstration of my government’s commitment towards accountability and transparency,” said Mr Mutharika. “My desire is that the health situation room will show us where to focus to improve even further in our quest for a healthier Malawi.”
The Executive Director of UNAIDS, Michel Sidibé, said the launch would strengthen the country’s health sector.
“The health situation room is an important innovation as it shares real-time data to improve the understanding of the country’s HIV epidemic and other health challenges,” said Mr Sidibé at the launch. “It will guide Malawi’s response and help officials to close the gaps, ensuring that no one is left behind as the country gets on track to end the AIDS epidemic by 2030.”
unaids.orgUNAIDS
Modelling the next set of HIV data
26 March 2019
26 March 201926 March 2019
Thirty minutes before the workshop had even started, the meeting room was full.
Thirty minutes before the workshop had even started, the meeting room was full. A murmur of voices echoed around the room as the participants took a last look at the data that would be used in the next round of HIV estimate modelling. It was important to get this right—the results of the workshop would eventually influence the allocation of billions of United States dollars-worth of investments in the AIDS response.
More than 100 people from 11 countries in eastern and southern Africa, supported by nine organizations, had come together in Johannesburg, South Africa, to analyse the trends and burden of the HIV epidemic in their countries. The UNAIDS workshop was one of 11 held worldwide between 28 January and 30 March 2019 during which 140 country teams—including epidemiologists, HIV programme managers and monitoring and evaluation experts—learned about the latest updates to the software used to estimate the number of people living with HIV, new HIV infections and AIDS-related deaths.
Over the course of the workshops, the teams produced new estimates on the HIV epidemics in their countries from 1970 to 2018, refining estimates made in past years. Country programmes and donor responses are based on the latest and most accurate data. Such data are used to set targets, identify hotspots, revise national programmes and decide the course of the AIDS response.
Before they arrive at the workshop, the country teams collect programme and surveillance data from their health information systems. At the workshop, those data are entered into Spectrum—a sophisticated UNAIDS-supported computer software package used to compile and analyse data on the HIV epidemic—to produce country HIV estimates.
Those countries that have good facility-level data use that information, together with data on road networks, population densities and other variables, to calculate the number of people living with HIV by district—information that is crucially important for a location–population approach to the AIDS response. Those district estimates are further broken down into different age groups and by sex.
Countries that receive funds from the United States of America import their estimates into a spreadsheet known as the Data Pack, which is used in the process to determine the level of financial support a country will receive.
One country whose AIDS response is supported by the United States is Lesotho. Assigned to support the country team members during the Johannesburg meeting was John Stover, the lead developer of Spectrum, who has an exceptional ability to explain complex concepts and find rigorous solutions even where few data exist.
The Lesotho country team members were eager to develop a comprehensive plan as part of Lesotho’s bid for additional funding, but they were concerned about the new estimates of child HIV infections, which were higher than their previous estimates. Mr Stover worked with the team over the course of the week to walk them through each of the assumptions made in the models, explaining how the model matched the data available from the country and the recent Lesotho Population-Based HIV Impact Assessment (LEPHIA) results and what caused the change in the estimates. A new tool has been included in Spectrum that shows where the new child infections came from and how to strengthen the prevention of mother-to-child HIV transmission programme to reduce the number of new child HIV infections in the future. When they left the workshop, the team had the capacity to explain the new estimates to policy-makers in Lesotho and beyond and to propose how to lower those new HIV infections in the future.
Additional workshops that trained more than 500 people on the Spectrum software have been held around the world, including in: Bangkok, Thailand; Panama City, Panama; Marrakesh, Morocco; Dakar, Senegal; Stockholm, Sweden; and Port of Spain, Trinidad and Tobago. The workshops were supported by facilitators from 14 organizations.
The estimates produced in the workshops will be reviewed by staff at UNAIDS over the coming month for quality assurance, before being signed off by ministers of health and published by UNAIDS at aidsinfo.unaids.org and in a UNAIDS report in mid-2019.
unaids.orgUNAIDS
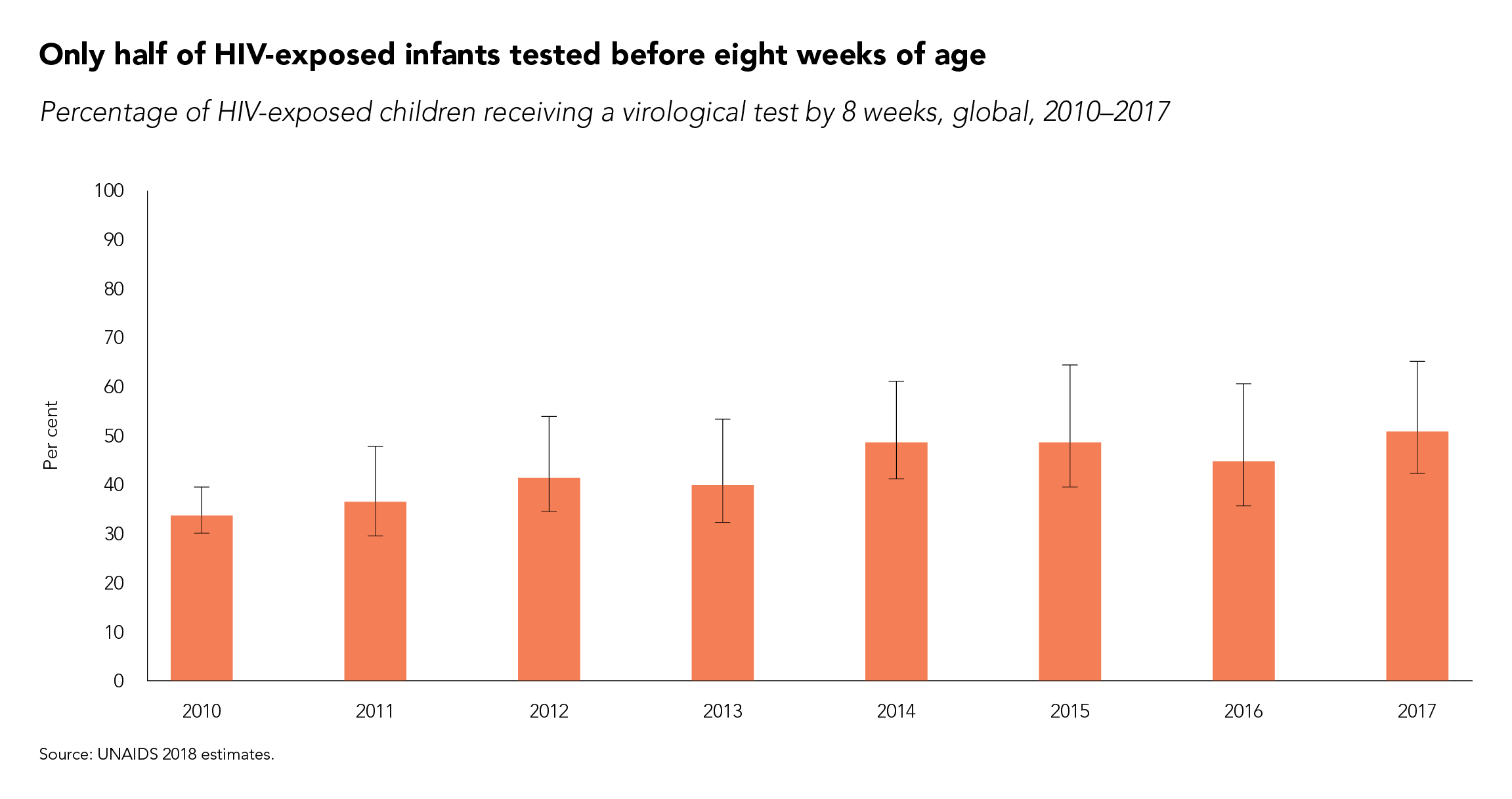
Only half of HIV-exposed babies are tested for HIV
25 March 2019
25 March 201925 March 2019
The earlier that a baby who has been born with HIV is diagnosed and starts treatment, the better
The earlier that a baby who has been born with HIV is diagnosed and starts treatment, the better the outcome.
To diagnose children younger than 18 months of age with HIV requires virological testing, which detects the virus or its components. Serological testing―which tests for HIV antigen and/or antibody generated as part of the immune response to infection―is used for children older than 18 months and adults. Serological testing cannot be used for infants, since it can’t differentiate between HIV antibody produced by the mother and then passed to her baby during the pregnancy, with the baby remaining uninfected, and HIV antibody produced by an HIV-infected baby.
Virological testing is not consistently available in most low- and middle-income countries, however, and when it is available it is often expensive and time-consuming, involving several clinic visits for mothers and infants, the transport of samples to centralized laboratories and potential delays in the return of results.
Globally, only half of infants who are exposed to HIV during pregnancy are tested before eight weeks of age. Since mortality among untreated infants is highest in the first three months of life, prompt diagnosis and linkage to treatment are crucial.
Survey interviewers crossing river in the North-East
The road to NAIIS: UNAIDS’ role in better understanding Nigeria’s HIV epidemic
22 March 2019
22 March 201922 March 2019
After six months of data collection and three months of data analysis, the President of Nigeria,
After six months of data collection and three months of data analysis, the President of Nigeria, Muhammadu Buhari, announced the results of the Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS) in March 2019. Costing approximately US$ 100 million and covering more than 200 000 people, 185 survey teams collected data for the NAIIS, the largest HIV-specific survey in the history of the global response to the epidemic.
In Nigeria, three types of survey have been conducted by the Federal Ministry of Health HIV/AIDS Division to determine HIV prevalence and to monitor the trends of the HIV epidemic in the country:
The HIV Sentinel Survey (HSS), which is conducted typically every two to three years among women attending antenatal clinics, which determines HIV prevalence among pregnant women.
The National Reproductive Health Survey (NARHS), which is conducted every five years among the general population.
The Integrated Biological and Behavioural Surveillance Survey (IBBSS), which is mostly used to monitor prevalence and behavioural trends among key populations.
The last HSS and IBBSS took place in 2014, while the last NARHS took place in 2012. These data sources have served as the main survey data sources for the AIDS response in the country.
Between 2012 and 2014, significant progress was made in the AIDS response in Nigeria. The number of antiretroviral therapy sites doubled, prevention of mother-to-child transmission sites increased eightfold and HIV counselling and testing sites increased fourfold. According to government data, 6.7 million adults were counselled and tested for HIV in 2014, a 65% increase from the previous year. HIV testing among pregnant women also doubled in 2014 compared to 2013. Similarly, the number of people living with HIV on antiretroviral therapy increased significantly.
However, despite this progress, there was no commensurate improvement in the statistics on the coverage of antiretroviral therapy among people living with HIV. National achievements in the AIDS response were poor compared to the targets, and programme implementers reported difficulties in identifying people living with HIV in need of services. It was therefore suggested that the HIV burden was not as high as was estimated using the available HIV prevalence data.
Former UNAIDS Country Director Dr Bilali Camara was a longstanding advocate for an expansion of the surveillance of the country’s epidemic.
“Working as UNAIDS Country Director in Nigeria, I realized early on that we did not have the full picture of the country’s AIDS epidemic,” said Dr Camara. “I was pushing for surveillance to be expanded for a long time―I am very happy that with this new survey we now have a better understanding of the AIDS epidemic in Nigeria and that it will allow us to better respond to the areas and people in most need.”
Dr Camara’s persistence indeed paid off.
In July 2015, the National Agency for the Control of AIDS (NACA), under the leadership of its then Director-General, Professor John Idoko, decided that it was imperative to better understand Nigeria’s HIV epidemic. The NACA set up a National Stakeholder Committee, comprising the head of the National AIDS and STI Control Programme, the UNAIDS Country Director, the World Health Organization (WHO) representative, the United States President’s Emergency Plan for AIDS Relief (PEPFAR) Coordinator, civil society and others, which decided to conduct a triangulation of data from various sources.
“The need for the survey was first initiated under my leadership, but we had overwhelming support from Dr Camara. UNAIDS headquarters was even willing to send its Strategic Information Director to Nigeria at the time,” said Professor Idoko.
Many countries have shifted to a location–population approach, which helps to ensure that HIV services reach the people and geographic areas with the greatest need. Location–population approaches require granular-level data, which were not typically available in Nigeria. In 2016, the UNAIDS Nigeria Strategic Information Team, led by Dr Gatien Ekanmian, was tasked to develop an evidence-informed methodology to estimate the HIV burden at the local level. During this process, a closer analysis of the results from the various surveys highlighted a series of issues with the HSS surveys:
The sentinel sites were too limited in number to ensure nationally representative geographic coverage based on the demographics of the country.
Urban sites were oversampled.
Rural sites were usually under-sampled.
There were often more urban sites than rural sites in many states, thus the HSS results reflect more the urban HIV epidemic than the rural epidemic among pregnant women.
The conclusion of the UNAIDS Nigeria epidemiological analysis was that the HSS and NARHS were no longer giving sufficiently precise epidemiological information. It was recommended that a comprehensive review of the HIV surveys being conducted in Nigeria be carried out in order to address the shortcomings in the existing survey approaches and methodology.
Thereafter, the UNAIDS country office met with various stakeholders, including the Development Partners’ Group on HIV, and presented these observations and recommendations, effectively utilizing the Development Partners’ Group on HIV to galvanize support from PEPFAR and the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) in particular.
In June 2016, the Director-General of the NACA raised an objection to the latest estimate of 3.5 million Nigerians living with HIV, believing that the figure was an overestimation. He had the opportunity to discuss his concerns with UNAIDS country directors, Dr Erasmus Morah and Dr Alti Zwandor at the International AIDS Conference in Durban, South Africa, in 2016. In July 2016, after advocacy from the UNAIDS country office, the new Minister for Health, Professor Isaac Adewole, and the new Director-General of the NACA, Dr Sani Aliyu, agreed on the need for an epidemiologically robust population-based HIV survey in Nigeria. They approved the recommendations for a population-based survey and committed to mobilize resources for it.
“When I resumed as Director-General of the National Agency for the Control of AIDS, a recurring issue that came up at every introductory meeting with partners was the difficulty in finding new cases. It was obvious that there was a problem with case-finding. Was this because we were looking in the wrong places? I had doubts on the quality data we had … and we can’t achieve epidemic control if we don’t even know where we are. Hence, the number one priority of my administration was born―establishing the true prevalence of HIV in Nigeria by employing the best scientific and technical survey tools available in the shortest possible time,” said Dr Aliyu.
In November 2016, a review and triangulation of HIV data in Nigeria was commissioned by the NACA, in collaboration with UNAIDS, the findings of which gave further support for a national survey to develop more precise estimates of HIV prevalence. Firm support for the survey came from the Government of the United States of America (the Centers for Disease Control and Prevention, PEPFAR, USAID and the Department of Defense) and the Global Fund, which committed funding to the NAISS.
“It was easy to see that getting the data situation in Nigeria right was not only the right thing to do but also the dream of so many people. Fortunately, Nigeria had great partners to help turn this dream into reality. Programming and accounting for HIV results in the country will never be the same,” said Dr Morah, the current UNAIDS Country Director for Nigeria.
The United Nations system’s contributions in the NAIIS Technical Committee were anchored by UNAIDS, WHO and the United Nations Children’s Fund. Before the results of the survey were announced, Peter Ghys, UNAIDS Director of the Strategic Information Department, led a multi-group technical mission to Nigeria. The team gave advice on the use of the survey results, on the trends and the geographic locations of the epidemic, at the national and subnational levels. They also gave technical guidance to national partners on data management and governance, including on a strategy for country ownership and leadership of the survey results and support on how to communicate the changes in the epidemiological profile of HIV in the country.
“The road to NAIIS is a wonderful and brilliant story to tell, because it actually tells the story of the HIV response in Nigeria,” said Professor Adewole.
This feature is adapted from an article written by Erasmus U. Morah, Gatien K. Ekanmian and Doris, A.Ogbang