
Feature Story
Partnerships and linking for action
06 марта 2008
06 марта 2008 06 марта 2008The Global Health Workforce Alliance (GHWA) held the first ever Global Forum on Human Resources for Health in Kampala, Uganda from March 2-7, 2008. The GHWA, hosted and administered by the World Health Organization (WHO), has been created to identify and implement solutions to the health workforce crisis.
UNAIDS Executive Director Dr Peter Piot gave the following plenary speech on "Partnerships and linking for action".
Plenary speech by Dr Peter Piot, UNAIDS Executive Director
Kampala, Uganda 5 March, 2008.

UNAIDS Executive Director Dr Peter Piot addressing plenary at the Global Forum on Human resources for Health, in Munyonyo, Kampala, 5 March 2008
Credit: UNAIDS/C. Opolot
Thank you Sigrun – and thank you for inviting me here today.
I came to Kampala for three reasons. Firstly, this Forum is one of the most important meetings in public health to take place this year. We are starting to build a coalition to address one of the greatest obstacles to health.
Secondly, I am here to pledge the firm support of UNAIDS to this initiative.
Thirdly, it is time to de-polarize this debate. Whether we invest in the AIDS response or in strengthening health systems. It is not a question of one or the other. Even when it comes to AIDS, it is not simply a question of strengthening health services but also community mobilization. We must not forget about people or health outcomes
The issue of human resources for health is complex. But we all know it’s not a new one. I lived it myself in the mid-70s in rural Zaire. But nor is it limited to Africa. Last week I was in India where this is an enormous maldistribution of human resources for health.
The shortage results from decades of under-investment by governments, donors and international agencies. It has been intensified by globalization, but globalization may also bring some of the solutions. Responsibility for the current situation is shared – between donors, national governments, NGOs, research organization and international organizations among others. We therefore have a shared duty to address it. That’s why this afternoon’s panel, with its focus on partnership, is so vital.
The debate we are having now is long overdue. And a major reason for its happening at all is AIDS!
One of the peculiar characteristics of AIDS is that it exposes injustices. AIDS - more than any other issue - has thrown a spotlight on the urgent need to strengthen human resources for health, for three reasons. Firstly, AIDS represents a significant burden on health systems. In some countries, half of all hospital beds are occupied with patients with AIDS-related illnesses. Secondly, to expand ART, and to make ART sustainable, we need strong health systems. Thirdly, being a health worker does not protect you from becoming infected. Botswana, for example lost approximately 17% of its healthcare workforce to AIDS between 1999 and 2005.
There have been good examples of how AIDS investment has helped overcome the human resources for health crisis. I remember well going to Malawi in 2004 with Sir Suma Chakrabarti, then Permanent Secretary of the UK’s DFID. AIDS had brought the health workforce literally to its knees. There was no way it could cope. It was an emergency that required exceptional measures. DFID and other donors financing the sector agreed to fund a groundbreaking initiative, the Emergency Human Resources Programme, to top up salaries for nurses and other health care workers as an incentive not to leave the country. This was totally novel: donors usually resist paying salaries, but in this case we managed to break the taboo. I’m glad to say that the Global Fund to Fight AIDS, Tuberculosis and Malaria is now supporting this programme.
This is just one example of another characteristic of AIDS: it forces us to do things differently. WHO’s “Treat, train, retain” initiative for health-workers with HIV is another new and pragmatic approach. I don’t know of any other programme that starts by addressing the health of the workers involved. It provides wins all round – to the health workers themselves, to the people who need their services, and to the health sector as a whole. So, when we are talking about strengthening health systems, let’s first make sure that people stay alive! But good partnerships require more than processes. There are too many partnerships that are not enough about results and outcomes.
AIDS funding and programming enhanced essential infrastructure for health facilities. Where HIV services have been integrated into existing service delivery sites, AIDS money helped renovate health facilities, upgraded clinics and laboratories and provided training opportunities for health care workers.
AIDS has also helped promote “task shifting”, an old concept/idea in public health – moving responsibility for certain tasks to other health-workers and community members to free up doctors and nurses to take care of other patients and to deliver other essential health services. Here in Uganda, there is an increasing trend for people living with HIV to take on tasks such as counseling for testing, adherence support, treatment literacy and to produce good quality outcomes. In Kenya, several organizations have been implementing prevention, treatment literacy and home based care programmes, which are led by people living with HIV at the community level. Women Fighting AIDS in Kenya, supported by UNICEF in Kisumu and Port Reitz General Hospitals, trained PLWHAs who were then used as PMTCT champions to provide counseling to ante-natal mothers and their partners.
We also see, particularly here in Africa that faith-based organizations play a major in the fight against AIDS providing vital HIV care and treatment services. For example, Christian hospitals and health centers are providing about 40% of HIV care and treatment services in Lesotho and almost a third in Zambia. In other countries, the formal and informal private sector is also very important.
AIDS has brought in new resources, to benefit not only HIV programmes but health systems more widely. Take for example the Haitian “accompagnateurs” – community workers who have been brought into the health workforce through the AIDS programmme. Or in Rwanda, HIV treatment and care was integrated with regular health services, resulting in better coverage for maternal and child health according to a study by Family Health International (FHI) presented at last year’s PEPFAR Implementers Meeting in Kigali. Les Mutuelles de Santé is another example of financing scheme to mobilize resources for health services.
So I have serious issues with the current wave of statements like “There’s too much money going to AIDS” or “Donors should prioritize health system strengthening”. They completely ignore the growing body of evidence that AIDS expenditure strengthens the health sector and contributes to broader development programmes, besides the fact that AIDS programmes are having measurable results, saving millions of lives. Indeed, AIDS has been an advocate for health systems strengthening.
They also seem to assume that dealing with HIV is mostly about treatment. It isn’t! For every one person we put on antiretroviral therapy, another four or five become infected with HIV. If we don’t radically enhance HIV prevention, demands for treatment will just keep on growing, placing an even greater burden on health systems in the future.
And prevention – except for PMTCT – is far more than a health issue. Prevention is a community based action. Effective HIV prevention derives from a range of multi-sectoral interventions (governments, nongovernmental organizations, faith-based organizations, the education sector, media, the private sector and trade unions and people living with HIV).
A lot of the recent surge of funding started as a direct consequence of the AIDS epidemic. AIDS advocacy did not only succeed in mobilizing money, but it also highlighted the profound disparities in health services that separated the developing countries from the developed world. It is however true that there are examples where AIDS related activities and AIDS funding are taking away health workers from other tasks. AIDS funding created new and more interesting job opportunities for doctors and nurses with NGOs and foreign aid agencies and thus can be a drain on the public sector. We have seen it happening in Malawi and in Zambia where focus of disease programmes shifted to HIV. However, and certainly in the heavily affected countries, the AIDS burdens for health services is also a reality. We need to find common solutions and ways of working together.
This brings me to my next point. AIDS has taught us about the critical value of partnerships. Tackling AIDS is one of the toughest challenges the world faces today. Like dealing with climate change, it’s tremendously complex - way beyond the capacity of any single sector or institution. It’s one of those issues that jolts us out of our comfort zone, and forces us to create new alliances with a variety of constituencies – across sectors and at state and non-state level.
UNAIDS itself is a joint programme. We are working with a wide range of constituencies – government, scientists, business, labour, and the media. One of the most important partnerships of all has been our relationship with civil society. It was the activists who kick-started the AIDS movement. Without them, we wouldn’t have achieved anything like the progress we’ve made. It’s thanks to these partnerships that we have been able to mobilize political momentum around AIDS, to leverage funding to $10 billion per year.
In the twelve years since UNAIDS was created, we’ve learnt a lot about partnerships. We’ve seen the advantages of being able to convene diverse actors from public, private, and non profit sectors – all with different strengths. They have the potential to achieve spectacular results – way beyond anything they could hope to achieve on their own.
But coordination and accountability are still important. That’s why UNAIDS established the Three Ones principles, as a framework for partnerships on AIDS. Just to remind you, these are: one agreed national action framework, one national coordinating authority and one agreed monitoring and evaluation system.
The lessons we’ve learnt through implementing the Three Ones are salutary – and very relevant to the aims of this Alliance. The Agenda for Action is right to highlight the need for “national responses to be guided by a national leadership that convenes all actors around one agreed national effort”, and to point to the importance of accountability. The challenge is to engage serious commitment at all levels – in-country, in donor capitals and international organization headquarters. This requires time and effort. But it will be time and effort well spent.
I began today by saying that addressing the shortage of human resources for health was a joint responsibility. It is something that no institution can tackle alone. It is complex, cross-sectoral and long-term. And, like AIDS, it is not a quick-fix problem and there is no one solution that fits all. This may be a major reason why so little has been done before. Another reason may be the fact that the current crisis of human resources for health is also a highly political issue and therefore any possible solutions need to have full political support. But coming together in this alliance is in itself a tremendous step forward. There is a lot at stake; therefore our response must address the emergencies of today and to draw up longer-term plans for the future.
The Agenda for Action offers a comprehensive menu of activities, but I want to suggest some very concrete actions where we can all work and benefit together.
The first is that we must build partnerships far beyond the public sector. Partnerships are crucial for the success of any solution. We must also look at the critical role of non-state actors in the provision of services and their role in the training of human resources. In many countries, 40 to 60% of health services are delivered by the private sector. We have to establish more private/public partnerships with greater engagement of the private sector, beyond workplace programmes. Equally, in many countries, particularly here in Africa, many clinics and health centers are run by faith-based organization. We need to bring them all into the policy dialogue of heath services provision.
The second is to engage the full participation of civil society. As I mentioned earlier, civil society has been at the heart of the AIDS response from the very beginning. And its presence there has been vital. Not only does civil society activism mobilize action, but community members are an invaluable source of knowledge about what works and about how to reach people. We must listen and learn from them, and at the same time invest in building their capacity to deliver alongside that of public sector.
The third is for health ministries to make improving human resource management a priority. This is implicit in the Agenda for Action. But I think we need to spell it out more clearly. Today’s crisis has come about for two reasons. Lack of investment and lack of management. There’s a lot to do, but one of the first steps should be to establish incentives for performance and raise health-worker morale.
Fourth, we need to work together to question and challenge our concepts of fiscal space, predict medium term expenditure frameworks and the suitability of salary supplementation. We have to involve ministries of finance in the discussions of solutions. We should also work together with the World Bank and IMF on these constraints.
There is also the need to address the issue of public sector pay and work conditions. To address issues such as poor infrastructure, lack of equipment and drugs, long hours and heavy workloads and lack of career development in addition to poor remuneration. This needs to be combined with putting human resources for health on the agenda of civil service reform and donor willingness support and invest in supplementing health workers’ salaries and training. Donors and countries should consider the lessons learnt from the Malawi experience.
These issues are at the heart of any assessment of countries’ ability to scale up the response and the achievements of the MDGs. They are relevant for all of the health MDGs and need close examination and a common assessment of the risks and opportunities.

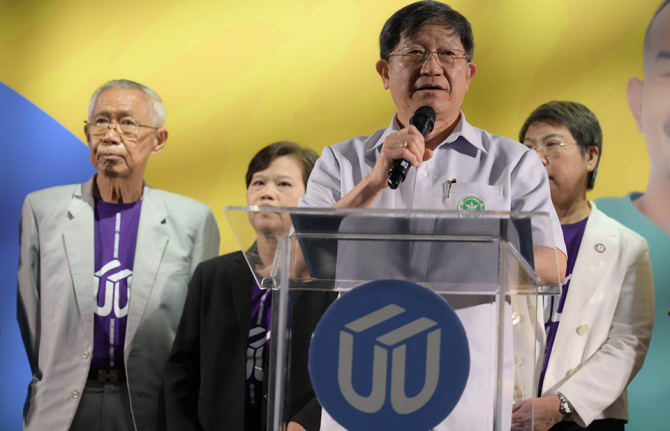
Press conference at the close of Global Forum on Human resources for Health, Kampala 5 March, 2008. (From left): Chair of the board Global Health Workforce Alliance, Dr Lincoln Chen; UNAIDS Executive Director, Dr Peter Piot and Representative of Women Living with HIV in Uganda, Beatrice Were.
Credit: UNAIDS/C. Opolot
We can be very ambitious, but need clear targets, goals and a partnership, where put the institutional interest aside. Fight for common good and common goal. We need to re-set the rules and to put into practice what has been discussed globally at country level. Every research programme must include overhead (/indirect costs for strengthening capacity. This is starting to be done among largest investors in heath (GAVI; GF; PEPFAR etc).
We also need to find a practical way to compensate low and middle-income countries that are losing their skilled staff in whose education they have invested.
The final – and most relevant for this afternoon’s session - is to be serious about applying the Three Ones principles, for all parties to come together and align around a single strategic plan for strengthening human resources for health that focuses clearly not just on process but on results. One National AIDS Coordination authority and one agreed country-level monitoring and evaluation system. Such a framework has been invaluable for a well coordinated AIDS response. We are not there yet, but we have made progress.
If we make progress on action plan, it will be because have worked together. It is through diversity we will success. Pragmatic approach is needed, one step at a time, and strong leadership which will hold us together. I believe we have that leadership.
That may sound ambitious. But if we can come back in a year’s time and say we’ve made progress in these four areas, the world’s health workforce will look a lot more robust than it does today – and its population will be fitter as a result.
We have to act now and “to work together to ensure access to a motivated, skilled, and supported health worker by every person in every village everywhere.” Dr. LEE Jong-wook
Thank you.
Partnerships and linking for action
Cosponsors:
WHO - Global Health Workforce Alliance
Feature stories:
Health workforce crisis limits AIDS response (29 February 2008)
External links:
First Global Forum on Human Resources for Health 2-7 March 2008, Kampala, Uganda
Publications:
Scaling up access to HIV prevention, treatment, care and support: The next steps (UNAIDS, 2006)
Global Health Workforce Alliance Strategic Plan (WHO)
Related
 Review recommends law reform on HIV testing to help Angola reduce new HIV infections among young people and ensure treatment
Review recommends law reform on HIV testing to help Angola reduce new HIV infections among young people and ensure treatment
11 мая 2022 года.
 Report highlights that women and marginalized people need urgent access to health-care services in Ukraine
Report highlights that women and marginalized people need urgent access to health-care services in Ukraine
11 мая 2022 года.
 Key considerations to integrate HIV and mental health interventions
Key considerations to integrate HIV and mental health interventions
28 апреля 2022 года.
Feature Story
Uniting against female genital mutilation
04 марта 2008
04 марта 2008 04 марта 2008
The Interagency Statement on
Eliminating Female genital
mutilation was signed by
UNAIDS, UNDP, UN Economic
Commission for Africa, UNESCO,
UNFPA, the Office of the High
Commissioner on Human Rights,
UNHCR, UNICEF, UNIFEM and
WHO.
Reaffirming their commitment to the elimination of female genital mutilation, 10 United Nations bodies including UNAIDS, have expressed their commitment to support governments, communities, and women and girls to abandon the practice within a generation.
There are a growing number of examples in countries around the world where the prevalence of female genital mutilation has declined. The interagency statement “Eliminating female genital mutilation” is a joint initiative to support the scaling up of good examples to become common practice.
Female genital mutilation, also called female genital cutting and female genital mutilation/cutting, violates the rights of women and girls to health, protection and even life as the procedure sometimes results in death. Although decades of work by local communities, government, and national and international organizations have contributed to reducing the prevalence of female genital mutilation in many areas, the practice remains widespread.
Damages public health and human rights
Between 100 and 140 million women and girls in the world are estimated to have undergone female genital mutilation and 3 million girls are estimated to be at risk of undergoing the procedures every year.
The statement points out that female genital mutilation is a manifestation of unequal relations between women and men with roots in deeply entrenched social, economic and political conventions.
The practice is believed to enhance a girl’s chastity and chances of marriage by controlling her sexuality. As such, it not only infringes on women’s sexual and reproductive health; it also perpetuates gender roles detrimental to women.
"We recognize that traditions are often stronger than law, and legal action by itself is not enough,” said all the agencies involved. “Change must also come from within. This is why it is critical for us to join hands and work closely with communities and their leaders so that they can bring about sustainable social change.”
Health complications of female genital mutilation
The statement highlights the damaging effect of female genital mutilation on the health of women, girls and newborn babies. Immediate risks of the practice include severe pain, shock and even death through hemorrhaging. The use of the same surgical instrument without sterilization could increase the risk for transmission of HIV between girls who undergo female genital mutilation together.
Long-term health risks include chronic pain, reproductive tract infections, birth complications and psychological consequences. An increased risk for bleeding during intercourse may increase the risk for HIV transmission. The increased prevalence of herpes in women subjected to female genital mutilation may also increase the risk for HIV infection, as genital herpes is a risk factor in the transmission of HIV.
The UN said, “We are becoming increasingly concerned about the medicalisation of female genital mutilation. This is where the mutilation is performed by health professionals in health facilities. The argument that a mild form performed by medically trained personnel is safer is commonly heard in countries where female genital mutilation is practiced. But this should never be considered as an option."
The statement argues that the treatment and care of the adverse health consequences of female genital mutilation should be an integral part of health services, such as safe motherhood and child survival programmes, sexual health counselling, psycho-social counselling, prevention and treatment of reproductive tract infections and sexually transmitted infections including HIV and AIDS, prevention and management of gender-based violence, youth health programmes and programmes targeting traditional birth attendants (who may also be traditional circumcisers).
New evidence and lessons learned
The interagency statement is based on new evidence and lessons learnt over the past decade. It highlights the wide recognition of the human rights and legal dimensions of the problem and provides current data on the prevalence of female genital mutilation.
It summarizes findings from research on the reasons why the practice continues, highlighting that the practice is a social convention which can only be changed through coordinated collective action by practising communities. It also summarizes recent research on its damaging effects on the health of women, girls and newborn babies.
Drawing on experience from interventions in many countries, the new statement describes the elements needed, for both working towards complete abandonment of female genital mutilation, and caring for those who have suffered, and continue to suffer, from its consequences.
The Interagency Statement on Eliminating Female genital mutilation was signed by the Joint UN Programme on HIV/AIDS (UNAIDS), the UN Development Programme (UNDP), The UN Economic Commission for Africa (UNECA), the UN Educational, Scientific and Cultural Organizations (UNESCO), the UN Population Fund (UNFPA), the Office of the High Commissioner on Human Rights (UNHCHR), The UN Refugee Agency (UNHCR), UNICEF, the UN Development Fund for Women (UNIFEM) and the World Health Organization (WHO).
Uniting against female genital mutilation
Cosponsors and partners:
UN Development Programme (UNDP)
UN Economic Commission for Africa (UNECA)
UN Educational, Scientific and Cultural Organizations (UNESCO)
UN Population Fund (UNFPA)
The Office of the High Commissioner on Human Rights (UNHCHR)
UN Refugee Agency (UNHCR)
United Nations Children Fund (UNICEF)
UN Development Fund for Women (UNIFEM)
World Health Organization (WHO)
External links:
WHO Department of Reproductive Health and Research
Publications:
Eliminating Female genital mutilation. An interagency statement. (February 2008)
Related
 The power of women supporting women - Mentor program for women living with and affected by HIV in Kazakhstan
The power of women supporting women - Mentor program for women living with and affected by HIV in Kazakhstan
13 сентября 2024 года.
 Young role models combat HIV stigma in Central Asia
Young role models combat HIV stigma in Central Asia
22 июня 2023 года.
 The urgency of HIV prevention among adolescent girls and young women
The urgency of HIV prevention among adolescent girls and young women
01 июня 2023 года.
Feature Story
Ограничения на поездки в связи с ВИЧ
04 марта 2008
04 марта 2008 04 марта 2008С начала эпидемии ВИЧ правительства и частный сектор вводят ограничения на поездки для ВИЧ-положительных людей, имеющих намерение въехать в страну или остаться в ней на короткий срок (например, деловые, частные поездки, туризм) или на более продолжительный срок (например, убежище, трудоустройство, иммиграция, переселение беженцев или учеба).

Международная целевая группа по
ограничениям на поездки в связи с ВИЧ
провела свое первое заседание в Женеве
25-26 февраля. Заседание проходило
под председательством ЮНЭЙДС и
правительства Норвегии.
ЮНЭЙДС создала международную целевую группу для привлечения внимания к проблеме ограничений на поездки в связи с ВИЧ (как краткосрочные, так и долгосрочные) на международном и национальном уровне и продвижения к их устранению.
Международная целевая группа провела свое первое заседание в Женеве 25-26 февраля. В работе заседания, под председательством представителей ЮНЭЙДС и правительства Норвегии, приняли участие представители правительств, межправительственных организаций и гражданского общества, включая частный сектор и сети людей, живущих с ВИЧ.
Согласно данным, собранным Европейской группой по лечению СПИДа, в общей сложности 74 страны имеют те или иные ограничения на поездки в связи с ВИЧ, причем в 12 из них ВИЧ-положительным людям запрещен въезд с любой целью и на любой срок. Чаще всего в качестве причины называется стремление защитить общественное здоровье и избежать возможных расходов в связи с уходом, поддержкой и лечением людей, живущих с ВИЧ.
Какой бы ни была причина, ограничения на поездки в связи с ВИЧ поднимают основополагающие проблемы в области прав человека, касающиеся недискриминации и свободы передвижения людей, живущих с ВИЧ, в сегодняшнем очень мобильном мире.
По оценкам Всемирной туристской организации, в 2000 году во всем мире насчитывалось 698 миллионов международных пассажиров. Большинство этих людей совершают краткосрочные поездки, например, с туристической, деловой целью, для участия в конференциях, для посещения семьи. Что касается более продолжительных поездок, то, по оценкам Международной организации по миграции (МОМ), за пределами своей страны постоянного проживания в настоящее время живут и работают 175 миллионов мигрантов, т.е. 2,9 процента мирового населения.
Ограничения на поездки в связи с ВИЧ обычно принимают форму закона или административной инструкции, которая требует, чтобы для въезда в страну или для дальнейшего пребывания в ней люди подтверждали отсутствие у них ВИЧ. В некоторых странах людям необходимо проходить тест на ВИЧ, в других - надо представить сертификат об отсутствии ВИЧ или просто заявить о своем ВИЧ-статусе.
Тестирование при таких обстоятельствах напоминает обязательное тестирование и во многих случаях проводится без надлежащего до- и послетестового консультирования или гарантий конфиденциальности. Любое тестирование на ВИЧ должно проводиться добровольно и на основе информированного согласия.
Для лиц, ищущих возможность иммигрировать, получить убежище, навестить семью, принять участие в совещании, получить образование или осуществить деловую сделку, воздействие ограничений на поездки в связи с ВИЧ на личность может быть разрушительным. Будущий иммигрант, беженец, студент или просто путешествующий может одновременно узнать, что он ВИЧ-инфицирован, что ему могут не разрешить совершить поездку и что, возможно, его статус стал известен правительственным должностным лицам, или семье, общине и нанимателю, в результате чего это лицо может столкнуться с серьезной дискриминацией и стигмой.
Тем, кто уже находится в принимающей стране, может грозить произвольная депортация, без необходимого юридического процесса и защиты конфиденциальности. При таких обстоятельствах, у этого лица есть все причины скрывать или отрицать свой ВИЧ-статус и избегать встречи с иммиграционными властями и медицинскими работниками. Тем самым подрывается иммиграционный контроль и усилия в области общественного здравоохранения, а отдельные лица лишаются доступа к профилактике, помощи и, вероятно, необходимым услугам здравоохранения..

“Ограничения на поездки на основе
ВИЧ-статуса, особенно краткосрочные
ограничения, вновь подчеркивают
исключительность СПИДа" - заявил
Исполнительный директор ЮНЭЙДС
д-р Питер Пиот.
“Ограничения на поездки на основе ВИЧ-статуса, особенно краткосрочные ограничения, вновь подчеркивают исключительность СПИДа» - заявил Исполнительный директор ЮНЭЙДС д-р Питер Пиот. «Ни одно другое заболевание не препятствует въезду людей в другие страны для целей бизнеса, туризма или для участия в совещании. Ни одно другое заболевание не заставляет людей опасаться, что на границе в их багаже будут искать медицинские препараты, в результате чего им не разрешат въезд или хуже того, задержат и затем депортируют обратно в свою страну» - добавил он.
Признавая, что охрана государственной границы и вопросы иммиграции относятся к суверенному праву отдельных государств, национальные законы и постановления, тем не менее, должны обеспечивать, чтобы люди, живущие с ВИЧ, не подвергались дискриминации в отношении своей способности равноправно участвовать в международном передвижении, искать возможность въехать в страну, которая не является их собственной, или остаться в этой стране. В Международных руководящих принципах по ВИЧ/СПИДу и правам человека указывается, что любое ограничение свободы передвижения или выбора постоянного места жительства на основе только предполагаемого или реального ВИЧ-статуса, включая скрининг на ВИЧ лиц, совершающих международные поездки, является дискриминацией.
Помимо того, что ограничения на поездки являются дискриминационными, они не имеют никакого обоснования с точки зрения общественного здоровья. ВИЧ не должен рассматриваться в качестве состояния, которое представляет собой угрозу для общественного здоровья в связи с поездкой, так как, хотя он и является инфекционным, вирус иммунодефицита человека не может передаваться в результате простого нахождения лица с ВИЧ в стране или через случайный контакт.
На деле, ограничительные меры могут идти вразрез с интересами в области общественного здоровья, поскольку изоляция ВИЧ-положительных людей, не являющихся гражданами страны, усиливает атмосферу стигмы и дискриминации против людей, живущих с ВИЧ, и таким образом могут лишать и граждан, и неграждан желания пользоваться услугами по профилактике и уходу в связи с ВИЧ. Кроме того, ограничения на поездки могут способствовать тому, что граждане данной страны начнут считать ВИЧ «заграничной проблемой», которая решена путем недопущения иностранцев в страну, так что они могут не видеть никакой надобности в том, чтобы самим практиковать безопасное поведение.
Ограничения на поездки не имеют и экономического обоснования. Люди, живущие с ВИЧ, могут сейчас вести долгую и продуктивную трудовую жизнь, и это заставляет менять экономические доводы в пользу огульных ограничений: обеспокоенность тем, что мигранты опустошают медицинские ресурсы, должна уравновешиваться их потенциальным вкладом. Кроме того, продолжающееся расширение программ лечения в направлении обеспечения всеобщего доступа к 2010 году и устойчивое снижение стоимости лечения в странах с низким и средним уровнем доходов разрушают миф о том, что поездки ВИЧ-положительных лиц резко поднимут расходы систем здравоохранения за рубежом.
Создание международной целевой группы по ограничениям на поездки в связи с ВИЧ является критически важной возможностью повысить внимание к проблеме ограничений на поездки в связи с ВИЧ на международном и национальном уровне и шагом в направлении их устранения.
Разработка конкретных рекомендаций для позитивных перемен

Целевая группа подготовит реальные
рекомендации в отношении конкретных
действий, которые различные
заинтересованные стороны могут
осуществить в целях продвижения к
устранению ограничений на поездки в
связи с ВИЧ.
Международная целевая группа состоит из двух рабочих групп, которые занимаются краткосрочными и долгосрочными ограничениями, при поддержке и руководстве со стороны Руководящего комитета. Рабочие группы и Руководящий комитет Целевой группы проведут четыре совещания до августа 2008 года, когда на Международной конференции по СПИДу в Мексике будут представлены их окончательные рекомендации. Целевая группа подготовит реальные рекомендации в отношении конкретных действий, которые различные заинтересованные стороны (правительства, гражданское общество, межправительственные организации и частный сектор) могут осуществить в целях продвижения к устранению ограничений на поездки в связи с ВИЧ. Целевая группа будет концентрировать внимание на ключевых стратегических действиях, которые:
-
повышают внимание к проблеме ограничений на поездки в связи с ВИЧ на международном, региональном и национальном уровне;
-
воздействуют на правительства в странах, имеющих ограничения на поездки в связи с ВИЧ, касающиеся въезда и краткосрочного пребывания, с целью снять такие ограничения; и
- активизируют более долгосрочную деятельность по продвижению к устранению всех ограничений на поездки в связи с ВИЧ.
При разработке этих рекомендаций Руководящему комитету будут оказывать поддержку рабочие группы, которым будет предложено осуществить:
- критическое картирование нынешней ситуации, касающейся применения краткосрочных и долгосрочных ограничений на поездки в связи с ВИЧ;
-
анализ препятствий на пути устранения различных видов ограничений на поездки в связи с ВИЧ и возможных действий со стороны различных национальных и международных заинтересованных участников с целью поддержать их устранение; и
- рекомендации в отношении лучшей практики, касающейся въезда и пребывания людей, живущих с ВИЧ, в различных условиях мобильности и миграции.
В рекомендациях будут поддержаны принципы недискриминации и расширения участия людей, живущих с ВИЧ, а также рациональная политика в связи с ВИЧ для путешествующих, мигрантов и мобильных групп населения в направляющих и принимающих странах – в контексте усилий по обеспечению всеобщего доступа к профилактике, лечению, уходу и поддержке в связи с ВИЧ, как это согласовано правительствами на Заседании высокого уровня по СПИДу (2006 год).
Международная целевая группа по ограничениям на поездки в связи с ВИЧ проведет свое следующее заседание 31 марта – 2 апреля в Женеве.
Ограничения на поездки в связи с ВИЧ
Ресорсы:
Политика и руководящие принципы:
Заявление ЮНЭЙДС/МОМ по ограничениям на поездки в связи с ВИЧ
Внешние ссылки:
16-е заседание Правления Глобального фонда – Подтверждение приверженности ЮНЭЙДС созданию целевой группы по ограничениям на поездки
(на английском языке)
Заявление по вопросам политики МОС
(на английском языке)
Европейская группа по лечению СПИДа
(на английском языке)
Мультимедия:
Слушать: Шона Меллорс, старший технический советник, права человека, Международный альянс по ВИЧ/СПИДу
(на английском языке)
Слушать: Грасия Виолета Росс Кирога, общенациональный председатель, Боливийская сеть людей, живущих с ВИЧ/СПИДом
(на английском языке)
Related
 People living with HIV in Kyrgyzstan have won the right to adopt
People living with HIV in Kyrgyzstan have won the right to adopt
12 февраля 2021 года.
 Raising the voices of women at the forefront of climate change
Raising the voices of women at the forefront of climate change
05 мартаа 2020 года.
 Mapping HIV laws and policies
Mapping HIV laws and policies
31 июля 2019 года.
Feature Story
Health workforce crisis limits AIDS response
29 февраля 2008
29 февраля 2008 29 февраля 2008The Global Health Workforce Alliance (GHWA) is convening the first ever Global Forum on Human Resources for Health in Kampala, Uganda from March 2-7, 2008.
The GHWA, hosted and administered by the World Health Organization (WHO), has been created to identify and implement solutions to the health workforce crisis. What is this crisis and how does it impact on the AIDS response?
Healthcare systems depend on trained staff
One of the major obstacles identified to scaling up access to HIV prevention, treatment, care and support in a country is a weak national healthcare system.
The question of human resources for health is a critical factor in any effective response to AIDS. A shortage of trained health care workers, particularly in low and middle-income countries, presents a real challenge to the ability of a country to respond to the HIV prevention, treatment and care needs of their populations.
In parts of sub-Saharan Africa shortages are so acute that they limit the potential to scale up programmes aimed at achieving health-related Millennium Goals including the roll-out of treatment for AIDS. - World Health Assembly, 2005
WHO estimates that more than 4 million additional doctors, nurses, midwives, managers and public health workers are urgently needed to avert serious crises in health-care delivery in 57 countries around the world—26 of these in sub-Saharan Africa. WHO estimates that at least 1.3 billion people around the world lack access to even the most basic health care.
Insufficient human resources has been identified as a primary obstacle to the delivery of antiretroviral treatment and other HIV-related services in many countries in Eastern Europe, Africa and Asia. Many healthcare systems have poor availability and quality of pre- and post-test counselling, health education, home care, diagnosis and treatment of opportunistic infections.
Governments pledge to increase capacity
At the 2006 High Level Meeting on AIDS, UN Member States reaffirmed their commitment to fully implement the 2001 Declaration of Commitment on HIV/AIDS and further strengthened international commitment on AIDS by:
“Pledging to increase capacity of human resources for health, and committing additional resources to low- and middle-income countries for the development and implementation of alternative and simplified service delivery models and the expansion of community-level provision of comprehensive AIDS, health and other social services.” However translating government commitment to increasing capacity into more health workers on the ground is a challenge of some complexity.
Balancing macroeconomic stability and staff retention
While AIDS funding has increased in recent years, simply pouring this into the healthcare system of a country to strengthen capacity is not the solution.
Most economists agree that a high rate of growth of a money supply causes a high rate of inflation - a rise in the general level of prices of goods and services in a given economy over a period of time.
Governments believe that fiscal and monetary policies – to keep inflation low - are needed to control and manage their economy to prevent potentially damaging sharp shocks and fluctuation in growth.
Low-income countries with high HIV-prevalence have to juggle the need to invest in their healthcare systems with a responsibility to maintain macroeconomic stability – nationally and regionally.
These economic policies include keeping salaries low and so constrain the hiring of the doctors, nurses, community health-care workers. Low salaries lead to low worker morale and low productivity and make it extremely difficult for some countries to retain their staff.
Open labour markets mean skilled professionals are migrating in record numbers to high-income countries, draining human capacity where it is most needed.
Global Forum on Human Resources for Health
Consensus is growing that this is a global crisis which calls for coordinated action.
The Global Health Workforce Alliance (GHWA) has been established to explore and implement solutions to this health workforce crisis. It is hosted and administered by the World Health Organization (WHO).
As a first step in the process, the GHWA are holding the first Global Forum on Human Resources for Health in Kampala this week. This meeting brings together government leaders, health and development professionals, civil society and academics from around the world who hope to consolidate a global movement on this.
Participants will explore solutions to improving education, training, and health sector management as well as looking at recent trends in migration.
Health workforce crisis limits AIDS response
Cosponsors:
WHO - Global Health Workforce Alliance
External links:
First Global Forum on Human Resources for Health 2-7 March 2008, Kampala, Uganda
Publications:
Scaling up access to HIV prevention, treatment, care and support: The next steps (UNAIDS, 2006)
Global Health Workforce Alliance Strategic Plan (WHO)
Related
Review recommends law reform on HIV testing to help Angola reduce new HIV infections among young people and ensure treatment
11 мая 2022 года.
Report highlights that women and marginalized people need urgent access to health-care services in Ukraine
11 мая 2022 года.
Key considerations to integrate HIV and mental health interventions
28 апреля 2022 года.
Feature Story
Providing community care in India
28 февраля 2008
28 февраля 2008 28 февраля 2008
While in India Executive Director Dr Peter
Piot visited Sewa Ashram—a centre that
provides essential healthcare, support and
vocational training.
While in India Executive Director Dr Peter Piot visited Sewa Ashram—a centre that provides essential healthcare, support and vocational training.
In 1996 while driving through one night in Delhi, Ton Snellaert saw a man lying in the street. Driving on he saw hundreds more people sleeping by the roadside. The experience motivated him to set up a centre in one of Delhi’s northern suburbs and a year later the ‘Delhi House’ opened. In its first year, the small 12 room centre welcomed 45 people with care and support. Since then more than 3,000 have come through its doors and it is now better known as ‘Sewa Ashram’. Sewa is a Hindi word which means 'the practice of selfless service' and ashram means 'spiritual community'.
The clinic, staffed by three nurses and a medical doctor, offers free medical care and confidential TB and HIV counselling and testing. The centre has continued to grow and now offers TB treatment, a children’s education programme and vocational training.

The clinic, staffed by three nurses and a
medical doctor, offers free medical care
and confidential TB and HIV counselling
and testing.
The Ashram has attracted volunteers from all over the world, brought together by the same passion for service. One of the volunteers is Kaye Kirsch who currently manages the Ashram. “Our community is based on compassion and focuses on restoring dignity while giving love and good healthcare to those that need it the most,” says Kaye Kirsch. “Many of our staff came through the doors in need of help and have chosen to stay at the centre and help others,” she adds.
Providing community care in India
Related links:
Related
 A rainbow of hope for LGBTQI+ people in rural Japan
A rainbow of hope for LGBTQI+ people in rural Japan
17 мая 2023 года.
 Thailand’s Mplus: HIV services delivered in style
Thailand’s Mplus: HIV services delivered in style
13 декабря 2022 года.
 Preventing transmission and tackling stigma: The power of U=U
Preventing transmission and tackling stigma: The power of U=U
12 декабря 2022 года.
Feature Story
MDR-TB more common in people living with HIV
28 февраля 2008
28 февраля 2008 28 февраля 2008
According to the 4th World Health Organization (WHO) report on anti-tuberculosis drug resistance released on 26 February, multi-drug resistant tuberculosis* (MDR TB) has been shown to be almost twice as common in tuberculosis (TB) patients living with HIV compared to TB patients without HIV.
The report presents the findings of the largest survey of TB drug resistance to date with information collected between 2002 and 2006 from 90,000 TB patients in 81 countries. It demonstrates the highest rates of MDR-TB ever recorded with nearly half a million new cases of MDR-TB worldwide each year––around 5% of the total 9 million new TB cases. It also found that extensively drug-resistant tuberculosis** (XDR-TB), a virtually untreatable form of the respiratory disease, has been recorded in 45 countries.
The true scale of the problem also remains unknown in some pockets of the world. Only six countries in Africa—the region with the highest incidence of TB in the world***––were able to provide drug resistance data for the report, and none of these were able to provide information on drug resistance in people living with HIV. Other countries in the region could not conduct surveys because they lack the equipment and trained personnel needed to identify drug-resistant TB.
‘This report confirms the serious threat that drug resistant TB poses to people living with HIV,’ said Alasdair Reid HIV/TB Adviser, UNAIDS. ‘UNAIDS, together with WHO and our international partners, is working with TB and HIV programmes in countries across the world to ensure they work more closely together to prevent the development and spread of drug-resistant TB among people living with HIV through better diagnosis and treatment of TB in people living with HIV and improved TB infection control in HIV care settings and communities affected by HIV’.
WHO estimates that US$ 4.8 billion is needed for overall tuberculosis control in low- and middle-income countries in 2008, with US$ 1 billion needed to respond to drug resistant tuberculosis. There is currently a gap in financing of US$ 2.5 billion, including a US$ 500 million gap for drug resistant tuberculosis.
NOTE TO EDITORS:
* The bacteria responsible for TB becomes resistant when people who are ill with TB are not provided with or do not complete a full course of medication. Drug-resistant TB, like drug-sensitive TB, can also be transmitted through the air from an infected person to a non-infected person. MDR-TB is a form of TB that does not respond to the standard six month treatment using first line-drugs (i.e. resistant to isoniazid and rifampicin). It can take two years to treat with drugs that are 100 times more expensive than first-line treatment.
** XDR-TB is a form of TB caused by bacteria resistant to virtually all the most effective anti-tuberculosis drugs (i.e. MDR-TB plus resistance to any fluoroquinolones and any one of the second-line anti-tuberculosis injectable drugs: amikacin, kanamycin or capreomycin).
*** In sub-Saharan Africa HIV is dramatically fuelling the spread of TB which is a major cause of death among people living with HIV. MDR-TB and XDR-TB are highly lethal in people living with HIV––studies show case fatality rates of over 90%. Drug-resistant TB is therefore a major threat to the effectiveness of both TB treatment and anti-retroviral treatment programs.
MDR-TB more common in people living with HIV
Cosponsors:
Related links:
Publications:
Anti-tuberculosis drug resistance in the world (pdf, 2.4 Mb)
Related
 United for ending cervical cancer, HIV and inequities for women and girls
United for ending cervical cancer, HIV and inequities for women and girls
17 ноября 2022 года.
 Delays in global, affordable access to long-acting, injectable HIV medicines would cost lives, say AIDS campaigners
Delays in global, affordable access to long-acting, injectable HIV medicines would cost lives, say AIDS campaigners
16 ноября 2022 года.
Key considerations to integrate HIV and mental health interventions
28 апреля 2022 года.
Feature Story
Microbicides 2008 concludes in India
27 февраля 2008
27 февраля 2008 27 февраля 2008
The biannual international microbicides
conference “Microbicides 2008” ran 24 –
27 February in New Delhi under the
theme “Striving towards HIV Prevention”.
Credit: Microbicides 2008
The biannual international Microbicides 2008 conference concluded Wednesday 27 February in New Delhi.
The scientific and networking conference was opened on Sunday by the Union Minister for Health and Family Welfare, Dr Anbumani Ramadoss.
More than 1,100 researchers, public health workers, communities and advocacy organizations gathered for the four-day meeting to discuss current research and development of a safe, effective and accessible microbicide which women could use to prevent the transmission of HIV and other sexually transmitted infections.
The meeting took place in the context of a year of mixed results in candidate microbicide clinical trials. A cellulose sulfate trial was stopped early due to safety concerns, while Carraguard, a candidate microbicide which completed large-scale Phase III trials, was found to be safe but not effective in preventing HIV transmission. These results were unexpected but all findings shed more light onto the research avenues.
The event ended on a positive and hopeful note. Addressing the closing ceremony, UNAIDS Executive Director Dr Peter Piot acknowledged the difficult time it has been for microbicide research but focused on the progress made in the field so far.
Emphasizing the importance of rising above these challenges and huge value of overcoming them, Dr Piot said in his speech, “Developing an effective microbicide will be a critical step forward in the AIDS response. To provide women with HIV prevention technology they can use themselves will be nothing short of revolutionary.”
The conference programme was overseen by an international scientific advisory committee and included plenary sessions, presentations of original research, round table discussion sessions, symposia and satellite meetings and poster sessions and exhibitions. A broad range of topics were discussed in four simultaneous tracks.

Dr Piot said in his speech that “Developing
an effective microbicide will be a critical
step forward in the AIDS response. To
provide women with HIV prevention
technology they can use themselves will
be nothing short of revolutionary.”
In the Basic Science track, topics included updates on the microbicide pipeline of current and emerging candidates, latest understanding of HIV sexual transmission, drug discovery, advances in formulations.
In the Clinical track lessons learned from cohort studies were explored as well as findings from Phase I, II and III Trials. Amongst other topics was the impact of other HIV prevention trials.
The Social Science track looked at behavioral and social science research tools, acceptability, lessons from managing the closure of multi-country HIV prevention trials and the role of men in microbicide use.
Under Community and Advocacy, many aspects of community engagement in trials were considered including managing stakeholder expectations of trial results and the importance of partnerships for HIV research.
Several cross-track discussions were also held, exploring challenges, experiences and lessons learned.
It is the first time that the meeting has taken place in the Asian region. Previous meetings have been held at Washington DC in 2000, Antwerp in 2002, London in 2004, and Cape Town in 2006. Each occasion takes researchers and activists further in their understanding of the challenges of microbicide development.
For all present this week in New Delhi, it is hoped that by the time of the next meeting in 2010, we will have turned a real corner on the road to delivery of a safe, effective and accessible microbicide which could make a difference to women’s lives.
For more information visit the Microbicides 2008 conference web site at http://www.microbicides2008.com/
Microbicides 2008 concludes in India
Partners:
Global Coalition on Women and AIDS
Global Campaign for Microbicides
Alliance for Microbicide Development
International Partnership for Microbicides (IPM)
Feature stories:
Microbicides: Why are they significant? (Part 1) (20 February 2008)
Microbicides: challenges to development and distribution (Part 2) (22 February 2008)
External website:
Related
A rainbow of hope for LGBTQI+ people in rural Japan
17 мая 2023 года.
Thailand’s Mplus: HIV services delivered in style
13 декабря 2022 года.
Preventing transmission and tackling stigma: The power of U=U
12 декабря 2022 года.
Feature Story
UNAIDS Executive Director receives prestigious humanitarian award
26 февраля 2008
26 февраля 2008 26 февраля 2008
President of the Catholic Bishop’s Conference of India, Cardinal Telesphore P. Toppo presents UNAIDS Executive Director, Dr Peter Piot the “Blessed Mother Teresa International Humanitarian Award” at a ceremony held on 26 February 2008 in New Delhi, India.
The first ever ‘Blessed Mother Teresa International Humanitarian Award’ has been awarded to Dr Peter Piot, Executive Director of UNAIDS for the ‘significant impact he has made to the lives of people living with HIV in the developing world’.
Dr Piot was presented with the award by Cardinal Telesphore Toppo, President of the Catholic Bishop’s Conference of India at a special ceremony held in New Delhi on 26 February 2008. He will share the award with Ambassador Mark Dybul, the US Global AIDS Coordinator, who will be presented with his award during the Mother Teresa Memorial Annual Oration to be held at the Indira Gandhi National University on 3 March.
The award was established by the Health Commission of the Catholic Bishop’s Conference of India to recognise the work of dedicated individuals demonstrating similar humanitarian concerns to those of Mother Theresa herself.
 (From left): Mission Director, U.S. Agency for International Development (USAID) Dr George Deikun; President of the Catholic Bishop’s Conference of India, Cardinal Telesphore P. Toppo; UNAIDS Executive Director, Dr. Peter Piot; Executive Secretary, Commission for Health of the Catholic Bishops' Conference of India, Fr Alex Vadakumthala.
(From left): Mission Director, U.S. Agency for International Development (USAID) Dr George Deikun; President of the Catholic Bishop’s Conference of India, Cardinal Telesphore P. Toppo; UNAIDS Executive Director, Dr. Peter Piot; Executive Secretary, Commission for Health of the Catholic Bishops' Conference of India, Fr Alex Vadakumthala.Speaking at the award ceremony, Dr Piot said, “I accept this award as a recognition of the contribution of the whole United Nations family, and in particular by colleagues at UNAIDS, who work for the values closest to Mother Theresa’s heart – service to those in need. We are indeed driven by the ideals which she promoted through her life and her work which was marked by tolerance, compassion and inclusiveness.”
Dr Piot commended the Indian Catholic Church for its engagement in the AIDS response and support for people living with HIV continuing Mother Teresa's tradition of compassion and respect.
Blessed Mother Teresa of Calcutta was the Albanian-born founder of the Order of the Missionaries of Charity—a Catholic Congregation of women dedicated to helping the poor in India. She lived as a simple nun who touched the hearts of many and in 1979 received the Nobel Prize for Peace.
UNAIDS Executive Director receives prestigious hu
External links:
Related
A rainbow of hope for LGBTQI+ people in rural Japan
17 мая 2023 года.
Thailand’s Mplus: HIV services delivered in style
13 декабря 2022 года.
Preventing transmission and tackling stigma: The power of U=U
12 декабря 2022 года.
Feature Story
Microbicides: challenges to development and distribution (Part 2)
21 февраля 2008
21 февраля 2008 21 февраля 2008The biannual international microbicides conference “Microbicides 2008” will run 24 – 27 February in New Delhi under the theme “Striving towards HIV Prevention”.
The gathering will enable knowledge-sharing between microbicide researchers, public health workers and advocacy organizations and will provide a forum for the discussion of new developments in microbicide research including basic science, clinical trials and social science issues as well as discussion on behaviour, community engagement and advocacy.
In the second of a two part series looking at microbicides, we will be exploring some of these topics.
For several years, UNAIDS has insisted that the development of an effective microbicide is a public health priority and has emphasized the importance of access and affordability. However due to a lack of significant investment, the research and development pipeline has been slow and inefficient.
UNAIDS Executive Director, Dr Peter Piot said, “ The international community, including the private sector, must continue to invest in effective HIV prevention technologies that can be used by women .”
“Ensuring access to safe and effective microbicides will be of critical importance to all our prevention efforts and to our goal of stopping and reversing the epidemic.”
The cost of saving lives
The total global funding for microbicide research and development in 2006 done by the non-commercial sectors was $217 million. The pharmaceutical sector chooses to invest into the search for new antiretroviral drugs, attracted by a potentially large return-on-investment.
If there was comparable investment into microbicide research, it is thought that a safe and effective product would be on the market much sooner than a vaccine. However, as any microbicide would have to be affordable to consumers to whom it would make most difference – women living in low- and middle-income countries – the profit margins would be low. This economic reality makes microbicide research a less attractive investment.
As a consequence virtually all microbicide research is conducted by small biotech companies funded by the public sector.
Research and development pipeline
Research and development is continuing in spite of the large funding gap. More investment will be needed to bring clinical trials to completion and lay groundwork for distribution of an effective product.
As with any new drug, candidate microbicides must pass a series of rigorous laboratory tests and then a series of human clinical trials.
| What are the different phases of a clinical trial? Phase I clinical trials are the first stage of testing in humans and are designed to evaluate safety. Normally the trials are conducted in an inpatient clinic, where volunteers can be monitored closely. A group of 20-80 healthy volunteers will use the product for 1–2 weeks. Once the initial safety of the study drug has been confirmed in Phase I trials, Phase II trials are performed on larger groups of 20-300 and are designed to assess how well the product works, as well as to continue safety and tolerability assessments in a larger group of volunteers over 6–18 months. When the development process for a new drug fails, this usually occurs during Phase II trials when the drug is discovered to show no evidence of potential effect, or found to have toxic effects. Phase III studies are randomized controlled multi-centre trials on large groups (300–3,000 or more) and are aimed at being the definitive assessment of how effective and safe the drug is. Because of their large size and duration (1–2 years), Phase III trials are the most expensive, time-consuming and difficult trials to design and run. |
A range of contraceptive and non-contraceptive microbicide products are currently in different phases of development and trial including over 30 candidates in clinical trials. More than 30 others are in pre-clinical testing. However, results to date have been disappointing.
The microbicide search had an unexpected setback in February 2007 when an advanced Phase III study of a candidate microbicide Cellulose Sulfate was stopped early because women who used the gel were suspected to have a higher risk of HIV infection compared with women in the placebo group.
Earlier this week it was announced that Carraguard, a candidate microbicide that had completed large-scale Phase III trials, was unable to prevent HIV transmission. Encouragingly the product was found to be safe for long-term vaginal use making it the first microbicide Phase III trial to be completed without safety concerns. Researchers are hopeful this is a finding which will be built on.
“The next generation of antiretroviral-based microbicide products holds much promise. We do need to develop better safety biomarkers and improve measurements of adherence and we can learn much more from trials which have not resulted in an effective product,” said UNAIDS Chief Scientific Adviser, Dr Catherine Hankins.
Timing of microbicide availability
The Global Campaign for Microbicides estimated that if one of the products in advanced clinical trials proves to be effective, a microbicide could be ready for distribution in a small number of countries by the end of 2010. However, if the current sets of products do not prove effective, the timeline will be longer.
| Ethical considerations Advocates and civil society work hard to ensure that as the science proceeds, the rights and interests of trial participants and their communities are protected. In microbicide trials all women are provided with a comprehensive HIV prevention package including counselling on condom use and safe sex, supplies of free, high quality condoms and regular screening for HIV and other sexually transmitted infections. Well-run trials are vital to women’s positive perception of trial participation – participants have expressed the importance of having access to information, being treated with respect, having an opportunity to be listened to, access to HIV testing and counselling and access to condoms. It is also vital that trial designs take into account local social and community perceptions of HIV, health and sex and that participants who become HIV-positive during or after the trials have access to care and support services. UNAIDS and AVAC have published “Good participatory practice guidelines for biomedical HIV prevention trials” which sets out ten principles for community engagement throughout the research life cycle. International consensus has been reached and detailed in 1 9 guidance points on a range of topics including confidentiality, informed consent, control groups and potential harms, in the recently published UNAIDS/WHO guidance document “Ethical considerations in biomedical HIV prevention trials” |
Next steps
Next week’s Microbicide conference will be an important forum for the discussion of the challenging issues of research, financing, clinical trials and ethical considerations.
Experts will gather to hear updates on current and emerging candidate product trials and will debate a range of topics. UNAIDS Chief Scientific Adviser Dr Catherine Hankins will make presentations on the implications of the results of male circumcision trials for microbicide research and present findings from the December 2007 consultation “Making HIV trials work for women and adolescent girls”.
UNAIDS Executive Director Dr Peter Piot will address the conference closing ceremony which will be attended by politicians, policy-makers, scientists, community activists and other AIDS experts.
The London School of Hygiene and Tropical Medicine estimated by mathematical modelling that the introduction of even a 60% effective microbicide into the world’s 73 lowest-income countries which would be used by only 20% of women already in contact with health services could avert up to 2.5 million infections in three years.
With many observers confident that a successful microbicide could make a significant impact in HIV prevention around the globe, the wait is all the more frustrating, the set-backs all the more disappointing.
Microbicides: challenges to development and distr
Cosponsors:
Feature stories:
Microbicides: Why are they significant? (Part 1) (20 January 2008)
Making HIV trials "work for women" (12 December 2007)
Women and HIV research - report from meeting (11 December 2007)
Experts meet on women and HIV trials (part III of three-part series) (07 December 2007)
The role of women in HIV trials (part II of three-part series) (05 December 2007)
Meeting ethical concerns over HIV trials (part I of three-part series) (03 December 2007)
Funding estimates for AIDS research and development (30 August 2007)
Multimedia:
Listen to UNAIDS Chief Scientific Adviser Dr Catherine Hankins on Microbicides 2008
External links:
Related
 “My life’s mission is to end stigma and discrimination, and that starts with U = U”: a story of HIV activism in Thailand
“My life’s mission is to end stigma and discrimination, and that starts with U = U”: a story of HIV activism in Thailand
01 мартаа 2022 года.
 Science, HIV and COVID-19—where are we headed?
Science, HIV and COVID-19—where are we headed?
08 июня 2021 года.
 How was a COVID-19 vaccine found so quickly?
How was a COVID-19 vaccine found so quickly?
09 февраля 2021 года.
Feature Story
Journal of Internal Medicine: Review article by L. O. Kallings
21 февраля 2008
21 февраля 2008 21 февраля 2008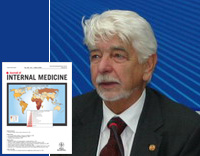
Professor Lars O. Kallings is also UN Special Envoy for AIDS in Eastern Europe and Central Asia
The March issue of the Journal of Internal Medicine published today features a review article by Professor Lars O. Kallings entitled “The first postmodern pandemic: 25 years of HIV/ AIDS”.
In the 26-page article Professor Kallings gives a biomedical overview of AIDS looking into the characteristics of AIDS and the scientific search for preventative technologies. He traces the changing epidemiology of HIV from its earliest reports to today’s incidence and distribution in different regions of the globe. The varied social and political aspects of AIDS and the global response to it are also examined.
The review explores disinformation and misconceptions around the issue of AIDS and discusses prospects of finding a cure and other future scenarios.
Professor Lars O. Kallings was appointed UN Special Envoy for AIDS in Eastern Europe and Central Asia by the UN Secretary-General in May 2003.
Engaged in the AIDS response for over 20 years, he has held positions including adviser to the World Health Organization, Chairman of the Global Commission on AIDS and Senior Adviser to the Global Programme on AIDS on Scientific and Policy Affairs. He is currently honorary Chairman of AIDS Accountability International. He is Founding President of the International AIDS Society (IAS) and was its Secretary-General 1994–2002.
Professor Kallings wrote this review as an independent scientist and its content does not necessarily represent the views of the UN or any organization to which the author is, or has been, affiliated.
Journal of Internal Medicine: Review article by L
Feature stories:
Professor Lars Kallings’ advocacy visit to Belarus (October 2006)
External links:
Publications:
The first postmodern pandemic: 25 years of HIV/ AIDS - L. O. Kallings (2008)
Journal of Internal Medicine, Volume 263 Issue 3 Page 218-243, March 2008
Related
 The Caribbean, answering the global call to end stigma and discrimination
The Caribbean, answering the global call to end stigma and discrimination
11 апреля 2014 года.
 Walk in my shoes — UNAIDS Board devotes key session to HIV, adolescents and youth
Walk in my shoes — UNAIDS Board devotes key session to HIV, adolescents and youth
20 декабря 2013 года.
 Know your HIV status: First European testing week takes off
Know your HIV status: First European testing week takes off
27 ноября 2013 года.