
Feature Story
Integrating the AIDS response with broader health and development agendas
10 June 2011
10 June 2011 10 June 2011
Ms. Francoise Barré-Sinoussi, Nobel Lauréate, Institut Pasteur, France; Ms. Aditi Sharma, International Treatment Preparedness Coalition; at Panel 5: Integrating the HIV AIDS Response with Broader Health and Development Agendas, held at UN Headquarters, NYC, on June 10, 2011.
UNAIDS/B. Hamilton
Taking AIDS out of isolation and into integration was the focus of the final official panel discussion on the closing day of the UN General Assembly High Level Meeting on AIDS.
Chaired by His Excellency the Second Vice-President of Burundi Gervais Rufyikiri, the panel was moderated by Laurie Garrett Senior Fellow for Global Health at the Council for Foreign Relations and brought together Nobel lauréate Francoise Barre-Sinoussi from the Institut Pasteur; civil society representative Aditi Sharma from the International Treatment Preparedness Coalition; UN Secretary General’s Special Envoy to Stop TB Jorge Sampaio and Norwegian State Secretary for Health State Secretary Ragnhild Mathisen.
Linking HIV to health and development
Thirty years into the HIV epidemic, AIDS has become an integral part of countries’ health and development challenges. But we need to strengthen these links to achieve universal access and ensure sustainability of the HIV response. Panellists identified key benefits and core elements for integrating HIV with other health and development agendas and discussed how the strengths of the AIDS response can be leveraged to the benefit of these issues.
“HIV responses cannot operate in isolation. Further scale up requires functioning integrated health systems and communities that are empowered through access to essential rights and goods, including food, nutrition and basic education,” said Francoise Barre Sinoussi.
The panel highlighted the lessons from integration of HIV and tuberculosis (TB) programmes and services and discussed links with sexual and reproductive health services and maternal, newborn and child health services, including efforts to eliminate new HIV infections among children and keeping their mothers alive. Mr Sampaio made a passionate plea to implement the recommended package of integrated TB/HIV services in order to prevent one million TB deaths in people living with HIV by 2015.
It was also noted that, as access to antiretroviral therapy expands, the HIV response is evolving from a disease-specific emergency response to a chronic disease management challenge which needs to be addressed within the context of other chronic health conditions. Many countries with a high HIV prevalence are also facing burgeoning epidemics of other chronic infections, such as Hepatitis B and C, and non-communicable diseases (NCD), such as cardio-vascular and chronic respiratory diseases and diabetes.
The panel emphasized that the benefits of an integrated approach to TB and HIV service-delivery to patients, programmes and partners are reflected in better access to comprehensive care, cost savings and reduced morbidity and mortality. Brazil’s combined approach to HIV and Hepatitis C was cited as an example of integrated, client centred approach. Similarly, the prevention of mother-to-child transmission of HIV—including treatment and care for mothers and their children—was highlighted as an integral and critical components to achieve Millennium Development Goal (MDG) 4 and MDG 5 and the UN Secretary-General’s ‘Global Strategy for Women’s and Children’s Health’.
The time is right, concluded the panel, to explore ways in which the scale up of HIV prevention, treatment, care and support may be leveraged to strengthen not only high-quality health services during specific periods of life—such as pregnancy and childhood—but responses to a range of other health conditions and development challenges development issues for example food security, poverty, drug dependence, human rights and gender. Mitigating the impact of HIV is therefore essential to achieving MDG 6 and other development goals.
Watch the event
External links
External links
Publications
Publications
Related
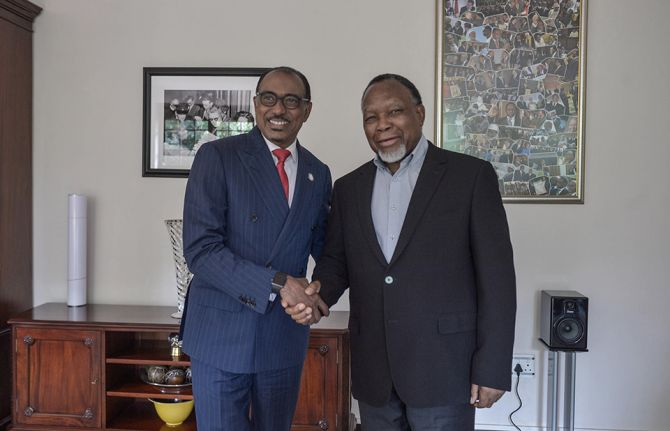 Keeping up the momentum in the global AIDS response
Keeping up the momentum in the global AIDS response
24 April 2019
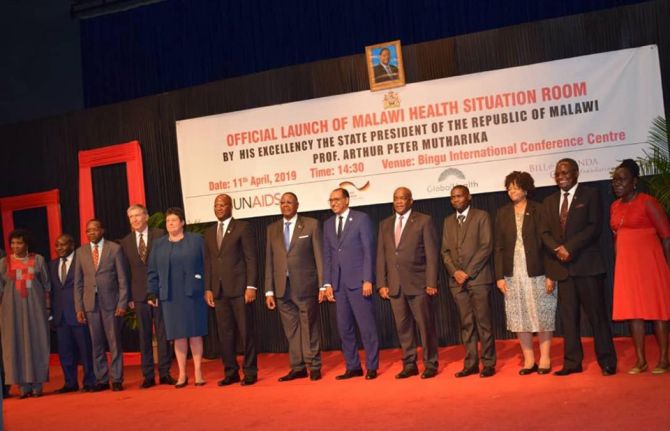 Malawi launches its health situation room
Malawi launches its health situation room
12 April 2019
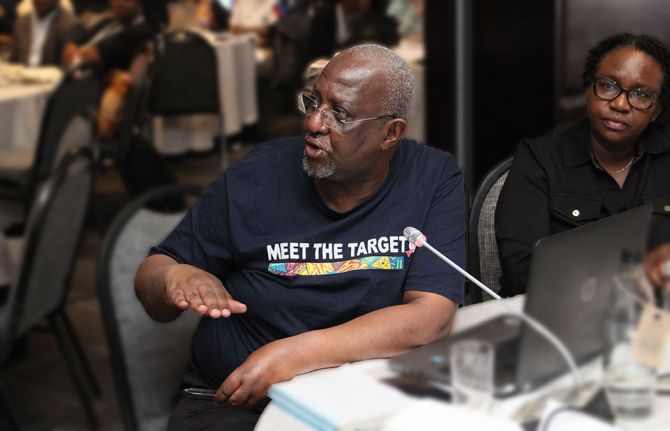
 Learning lessons on evaluation
Learning lessons on evaluation
02 April 2019
Press Release
World leaders launch plan to eliminate new HIV infections among children by 2015
09 June 2011 09 June 2011
(Left to Right): Michel Sidibé, UNAIDS Executive Director; President Bill Clinton; Ban Ki-moon, Secretary General of the UN; Goodluck Jonathan, President of Nigeria; Dr Eric Goosby, US Global AIDS Ambassador, Anthony Lake, UNICEF Executive Director, at launch of the Global Plan towards elimination of new HIV infections among children and keeping their mothers alive, at UN Headquarters, NYC, 9 June 2011.
Credit: UNAIDS/B. Hamilton
NEW YORK/GENEVA, 9 June 2011—World leaders gathered in New York for the 2011 United Nations High Level Meeting on AIDS have today launched a Global Plan that will make significant strides towards eliminating new HIV infections among children by 2015 and keeping their mothers alive.
“We believe that by 2015 children everywhere can be born free of HIV and that their mothers can remain healthy,” said Michel Sidibé, Executive Director of UNAIDS. “This new global plan is realistic, it is achievable and it is driven by the most affected countries.”
“Nearly every minute, a child is born with HIV. Working together, we can reverse this tide as we have done in the United States and they are very close to doing in Botswana,” said Ambassador Eric Goosby, the United States Global AIDS Coordinator. “Preventing new HIV infections among children across the globe is truly a smart investment that saves lives and helps to give children a healthy start in life.”
Providing pregnant women living with HIV with antiretroviral prevention and treatment reduces the risk of a child being born with the virus to less than 5%—and keeps their mothers alive to raise them. Neither technical nor scientific barriers stand in the way of responding to this global call to action. The plan notes that what is needed is leadership, shared responsibility and concerted action among donor nations, recipient countries and the private sector to make an AIDS-free generation a reality.
In answering the Global Plan’s call to action, the United States President's Emergency Plan for AIDS Relief (PEPFAR) announced an additional US$ 75 million to preventing mother-to-child transmission of HIV (PMTCT) efforts. This funding will be on top of the approximately US$ 300 million that PEPFAR already provides annually for PMTCT.
The Bill & Melinda Gates Foundation pledged US$ 40 million, Chevron committed to US$ 20 million and Johnson & Johnson pledged US$ 15 million.
"Investments in preventing mother-to-child transmission are greatly needed and the Bill & Melinda Gates Foundation is committed to ensuring that such initiatives are fully integrated into family planning and maternal, newborn, and child health programmes," said Stefano Bertozzi, Director of HIV and tuberculosis at the Foundation.
“Chevron understands that its sustainability as a business is inextricably linked to the health and well-being of its employees and the communities in which it operates,” stressed Rhonda Zygocki, Executive Vice President, Policy and Planning, for Chevron Corporation. “We are proud to pledge US$ 20 million, joining in this mission to eliminate mother-to-child transmission of HIV.”
“We have a dream that no baby will be born HIV positive and today’s pledge continues the Johnson & Johnson enduring commitment to eliminating mother-to-child transmission of HIV,” said Brian Perkins, Corporate Vice President, Corporate Affairs. “It is another step in fulfilling our commitment to support achievement of the Millennium Development Goals, and reflects our long-standing dedication to improving maternal and child health.”
In 2009, approximately 370 000 children were born with HIV—almost all of them in low- and middle-income countries, mainly in sub-Saharan Africa. Under the Global Plan, the goal would be to work toward reducing this number by 90% by 2015. All 22 of the countries with the highest burden of new HIV infections among children have contributed to the development of the plan and signed up to implement it.

(Left to Right): Babalwa Mbono, Representative of Women Living with HIV; Michel Sidibé, UNAIDS Executive Director; President Bill Clinton at launch of the Global Plan towards elimination of new HIV infections among children and keeping their mothers alive.
Credit: UNAIDS/B. Hamilton
The Global Plan towards the elimination of new HIV Infections among children by 2015 and keeping their mothers alive was developed by a group of more than 30 countries and 50 community groups, non-governmental and international organizations. The group was convened by UNAIDS and PEPFAR.
Babalwa Mbono found out she was HIV positive when she became pregnant. “Helping pregnant women to protect their babies is really important,” she said. “Like all mothers, I would do anything to give my child a healthy start in life—and this prevention should be available to women everywhere.”
"We can only achieve a generation free of HIV and AIDS by focusing our efforts on the mothers and children at greatest risk and in greatest need," urged UNICEF Executive Director Anthony Lake. "The investments we make in preventing maternal-to-child transmission of HIV—and in expanding more women's access to quality care—will yield tremendous returns, not only in the lives of children and families affected by HIV and AIDS, but in improving mothers' and children's health in the poorest countries that bear the greatest burden of the AIDS epidemic."
The plan focuses on a series of specific policy and programmatic measures which countries will take to ensure that all pregnant women living with HIV have access to HIV prevention and treatment services and that new HIV infections among children are eliminated by 2015. The plan also includes efforts to provide treatment to mothers and children living with HIV during breastfeeding and referral to ongoing HIV prevention and treatment programmes thereafter.
The key elements of the Global Plan include ensuring that:
- All women, especially pregnant women, have access to quality life-saving HIV prevention and treatment services—for themselves and their children.
- The rights of women living with HIV are respected and women, families and communities are empowered to fully engage in ensuring their own health and, especially, the health of their children.
- Adequate resources—human and financial—are available from both national and international sources in a timely and predictable manner while acknowledging that success is a shared responsibility.
- HIV, maternal health, newborn and child health and family planning programmes work together, deliver quality results and lead to improved health outcomes.
- Communities, in particular women living with HIV, are enabled and empowered to support women and their families to access the HIV prevention, treatment and care that they need.
- National and global leaders act in concert to support country-driven efforts and are held accountable for delivering results.
The plan also includes a detailed timetable for action at community, national, regional and global levels to ensure rapid progress towards elimination of new HIV infections in children by 2015 and keeping their mothers alive.
About the Global Plan
This Global Plan provides the foundation for country-led movement towards the elimination of new HIV infections among children and keeping their mothers alive. The Global Plan was developed through a consultative process by a high level Global Task Team convened by UNAIDS and co-chaired by UNAIDS Executive Director Michel Sidibé and United States Global AIDS Coordinator Ambassador Eric Goosby. It brought together 30 countries and 50 civil society, private sector, networks of people living with HIV and international organizations to chart a roadmap towards achieving this goal by 2015.
This plan covers all low- and middle-income countries, but focuses on 22 countries [1] with the highest estimate of HIV-positive pregnant women. Exceptional global and national efforts are needed in these countries that are home to nearly 90% of pregnant women living with HIV in need of services. Intensified efforts are also needed to support countries with low HIV prevalence and concentrated epidemics to reach out to all women and children at risk of HIV. The Global Plan supports and reinforces the development of costed, country-driven national plans.
UNAIDS
UNAIDS, the Joint United Nations Programme on HIV/AIDS, is an innovative United Nations partnership that leads and inspires the world in achieving universal access to HIV prevention, treatment, care and support. Learn more at unaids.org.
PEPFAR
The U.S. President's Emergency Plan for AIDS Relief (PEPFAR) is the U.S. Government initiative to help save the lives of those suffering from HIV/AIDS around the world. This historic commitment is the largest by any nation to combat a single disease internationally, and PEPFAR investments also help alleviate suffering from other diseases across the global health spectrum. PEPFAR is driven by a shared responsibility among donor and partner nations and others to make smart investments to save lives. Learn more at www.pepfar.gov.
[1] Angola, Botswana, Burundi, Cameroon, Chad, Côte d’Ivoire, Democratic Republic of the Congo, Ethiopia, Ghana, India, Kenya, Lesotho, Malawi, Mozambique, Namibia, Nigeria, South Africa, Uganda, United Republic of Tanzania, Swaziland, Zambia and Zimbabwe.
Contact
UNAIDS GenevaSophie Barton-Knott
tel. +41 22 791 1697
bartonknotts@unaids.org
Office of the U.S. Global AIDS Coordinator
U.S. Department of State
tel. +1 202 663 2708
PetersonJL@state.gov
Press centre
Download the printable version (PDF)
Feature Story
Call for leaders to champion the needs of women and girls in HIV policy and programming
10 June 2011
10 June 2011 10 June 2011.jpg)
Thematic panel discussion, “Women, Girls, and HIV”, which focuses on the disproportionate burden of HIV that is carried by women and girls around the world. (Left to right): Stephanie Nolan, journalist at the “Globe and Mail”; Hanno Pevkur, Minister of Social Affairs for Estonia; and Dr Aaron Motsoaledi, Minister of Health for the Republic of South Africa. UN Headquarters in New York, 9 June 2011
Credit: UN Photo/Eskinder Debebe
Women, girls and HIV was the theme of a high level panel which was held at the United Nations on Thursday 9 June. The event, which forms part of the UN General Assembly High Level Meeting on AIDS, was chaired by Hanno Pevkur, Minister of Social Affairs, Estonia.
The interactive discussion was moderated by Stephanie Nolen and the high level panel included Dr Aaron Motsoaledi, Minister of Health, Republic of South Africa; Dr Babatunde Osotimehin, Executive Director of UNFPA, represented the United Nations; and Siphiwe Hlophe, the co-founder of the non-governmental organization Swaziland for Positive Living.
“In 30 years of dealing with HIV,” explained Mr Pevkur, “we have learned that it is as much a social as a medical problem; and the lack of quality of sexual reproductive health and rights services, violence, harmful cultural practices, are fuelling the epidemic.”
We will not attain a sustainable response if we do not invest in women with education and economic empowerment
Siphiwe Hlophe, the co-founder of the non-governmental organization Swaziland for Positive Living
To explore the issue, the panellists and speakers from the floor responded to a series of questions and identified strategies that will help the HIV response to spark social transformation for women and girls to secure their human rights and protect themselves against HIV. They discussed ways to ensure that the specific needs and vulnerabilities of women and girls are adequately addressed in the response to HIV.
Unequal opportunities
In many societies, women face barriers in accessing HIV prevention, treatment, care and support services due to limited decision-making power, lack of control over financial resources, restricted mobility and unequal care responsibilities. Lack of education is another major barrier; around two-thirds of the world’s 796 million illiterate adults are women.
“We will not attain a sustainable response if we do not invest in women with education and economic empowerment,” said Ms Hlophe who highlighted need to engage communities including at the rural level so that all women are empowered. There was consensus that comprehensive sexuality education, which includes HIV education, is a key component of effective evidence-informed HIV prevention. Such education should be made available in a non judgemental, youth-friendly way, to adolescents and young people in and out of schools, and must include human rights and gender equality.
Challenge violence against women
One of the event findings was that stopping AIDS requires acting to stop violence against women at every level. “Violence against women is both a cause and a consequence of HIV,” said Minister Pevkur. The participants discussed how to better address the linkages between violence against women and girls and HIV as well as the social determinants that increase their vulnerability to HIV infection.
The risk of HIV among women who have experienced violence may be up to three times higher than those who have not. The prevalence of forced first sex among adolescent girls below 15 years ranges between 11% and 45% globally. Laws and policies that prevent and punish violence against women, including harmful traditional norms, and effective implementation, are paramount the speakers concluded.
Ensure access to comprehensive HIV and sexual and reproductive health services
There were calls for political leaders and stakeholders to champion “women- and girl- tailored” approaches in policy and programming. Another recommendation was the need to ensure that women in all their diversity, including adolescent girls and young women, have access to comprehensive HIV and sexual and reproductive health services, free of violence, discrimination, and coercion.
Uphold women’s human rights
It is crucial for governments to commit to fulfil all women’s human rights, including their sexual and reproductive health and rights. There is an urgent need for a clear target which views women in their entirety, across their lifespan, and not solely as mothers.
Invest in women and girls
The discussion also highlighted the need for greater and sustainable investment in the leadership of women and girls, as well as in strengthening women’s rights organizations and networks of women living with HIV, is needed to achieve the meaningful engagement of women and girls in the response to HIV
UN General Assembly High Level Meeting on AIDS
Thirty years into the AIDS epidemic, and 10 years since the landmark UN General Assembly Special Session on HIV/AIDS, the world has come together to review progress and chart the future course of the global AIDS response at the 2011 UN General Assembly High Level Meeting on AIDS from 8–10 June 2011 in New York. Member States are expected to adopt a new Declaration that will reaffirm current commitments and commit to actions to guide and sustain the global AIDS response.
External links
External links
Publications
Publications
- Backgrounder Panel 4: Women, girls and HIV (pdf, 186 Kb)


.")
Feature Story
Applying evidence for results: How can we effectively scale up HIV treatment?
10 June 2011
10 June 2011 10 June 2011
Agnes Binagwaho, Minister of Health, Rwanda at Ministerial Round Table Addressing Access: Taking Programmes to Scale. UN Headquarters, NYC, on June 9, 2011.
Credit: UNAIDS/B. Hamilton
With unprecedented high level participation at this week’s UN General Assembly Meeting on AIDS, with more thirty Heads of State and Government and Vice Presidents and some 100 ministers in attendance. A special side event was convened for the ministers to come together to share their experiences across the new landscape and outlook for HIV treatment, including treatment for prevention. It brought together ministers from a wide spectrum of sectors—including health, justice, social development and labour—with members of civil society, to exchange a diversity of country experiences.
Panellists in the session included Aaron Motsoaledi, Minister of Health, South Africa; José Angel Cordova Villalobos Secretary of Health, Mexico; Marijke Wijnroks, AIDS Ambassador, Netherlands; Ruben Pecchio, Director REDLA+ (Network of People Living with HIV, Latin America) and UNAIDS Executive Director Michel Sidibé.
We must consider the investments we make now as down-payments that will reduce costs later
UNAIDS Executive Director Michel Sidibé
Treatment for prevention
The panel drew attention to the recent results of the HPTN 052 study announced by the United States National Institutes of Health which demonstrated that if an HIV-positive person adheres to an effective antiretroviral therapy regimen, the risk of transmitting the virus to their uninfected sexual partner can be reduced by 96%.
Involvement of people living with HIV essential
In the discussion, moderated by Al Jazeera television host Riz Khan, the participants highlighted the need to involve people living with HIV in treatment and prevention programmes. “Testing needs to be available to everyone—people living with HIV need to know their status as early as possible to enable them to effectively engage in prevention. ‘Positive prevention’ must be at the centre of prevention efforts and treatment for prevention plays a critical role,” said Mr Pecchio.
Addressing stigma in the context of treatment
According to Secretary of Health of Mexico, José Angel Cordova Villalobos, Mexicohas created a financial vehicle to guarantee sustainable access to treatment over long term. “But we must also work to strengthen education to fight stigma and discrimination and homophobia and to increase people’s willingness to get tested,” said Mr Cordova Villalobos.
With the largest number of people living with HIV in the world, at 5.6 million, South Africa also has the largest antiretroviral treatment programme in the world. The country has also recently launched a national HIV testing campaign in which 12 million South Africans have been tested for HIV between April 2010 and June 2011.
We must also work to strengthen education to fight stigma and discrimination and homophobia and to increase people’s willingness to get tested
José Angel Cordova Villalobos, Secretary of Health of Mexico
“South Africa has no option but to scale up treatment. As testing is scaled up, more people learn their status, and given the evidence of its impact on prevention, this is an important approach,” said Aaron Motsoaledi, Minister of Health of South Africa.
Recent developments in scientific understanding and approaches were highlighted and shown how they can be seen as “game changers.” Country representatives discussed how they can apply this information to further scale up HIV treatment programmes. New information about the prevention benefits of HIV treatment provides an opportunity for increased collaboration within the HIV response.
Investment needs
According to the new UNAIDS investment framework published in the Lancet ahead of the High Level Meeting on AIDS, a relatively small amount of additional money would be required to reach the US$ 22 billion needed for universal access to HIV treatment by 2015. However new data indicate that international investments in AIDS appear to be falling for the first time in 10 years.
“We must consider the investments we make now as down-payments that will reduce costs later,” stressed Mr Sidibé. “It is unacceptable that we have the evidence of the incredible effectiveness of treatment for prevention, yet nine million people living with HIV still don’t have access to it.“
External Links
External Links
Multimedia
Multimedia
Related



Feature Story
Market approaches for innovation and access to medicines: Challenges and opportunities
10 June 2011
10 June 2011 10 June 2011
Credit: UNAIDS
What lessons can be learned from market-based approaches to providing medicines and healthcare in low- and middle-income settings? What are the challenges and future opportunities? These were the key questions raised at an event organised by UNITAID, UNAIDS and the Medicines Patent Pool at the High Level Meeting on AIDS in New York on 9 June.
The event, which took the form of a lively debate, was chaired by Philippe Douste-Blazy, Chair of UNITAID’s Executive Board. Andrew Jack of the Financial Times served as moderator. Speakers included UNAIDS Deputy Executive Director, Programme, Dr Paul De Lay, Dr Precious Matsosa, South Africa’s Director General for Health, Brenda Waning, Coordinator of Market Dynamics at UNITAID, Ellen t’Hoen, Executive Director of the Medicines Patent Pool, and Clifford Samuel of Gilead Sciences.
A changing landscape
The participants discussed how globalization and economic development are changing the international health landscape and examined current challenges to innovation and access. They also looked at interventions needed to ensure that emerging new medicines and technologies can be absorbed by health systems in developing countries.
It was noted that the recent adoption of market-based approaches to public health provision by several donors and international organisations, such as UNITAID—which has committed over US$1.5 billion since 2006—has led to sustainable markets for manufacturers, encouraging price reductions and the development of new medicines, such as AIDS drugs.
We need a research and development agenda that meets the specific needs of low- and middle-income countries. This includes ARV that can be used safely with TB treatment, for children, and during pregnancy
Dr Paul De Lay, UNAIDS Deputy Executive Director, Programme
Paradigm shift
However, this paradigm is beginning to shift. For example, by 2008 India had provided 87% of AIDS medicines used in developing countries. Today, Indian manufacturers are turning their attention towards research and development and service in middle-and high-income markets. This leaves potential space for local producers in low-income countries to establish medicine production for their own markets if such access can be promoted.
In his introductory remarks on future challenges and gaps in innovation and access, Dr De Lay stressed that one key innovation challenge was to provide simplified drug regimens and diagnostics to ensure easier supply and greater adherence to treatment in developing countries.
“We need a research and development agenda that meets the specific needs of low- and middle-income countries. This includes ARV that can be used safely with TB treatment, for children, and during pregnancy,” said Dr De Lay.
“We expect that drug optimization will proceed in several phases which will include optimizing existing treatment including dose reductions and frequency, where possible and implementing emerging new technologies including point of care viral load and CD4 testing; next-generation of low cost, highly effective first and second line treatments; and first generation of long-lasting injectable ART.”
Commenting on exactly why new market approaches were needed to meet today’s challenges, Mr Douste-Blazy explained, “UNITAID works to impact on markets and increase access to innovative products at affordable prices. This is the beginning of an era that sees the poorest people start to gain access to the newest, most expensive products at a price their governments can afford.”
Talking specifically about how to promote innovation in the field of HIV that seeks to address developing country needs, Ms t’Hoen contended that the recently created Medicines Patent Pool “could spur innovation in needed formulations for children and combination medicines as well as bring down prices by promoting generic production of newer medicines.”
Dominant national purchasers emerging
The participants also discussed how industrial and economic developments are helping to change the power-base within the global health landscape from large donors to a few dominant national purchasers. For example, the recent tender by the South African government represents approximately 25% of the developing country market for AIDS medicines and the government also self-funds 75% of the country’s ARV purchases in 2010-2011.
Dr Matsoso expanded on the role national governments play in shaping regional and global markets and underlined the importance of fast tracking the registration of new medicines in developing countries. “We need to harmonise medicines regulation at the regional level to ensure faster uptake of new and innovative products in our countries,” she said.
All those taking part in the event committed to redoubling efforts to protect lives by helping to ensure that attractive markets are created for producers while promoting public health goals of continued innovation and universal access to HIV treatment.
As Dr De Lay summed up: “We have all contributed to the accomplishment of vastly increasing the numbers of people living with HIV who are on ART. For the foreseeable future ART demand will be increasing and we expect to see pressures on ART supply, and continuing innovation in research and development of new ART formulations, as well as for laboratory diagnostic and monitoring tests, is required, and this may require new incentive mechanisms.”
External Links


Feature Story
AIDS and Disability Partners Forum: Enhancing inclusive and accessible HIV programming which fits all the population
09 June 2011
09 June 2011 09 June 2011
Jan Beagle, UNAIDS Deputy Executive Director, Management and External Relations
Credit: UNAIDS
Although there is growing international attention for the rights of people with disabilities, governments and policymakers rarely consider disability issues when formulating their HIV strategic plans.
To highlight the significance of this area of work and advocate for national integration of the needs of persons with disabilities into all aspects of the AIDS response, a partner’s forum on AIDS and Disability was held on 9 June during the High Level Meeting on AIDS.
The event was co-chaired by Jan Beagle, UNAIDS Deputy Executive Director, Management and External Relations and Professor Nora Ellen Groce, Director, Leonard Cheshire Disability & Inclusive Development Centre at University College London.
“Both the AIDS movement and the disability movement have at their core a respect for human rights of the individual. Both are movements which are confronting sigma and discrimination of different kinds. Both HIV and disability affect not only the individual but also the household, in ways that you all know so well. Where you have both HIV and disability, there's a double stigma, and a double burden,” said Jan Beagle, UNAIDS Deputy Executive Director, Management and External Relations, introducing the event.
Mary Muthoni Rop is a mother of three children who lives in rural Kenya. She has multiple disabilities and is living with HIV. She has become an activist with Thika Disabled Fighting HIV and AIDS and spoke at the event of the myriad difficulties and vulnerability the HIV epidemic has brought to people living with a disability which include obstacles to access to HIV services due to distances and infrastructure of health facilities. “We find that most of the health facilities are not accessible to people with disability: for example a hospital having stairs all over,” she said. HIV prevention information is also often inaccessible. “We find that in most of our health facilities, we don't have people who can give proper information to people with disability. We don't have workers trained in sign language interpretation.”
We've all got to work together: governments in North and South, civil society and in particular, people living with disabilities and people living with HIV
Jan Beagle, UNAIDS Deputy Executive Director, Management and External Relations
In 2006 the United Nations Convention on the Rights of Persons with Disabilities was adopted in 2006 and ratified in 2008. This Convention obliges states to provide access to sexual and reproductive health including HIV information and services for all persons with disabilities. The UN Development Group under the leadership of the UNDP Administrator has developed specific guidance for UN country teams on integrating disability into all its work and that of the UN system at global and regional levels.
Stephen Lewis, co-founder and co-director of AIDS-Free World spoke about the need for national government to transform this global instrument into a tool, saying “countries need to understand that they need to take the Convention and turn international law into national law in order for it to be effective and implemented.”
Disabled people’s organizations in different countries in Africa and Asia are becoming more and more involved in the HIV arena to mainstream disability into HIV programmes. Richard Kabeto Matlhare head of Botswana’s National AIDS Coordinating Agency shared insights from his country’s response.
Etienne Krug, Director of Violence and Injury Prevention and Disability gave an overview of the global report which was launched by the World Health Organization earlier in the day “and the big message of the report is that we cannot continue to ignore the needs of 1 billion people in the world.”
“What the report clearly states is that disability results from impairment, but much more from the barriers that society erects. Barriers such as stigma and discrimination, lack of adequate health care and rehabilitation services, inaccessible transport, buildings, information, communication technologies." said Dr Krug
What’s needed is “attacking those barriers, which contribute to a large number of negative outcomes: poorer health status, poorer employment status, less access to education,” he added.
Summing up the discussion as co-chair, Jan Beagle stressed the actions needed to ensure the needs of persons with disabilities are included into all aspects of the AIDS response. “We know that there's very far to go. However, we know how to do it, and the way to do it is by working together. We've all got to work together: governments in North and South, civil society and in particular, people living with disabilities and people living with HIV.”
The AIDS and Disability Partners Forum was organized by UNAIDS in collaboration with Global Partnership for Disability and Development, Health Canada, USAID, US State Department, ILO, UNDESA, UNICEF and WHO.
UN General Assembly High Level Meeting on AIDS
Thirty years into the AIDS epidemic, and 10 years since the landmark UN General Assembly Special Session on HIV/AIDS, the world has come together to review progress and chart the future course of the global AIDS response at the 2011 UN General Assembly High Level Meeting on AIDS from 8–10 June 2011 in New York. Member States are expected to adopt a new Declaration that will reaffirm current commitments and commit to actions to guide and sustain the global AIDS response.
External Links
External Links
Publications
Publications
- HIV/AIDS and Disability: Final Report of the 4th International Policy Dialogue (Health Canada, 2009)
- Global Survey on HIV/AIDS and Disability (World Bank, 2004)


Feature Story
High Level meeting side-event calls for full inclusion and recognition of key populations at risk of HIV in all responses to HIV
10 June 2011
10 June 2011 10 June 2011
Credit: UNIC
Stigma and discrimination and punitive legal environments continue to block people around the world from accessing the HIV services they need. Thirty years into the epidemic they still represent a major barrier to universal access to HIV prevention, treatment, care and support. To find ways to overcome these obstacles, a community dialogue event provided members of key populations at higher risk of HIV a critical and groundbreaking platform at the UN General Assembly High Level Meeting on AIDS to share their expertise and experience. The panellists—who represented leaders among men who have sex with men, people who inject drugs, transgendered people and sex workers—reinforced the call for full recognition and protection of their human rights in all national HIV responses.
Ten years since the 2001 Declaration of Commitment, in which Member States committed to eliminate discrimination against people living with HIV and vulnerable groups, many countries still lack anti-discrimination laws and use punitive approaches to key populations that create barriers between them and HIV services. Countries cite stigma as the single greatest impediment to accelerating progress in the HIV response; however, stigma reduction programmes are neither adequately resourced, taken to scale or targeted to benefit key populations.
The event, hosted by the UK and South Africa Governments and partnered by the International HIV/AIDS Alliance (IAA) and International Federation of the Red Cross (IFRC), was an opportunity for leaders from key populations at risk of HIV to describe what is needed and what is working in the criminalized and discriminatory environments in which they live their everyday lives. Many communities have taken bold steps to overcome human rights abuses and lack of access to HIV services—organizing to demand their rights, providing services through their peers, working with local police and government leaders for recognition and protection. What is needed now is greater support and political, legal and social space for these groups to continue to find and implement such solutions that work for them.
Rather than simply describing the barriers they face in accessing services, they highlighted examples where their key affected population has achieved greater access and offered concrete solutions on how we can address these obstacles in a practical way.
Full respect for the human rights of key populations and evidence-based interventions targeted to the realities they face, as well as support for their leadership and capacity to find solutions for their communities, are all critical to advance the AIDS response
Jan Beagle, UNAIDS Deputy Executive Director, Management and External Relations
United Kingdom Minister for International Development, Stephen O’Brien, in his introductory remarks stressed that for effective AIDS responses, it is essential to work with key populations without prejudice and address restrictive laws that are hampering access to services for key populations.
Alexei Kurmanayevsky from Russia shared his experience as a person who injects drugs and is living with HIV. The panel also included Penninah Mwangi who is the Director of Bar Hostess Association, Nairobi, Kenya—one of the longest standing sex worker-led organizations in Africa. Marcela Romero from Argentina spoke as a transgender person. Othman Mellouk from Morocco spoke about the barriers to delivering effective HIV services to men who have sex with men.
The event was chaired by Michaela Clayton, Executive Director of ARASA and Co-chair of UNAIDS Reference Group on HIV and Human Rights, who also invited interventions from the floor. Jan Beagle, UNAIDS Deputy Executive Director, Management and External Relations, stressed the need for a rights-based approach when addressing HIV. "Full respect for the human rights of key populations and evidence-based interventions targeted to the realities they face, as well as support for their leadership and capacity to find solutions for their communities, are all critical to advance the AIDS response," Ms Beagle said.
The key recommendations from each speaker and the floor discussion were collated into a list of recommended next steps to be presented to the Chairs of the High Level Meeting on AIDS.
UN General Assembly High Level Meeting on AIDS
Thirty years into the AIDS epidemic, and 10 years since the landmark UN General Assembly Special Session on HIV/AIDS, the world has come together to review progress and chart the future course of the global AIDS response at the 2011 UN General Assembly High Level Meeting on AIDS from 8–10 June 2011 in New York. Member States are expected to adopt a new Declaration that will reaffirm current commitments and commit to actions to guide and sustain the global AIDS response.
External Links
External Links



Feature Story
Can MDG 6 be achieved with the Health Workforce we have?
09 June 2011
09 June 2011 09 June 2011
Credit: AMREF
If international aims such as achieving health-related Millennium Development Goals (MDGs) and universal access to HIV services are to be realized, the serious global shortage of health workers must be urgently addressed. This shortage has been severely exacerbated by the AIDS epidemic reducing staff numbers and significantly increasing the workload of those remaining.
At a side event during the High Level Meeting on AIDS in New York this week, the need to recognise human resources as a crucial element in the global AIDS response was explored in depth. Without sufficient human resources, countries' efforts to scale up comprehensive AIDS services will not be sustained, making it impossible to reach the MDGs.
The meeting, Can MDG 6 be achieved with the Health Workforce we have?, was jointly organized by the Global Health Workforce Alliance (GHWA), along with the Government of Brazil, the Commonwealth Secretariat, UNAIDS and the African Medical and Research Foundation (AMREF).
A lively panel discussion, including heads of state, senior representatives from donor and international organisations, civil society and the private sector, examined the interconnectivity of HIV and human resources and also shared best practices.
Joining discussants Mphu Ramatlapeng, both Global Fund Vice-chair and Lesotho’s Health Minister and Secretary Jarbas Barbosa, Brazil’s Secretary of Health Surveillance, were keynote speakers Dileita Mohamed Dileita, Prime Minister of Djibouti and Maxensia Nakibuuka, a Ugandan community health worker living with HIV. The session was moderated by Pulitzer prize-winning journalist Laurie Garrett, who is also Senior Global Health Fellow at the Council on Foreign Relations research centre.
Mr Dileita Mohamed Dileita highlighted the effects of an insufficient number of health workers, their uneven distribution, and limitations in their competencies in his own country, Djibouti. Dr Barbosa agreed that uneven distribution of staff is a major problem in Brazil.
Speaking as a community health worker Maxensia Nakibuuka from Uganda emphasized the difficulties she and her colleagues faced, “We are left to do it alone. Without system strengthening, without budgets; with nothing…We need to be recognized.”
According to Mphu Ramatlapeng, the Global Fund is helping countries meet their needs, with round 11 of Fund proposals including support for health workforce strengthening. She also stressed the crucial need for all stakeholders to work together.
The role of the private sector in offering support was examined. Michael Bzdak, Johnson & Johnson ‘s Director of Contributions and Community relations, spoke of their corporate social responsibility and building health care capacity, primarily in terms of leadership, management techniques and skills training.
Dr Sigrun Mogedal, former-Ambassador, HIV/AIDS and Global Health Initiatives, Norway, and former Chair of the GHWA board, commented on the need to “do things differently.” She referred to the recently released Alliance taskforce report Will we achieve universal access to HIV/AIDS services with the health workforce we have? A snapshot from five countries and stressed actions required by governments and other decision makers. These include: estimating numbers and types of health workers needed to reach international targets; strengthening health workforce management systems; implementing costed plans for increasing and improving the health workforce; and scaling up successful approaches.
Another important aspect raised was the need to focus considerable attention not only on workforce training but on staff retention strategies, looking at motivation and job satisfaction. This point was made by Dr John Palen, Senior HRH advisor of the US President’s Emergency Plan for AIDS Relief (PEPFAR).
The answer to the central question posed was a sobering one: if the impact of AIDS on health workers is not seriously addressed, the human resources crisis will worsen and MDG 6 will become almost impossible to attain. Although progress is being made, there are still many gaps and challenges to overcome.
A report of the meeting will be made available shortly.
Related



Feature Story
New world report on disability: Breaking down barriers
09 June 2011
09 June 2011 09 June 2011
Credit: WHO
The world’s one billion people living with disabilities have poorer health, lower educational achievements and are more prone to social exclusion than those without disabilities. Launched 9 June, the first ever World Report on Disability challenges these disparities and suggests how they can be overcome.
The launch event, which took place during the High Level Meeting on AIDS in New York, was hosted by World Health Organization (WHO) Director-General Dr Margaret Chan and World Bank Vice President Tamar Manuelyan Atinc. The report is produced by both organizations and the two heads were joined by other dignitaries and by representatives of government and civil society.
The publication is a global call to action and assists implementation of the groundbreaking international treaty, the Convention on the Rights of Persons with Disabilities, which was adopted in May 2008. Concerned with national, regional and global policy, it also includes the perspectives of many people who are living with disabilities. In addition, it features the first new disability prevalence estimates for more than three decades: it contends that prevalence is likely to rise in the future due, in part, to the increase in chronic diseases and ageing populations.
We must do more to break the barriers which segregate people with disabilities, in many cases forcing them to the margins of society
Dr Margaret Chan, Director-General, World Health Organization
During the launch event the speakers described the difficulties people with disabilities face, including barriers to accessing health, education, employment and information services.
According to Dr Chan, "Disability is part of the human condition. Almost every one of us will be permanently or temporarily disabled at some point in life. We must do more to break the barriers which segregate people with disabilities, in many cases forcing them to the margins of society."
UNAIDS Executive Director Michel Sidibé called for “an end to all discrimination and inequity faced by people living the disabilities, which not only rob people of their dignity, but block their access to HIV prevention, treatment, care and support.”
HIV and people with disabilities
According to the UNAIDS, WHO and OHCHR policy brief on HIV and disability people with disabilities may be at risk of HIV infection due to a number of reasons, including insufficient access to appropriate HIV prevention and support services, and their higher risk of experiencing sexual assault or abuse during their lifetime. They may also be turned away from HIV education forums or not be invited by outreach workers, because of assumptions that they are not sexually active, or do not engage in other risk behaviours such as injecting drugs.
There must be an end to all discrimination and inequity faced by people living the disabilities, which not only rob people of their dignity, but block their access to HIV prevention, treatment, care and support
Michel Sidibé, UNAIDS Executive Director
The new report gives examples of the issues and situation concerning HIV and people with disabilities. A survey commissioned by the Zimbabwe Parents of Handicapped Children’s Association demonstrated that hearing and visually impaired people were excluded from HIV services because they were not offered in sign language or Braille. On the other hand, there are many examples throughout the report of how individuals, organizations, countries and regions are promoting good practice.
The goal of the World Report on Disability is to provide information and strategic guidance to key actors, such as policy makers, donors and practitioners. A series of recommendations include: investing in specific programmes and services for people with disabilities; adopting a national strategy and action plan; involving people with disabilities in policy and planning decisions and raising public awareness and understanding.
External Links
External links
Publications
Publications
- World report on disability (WHO/World Bank, 2011)
- Disability and HIV policy brief
Multimedia
Multimedia
Related
 Building country-led sustainable HIV responses
Building country-led sustainable HIV responses
20 December 2024

 Towards a life of dignity for people living with disabilities
Towards a life of dignity for people living with disabilities
15 February 2022
Feature Story
It’s possible: Making the most of linking sexual and reproductive health and HIV responses
09 June 2011
09 June 2011 09 June 2011
Dr Babatunde Osotimehin.
Credit: UNFPA
Linking sexual and reproductive health and HIV is of critical importance. Worldwide more than 80% of HIV infections are sexually transmitted. In addition, sexual and reproductive ill health and HIV are fueled by similar causes such as poverty, limited access to services, lack of correct information, gender inequality and social marginalization.
On 8 June, during a side event at this week’s General Assembly High Level Meeting on AIDS in New York, the question of how exactly such linkages can be strengthened was explored. The event was sponsored by UNAIDS, the UN Educational, Scientific and Cultural Organization (UNESCO), the UN Population Fund (UNFPA), the World Health Organization (WHO), and the International Planned Parenthood Federation (IPPF).
The highly interactive session looked at the issue through the prism of five key thematic areas: cost-effectiveness and cost savings of linkages; prevention of mother to child transmission though a sexual and reproductive health platform; comprehensive sexuality education for young people; ending gender-based violence; and human rights of people living with HIV.
Making ‘people-sense’
In his opening remarks, Dr Babatunde Osotimehin, UNFPA Executive Director, explained how the integration of sexual and reproductive health and HIV services makes ‘people-sense’. These services include testing for HIV and other sexually transmitted infections, prevention of mother-to-child transmission, support for fertility decisions, and access to condoms, contraception and correct information. He went on to emphasize wider policy and human rights implications.
“Linking sexual and reproductive health and HIV goes beyond integrating health services,” he said. “It demands from us that we fortify the human rights platform–ending stigma, violence and discrimination.”
Human rights and the right to health were said to be at the core of greater integration of services. A broader human rights agenda can also be promoted that goes beyond service delivery and tackles legal reforms, such as those relating to the right to information and freedom from violence, abuse and coercion.
Sharing ideas and experience
The participants shared ideas and experiences of how those working in the fields of HIV and sexual and reproductive health have combined their efforts to make interventions more effective in creative and innovative ways, including strategies to strengthen treatment as a prevention option.
It was stressed that mother- and child-centred care can improve both sexual and reproductive health and HIV outcomes. For many women, pregnancy is the first point of access in the health system and they can benefit from a range of interventions, including HIV prevention and treatment integrated into routine maternal health care; family planning; and preventing and managing sexually transmitted infections and gender-based violence.
The discussion also showed that when comprehensive sexuality education is effectively implemented on a national scale, there is potential for cost saving from averting HIV infections, other STIs and unintended pregnancies.
Participants examined how men can benefit from greater integration. For instance, in countries where voluntary male circumcision is being implemented for HIV prevention, the number of men accessing other sexual and reproductive services, such as prevention of mother-to-child transmission and treatment of STIs, has increased.
The meeting closed with agreement that linking sexual and reproductive health and the HIV response, especially in a climate of austerity, is a gateway to strengthening both the human rights agenda and health systems.