
Feature Story
“Art for AIDS” receives Keith Haring sculptures
27 November 2008
27 November 2008 27 November 2008
Ahead of World AIDS Day 2008, two sculptures by Keith Haring have come to UNAIDS to join the “Art for AIDS” collection. Credit: UNAIDS
Ahead of World AIDS Day 2008, two sculptures by Keith Haring have come to UNAIDS to join the “Art for AIDS” collection. His iconic and poignant work has been instrumental in raising awareness around AIDS issues worldwide.
The UNAIDS headquarters building in Geneva received on Wednesday two new additions to its “ART for AIDS” collection. The artworks are two sculptures by the celebrated artist and AIDS activist Keith Haring which have been loaned to UNAIDS by the Keith Haring Foundation.
In his all-too-brief lifetime, Keith Haring (1958-1990) produced artwork at a prodigious rate and reached a worldwide audience that transcended differences of race, nationality, gender, age, and sexual orientation. He used his now iconic symbols— the barking dog, radiant baby, dancing person and the heart—to encourage reflection on and dialogue about social and political issues.
The humanist elements of his work allowed him to communicate on virtually universal terms. As a result, Haring used his designs for many public and social awareness campaigns, including AIDS prevention, literacy, UNICEF children's causes, and the fight against South African apartheid.

Haring enlisted his imagery during the last years of his life to generate activism and awareness about AIDS. Credit: UNAIDS
Haring was diagnosed with HIV in 1988. In 1989, he established the Keith Haring Foundation, whose mandate is to provide funding and imagery to AIDS organizations and children’s programmes, and to expand the audience for Haring’s work through exhibitions, publications and the licensing of his images. Haring enlisted his imagery during the last years of his life to speak about his own illness and generate activism and awareness about AIDS.
Although his art had always reflected his social consciousness, in Haring's last years many of his works were devoted to creating cultural awareness about HIV and gay rights issues.
The UNAIDS’ Art for AIDS is an art collection created to recognize the role art has played in the response to AIDS. The pieces in the collection have been chosen to provoke thought and dialogue around some of the most difficult issues around AIDS. With an initial emphasis on contemporary African art, the collection has grown to more than 60 museum quality pieces thanks to the involvement of artists, collectors and donors around the world.
“Art for AIDS” receives Keith Haring sculptures
External links:



Feature Story
The impact of nutrition and HIV: World Food Programme
26 November 2008
26 November 2008 26 November 2008
Credit: UNAIDS/ L. Alyanak
The World Food Programme (WFP) is the lead UN agency providing emergency food assistance and the world's largest humanitarian agency. As a cosponsor of UNAIDS it also plays a unique and significant role in the global AIDS response. In 2007, WFP reached 1.3 million people affected by HIV in 20 of the 25 highest HIV prevalence countries.
For a person living with HIV to respond well to antiretroviral treatment, access to adequate food is essential. WFP was one of the first agencies to provide food to complement the expansion of people’s access to HIV treatment. Last year, WFP supported treatment programmes in 16 African countries, providing food support to over 332,000 beneficiaries during the critical early stages of treatment.
High Food Prices
With high food prices jeopardizing household food security of some of the most vulnerable people in the world, the importance of WFP’s nutritional response for people living with HIV and their families has never been more urgent. A recent pilot study from Zambia showed that food supplementation improved treatment adherence and there is growing evidence from various countries that health clinic attendance has decreased as food prices increase.
UNAIDS and WFP
WFP’s lead role in dietary and nutritional support in the UNAIDS Division of Labour (DoL) involve leadership in the delivery of food assistance and nutritional support and in enhancing national actions through advocacy, guidance and technical support.
WFP is central to efforts to scale up HIV services for populations of humanitarian concern, and it has been integrating HIV treatment and support with inter-agency emergency preparedness, response and recovery activities in Latin America, the Caribbean and Africa. Many different food products are being developed and tested to improve the health and well-being of people on HIV treatment. WFP’s is involved in providing support to scientific studies on the efficacy of specially formulated food products for the nutritional needs of people living with HIV.
Unique contribution at national level
WFP works through national governments and local partners to provide food and nutritional assistance to food insecure people living with HIV and their families. This can make a big difference to a household when the main breadwinner is too ill to work. It also provides in-school meals for orphans and other children affected by HIV. It also provides technical assistance to national governments to ensure that people living with HIV have access to appropriate nutritional food to accompany their treatment and the Programme ensures that people living with HIV link to community support mechanisms to help ensure longer-term livelihood survival.
WFP and “responsible transport”
WFP works with private sector companies that employ thousands of truck drivers to transport food and goods to people in need. However throughout Southern Africa, high prevalence rates of HIV are found along the commercial transport corridors and the World Food Programme, taking its corporate responsibility seriously, wishes to minimize the risks of HIV infection.
In the past year, WFP has improved its HIV prevention and health services for transport workers under its commitment to support “responsible transport”. The project helps to protect the health and well-being of transporters and the local communities they come in contact with along the way. The wellness centre pilot project in Malawi, supported by WFP and TNT, has grown into an independent non-profit alliance called North Star Foundation (NSF) that includes UNAIDS and the International Transport Workers Federation as partners. Five NSF wellness centres are now operating – two in Malawi, one in Namibia, one in Swaziland and one in Zambia; two more in Zimbabwe will open in 2008. NSF will work with Family Health International to set up 23 wellness centres in eight east African countries over the next three years.
Country offices in Benin, Chad, the Democratic Republic of Congo, Ethiopia, The Gambia, Kenya and Niger have worked with United Nations and NGO partners to provide HIV training, improved access to health services and enhanced workplace HIV policies for transport workers.
New Guidance Materials Produced by WFP
In response to requests from country offices for detailed guidance on HIV programming, several guidance tools have recently produced. These are linked on right of the page under “Tools”.
Future Directions
WFP can help advance the debate on and deepen understanding of the nutritional needs of people living with HIV and their family members, working together with the cosponsors by advocating with major funding mechanisms such as PEPFAR and the Global Fund. WFP can help ensure that national and community-level HIV and AIDS programmes, especially treatment programmes, include gender-responsive nutritional components. WFP can also support and promote scientific studies that look at the efficacy of specially formulated foods for the nutritional needs of PLHIV.
The impact of nutrition and HIV: World Food Progr
Cosponsors:
Press centre:
WFP becomes ninth Cosponsor of UNAIDS (16 October 2003)
Feature stories:
New UNAIDS policy on HIV, food security and nutrition (21 May 2008)
AIDS, nutrition and food security (28 November 2007)
External links:
North Star Foundation
International Transport Workers' Federation
Tools:
Food Assistance Programming in the Context of HIV (WFP, 2007)
Food Assistance in the Context of HIV: Ration Design Guide (WFP, 2008)
Publications:
UNAIDS/WFP/WHO Policy Brief – HIV, food security and nutrition (pdf, 247 Kb)
Hunger, health and HIV/AIDS: a critical connection
Full matrix of the UNAIDS Division of Labour (gif, 141 Kb)
UNAIDS Technical Support Division of Labour: Summary & Rationale (pdf, 403 Kb)
Related


Feature Story
Translating intent into action in Ethiopia
25 November 2008
25 November 2008 25 November 2008
The Ethiopian Business Coalition against HIV/AIDS (EBCA), GTZ Engineering Capacity Building Program, the World Bank Institute and the Rapid Results Institute implemented a pilot programme to achieve rapid HIV results within businesses in Ethiopia in 100 days.
Implementing ambitious long-term HIV programmes in the workplace can be a daunting undertaking for a business. In Ethiopia, partners have piloted a management tool designed to restructure policies into a series of short-term goals and produce concrete results quickly.
The Ethiopian Business Coalition against HIV/AIDS (EBCA), GTZ Engineering Capacity Building Program, the World Bank Institute and the Rapid Results Institute implemented a pilot programme to achieve rapid HIV results within businesses in Ethiopia in 100 days.
In March and April 2008, 180 staff from twelve companies, together with six members of EBCA, attended workshops in “Rapid Results Approach” (RRA) for their business HIV programmes. The trainings gave the company teams—management and employees—an opportunity to identify HIV focus areas, set ambitious targets and develop work plans.
Tadesse Tekallign of Crown Cork and Can Share Company is in no doubt about the value of the initiative. “The pilot project is creating new best practices on HIV in Ethiopia’s private sector.” “The companies are finding their own solutions and tackling challenges quickly to produce very effective results,” Tekallign continued.
Achieving their goals

In March and April 2008, 180 staff from twelve companies, together with six members of EBCA, attended workshops in “Rapid Results Approach” (RRA) for their business HIV programmes.
In the three months following the training EBCA gave outreach support to the companies by regular telephone calls, weekly meetings and assistance with setting up partnerships with non governmental organizations and associations who could provide services to the companies.
The companies’ team commitment was impressive and progress substantial. All companies reached, and exceeded, their goals within the time period.
|
Ten companies in Ethiopia took part in the 2008 pilot programme and their goals for the following 100 days were: Alkyd Resin Share Company Crown Cork and Can Share Company East Africa Holding Company Emergency Relief Transport Kaliti Construction Kaliti Metal Mugher Cement Prefabricated Building Parts Production Enterprise Total Ethiopia |
Sustainability
Following the completion of the pilot, a workshop on experience-sharing and sustainability was held for all companies who had participated. EBCA is continuing its follow up and technical support to ensure companies continue their HIV programme implementation.
Next round
EBCA, together with the African Capacity Building Foundation, the World Bank Institute and the Rapid Results Institute have recently launched the second round of Rapid Results in 10 additional Ethiopian companies:
- Coffee Processing
- Comet Transport
- Ethiopian Electric Power Corporation
- Faffa Food Share Company
- Kokeb Flour and Pastas
- National Alcohol and Liquor
- National Mining
- National Motor Corporation
- Nyala Insurance
Rapid Results Approach (RRA)
The Rapid Results Approach (RRA) is a management tool designed to give quick and meaningful results within 100 days or less. By focussing on results it aims to jumpstart major change efforts and assist implementation. RRA is based on the belief that the best way to build capacity is to provide people with real-time support while they work to achieve an ambitious short-term goal that is of critical importance to the organization.
In addition to achieving short-term results and teaching people how to work together, the approach aims to create grassroots capacity to carry out large-scale, complicated changes. It can help companies take their most challenging long-term HIV/AIDS projects and restructure them into a series of short-term initiatives that produce real results quickly. The approach also offers business leaders a new set of skills and expertise in coaching, team building and achieving measurable results quickly.
“UNAIDS is very happy to support the Rapid Results Initiative in Ethiopia. This approach of formulating an action plan with a sharpened focus on producing early results, can be a great model for the private sector and can help engage them better in the AIDS response," said Regina Castillo, Chief Private Sector Partnerships, UNAIDS.
The approach has also been used successfully in HIV and reproductive health programmes in Kenya, Sierra Leone and Madagascar.
Translating intent into action in Ethiopia
Feature stories:
Business coalitions from Latin America and the Caribbean gather in Brazil (13 October 2008)
UN Secretary-General convenes pharmaceutical companies in New York (09 October 2008)
The Life Initiative – Hotels addressing AIDS (23 July 2008)



Feature Story
HIV, Health and Human Rights: The Legacy of Jonathan Mann Today
24 November 2008
24 November 2008 24 November 2008 Jonathan Mann was a visionary physician, advocate and scientist who highlighted the critical links between human rights and public health.
Jonathan Mann was a visionary physician, advocate and scientist who highlighted the critical links between human rights and public health.Today a public event in celebration of Jonathan Mann and his legacy on HIV, health, and human rights is being held at UNAIDS Secretariat, Geneva. The event, co-hosted by UNAIDS, the World Health Organization and the Office of the UN High Commissioner for Human Rights, also marks the 60th Anniversary of the Universal Declaration of Human Rights.
Jonathan Mann was a visionary physician, advocate and scientist who highlighted the critical links between human rights and public health. The enduring relevance of Jonathan’s work is clear—the protection and promotion of human rights is needed now more than ever in the response to AIDS. Stigma and discrimination remain major barriers to achieving universal access to HIV prevention, treatment, care and support. Gender-based violence puts women and girls at risk of HIV infection. Punitive laws keep sex workers, men who have sex with men, people who use drugs and other key populations from accessing the HIV-related programmes and services they need. Panellists will address Jonathan’s legacy, as well as the challenges today and in the years to come in HIV, health and human rights.
HIV, Health and Human Rights: The Legacy of Jonat
Press centre:
UNAIDS acknowledges the health and human rights legacy of Jonathan Mann on the tenth anniversary of his death (2 September 2008)
Multimedia:
Watch the event live online from 17:00 to 20:00 (CET)
Publications:
Invitation to A celebration in honour of Jonathan Mann and the 60th Anniversary of the Universal Declaration of Human Right (pdf, 299 Kb)
Related



Feature Story
Philanthropies major contributors to AIDS
21 November 2008
21 November 2008 21 November 2008
U.S. Philanthropic Support to Address HIV/AIDS in 2007
Total AIDS-related philanthropy in 2007 has risen to US $555 million among U.S.-based philanthropies and to EUR114 million (US $168 million) among Europe-based philanthropies, according to new reports from Funders Concerned About AIDS (FCAA) and the European HIV/AIDS Funders Group (EFG), released in New York yesterday.
The set of reports - the first of its kind - comes at a time when the global financial crisis could potentially impact the global AIDS response.
“There has been a good return on investments made on AIDS” said Dr Paul de Lay, UNAIDS Director for Evidence, Monitoring and Policy. “In the past three years, not only have we seen the number of people on treatment doubling, but also tangible results in HIV prevention efforts, with the number of new HIV infections falling in several countries”.
Sunita Viswanath, FCAA’s Executive Director, emphasized the essential role of the philanthropic sector as governments and global institutions face increasing financial pressures while numbers of people living with HIV - and the risk of infection - continue to rise.
Dr de Lay added, “Philanthropies can play an important role, in supporting a long term and sustainable response to AIDS and help donors and others not lose sight of their goals amidst short term crises – any cutback in investments in the AIDS response today will undoubtedly affect millions of lives”.
The findings from a study in which organizations identified the top population groups that receive the greatest benefit from their domestic and international funding for 2007, identified people living with HIV most frequently as chief beneficiaries of both domestic and international philanthropy by both U.S.-and Europe-based funders.
EFG Chair, Astrid Bonfield, commented on the magnitude of the AIDS epidemic and the challenges and opportunities of funding, remarking that U.S. and European philanthropy could recognize and exercise its ability to be flexible, collaborate, and grow towards the most effective response to HIV.
Over the past three years FCAA worked with EFG and UNAIDS to harmonize their data collection in order to present the most accurate picture of global AIDS-related philanthropy. FCAA, EFG, and UNAIDS are now embarking on an effort to provide information and support to funders internationally through the creation of the Working Group on Global Philanthropic Resource Tracking.
Philanthropies major contributors to AIDS
Press centre:
Press release from FCAA and EFG: New Report Documents Increased Philanthropic Efforts in the U.S. and Europe to Address the Global AIDS Epidemic (21 November 2008)
Feature stories:
UNAIDS and Kaiser Family Foundation release new report assessing funding for AIDS by G8 countries and other major donors (06 July 2008)
External links:
Funders Concerned About AIDS
European HIV/AIDS Funders Group
Publications:
U.S. Philanthropic Support to Address HIV/AIDS in 2007 (pdf, 1.41 Mb)
European Philanthropic Support to Address HIV/AIDS in 2007 (pdf, 1 Mb)



Feature Story
Kenya’s experience informs new resource for increasing coordination on AIDS
21 November 2008
21 November 2008 21 November 2008
The Joint Annual Programme Review process is a vital tool in the global effort by governments and development organizations to ‘make the money work’ Credit: UNAIDS/P.Virot
HIV prevalence in Kenya has halved in a decade – a dramatic and sustained decline rarely seen elsewhere in Africa. The Government aims to continue this level of progress by ensuring that the national response to the epidemic is as coordinated and collaborative as possible, and that funding is spent effectively.
In recent years, as national responses to and funding for AIDS in many countries have become more complex – with more activities, stakeholders and donors than a few years ago – coordination has become an even bigger challenge.
Kenya decided to support coordination by conducting Joint Annual Programme Reviews, which bring together a wide range of people working on AIDS to take a comprehensive look at the overall national response. The Joint Review process is led by the national Government and involves participation at all government levels, as well as by civil society organizations, networks of people living with HIV, local and district authorities, and international donors and organizations.
“Joint Reviews of National AIDS Responses: A Guidance Paper”.
With the lessons learned from the Joint Review processes in Kenya and other countries, UNAIDS has developed a new publication entitled “Joint Reviews of National AIDS Responses: A Guidance Paper”. It aims to help countries conduct Joint Reviews and improve coordination, implementation and funding effectiveness among the many stakeholders involved in national responses.
Well carried out Joint Reviews provide a truly nationally-led forum for sharing information, achievements, shortfalls, challenges and emerging issues, and assessing how well efforts and spending are aligned in meeting the goals of the national AIDS strategy.
Kenya has undertaken in 2007 the 6th consecutive Joint Review of its national response and the process has become a valued method for building bridges and coalitions among the many groups involved in the AIDS response.
 With the lessons learned from the Joint Review processes in Kenya and other countries, UNAIDS has developed a new publication entitled “Joint Reviews of National AIDS Responses: A Guidance Paper”.
With the lessons learned from the Joint Review processes in Kenya and other countries, UNAIDS has developed a new publication entitled “Joint Reviews of National AIDS Responses: A Guidance Paper”.Kenya’s 2007 Joint Review lasted two and a half months and involved hundreds of participants – not a quick or easy process, but well worth the effort. The Review is widely recognized by those working on AIDS as a platform for bringing together data from a range of sectors and levels, including surveillance and service delivery data, as well as qualitative data collected at the community level. The 2007 Review was more inclusive than ever, with participants from all 71 districts and nine regions of the country. The findings and recommendations were used to revise the way the country measures the results of AIDS programmes, and also to inform planning at district and regional levels. The effort of doing regular participatory joint reviews has resulted in more alignment, collaboration and commitment among the many organizations involved in the Kenyan AIDS response.
Anatomy of a Joint Review
The new Guidance Paper gives specific advice for conducting a successful Joint Review. However, just as every country’s AIDS epidemic and response is different, the Joint Review process in each country will differ according to the national political environment, health and social policies, infrastructure, economic development and other factors. Nonetheless, the Guidance Paper lays out several principles which should help build a strong Joint Review process in any country, including:
- national ownership
- inclusion and participation
- commitment to results – participants must agree from the outset to subscribe to the recommendations of the Review
- impartiality
- evidence informed
- enhancing national planning
- sensitivity to gender and human rights.
The Joint Annual Programme Review process is a vital tool in the global effort by governments and development organizations to ‘make the money work’ – ensuring that all AIDS funds are linked to national objectives and simplifying aid structures. In Kenya, for example, the Joint Review process has helped to strengthen donors’ confidence in the quality and effectiveness of national programmes.
The new Guidance Paper on Joint Reviews, along with other related tools, is designed to help countries unite the many stakeholders involved in the AIDS response, in order to increase understanding of the epidemic and work collectively to achieve results.
Kenya’s experience informs new resource for incre
Feature story:
Assessing aid effectiveness at Accra forum (01 September 2008)
Publications:
Joint Reviews of National AIDS Responses: A Guidance Paper (pdf, 316 Kb)
Related


Feature Story
New guidelines for media reporting on HIV in India
19 November 2008
19 November 2008 19 November 2008
Women in Mumbai, India. Credit: UNAIDS/S. Montanari
Journalists have a responsibility to report on HIV issues with accuracy and sensitivity to avoid stigmatizing people living with HIV and to clarify common misunderstandings about the disease, its prevention and transmission.
Following a court case in India where unbalanced reporting led to discrimination against an HIV positive child, the Press Council of India updated its media guidelines on the coverage of HIV-related news. Surveys show that media training and sensitization leads to relatively more balanced and accurate media reportage on HIV particularly in high-prevalence states.
The guidelines were published on 16 November, India’s National Press Day, at a function presided over President of India Pratibha Patil.
“The Press Council of India guidelines are a major step forward in the HIV response and they will set a benchmark for media reporting on the issue,” said Mohuya Chowdhary, Senior Editor, NDTV.
“At a time when the Indian media is expanding at a furious pace, these guidelines are very necessary to ensure qualitative and responsible coverage of HIV-related issues,” he continued.
How the media cover HIV issues or stories related to AIDS
Knowledge and understanding about the virus, as well as developments in HIV treatment, have undergone a sea change since 1993 when the Press Council guidelines for journalists which were first drawn up. The nature of media has also changed with the rise of electronic media in addition to print.
To assist in the review and update of guidelines to media the Press Council of India approached UNAIDS and civil society working in HIV. Workshops were held in September and October 2008 where experts discussed, debated and formulated revisions to the guidelines. They also agreed that this resource should be translated into as many languages as possible for the benefit of the journalists across India. Speaking at the launch, Justice GN Ray, Chairman of the Press Council of India, thanked UNAIDS for facilitating the process of formulating the new guidelines.
As HIV impacts across society they recommend that instead of concentrating on health reporters alone, people at all levels of a news organization should be trained and sensitized on HIV, especially on appropriate terminology.
|
Overview of messages covered in “Guidelines on HIV and Media” - The Press Council of India (October 2008)
|
Be objective, factual and sensitive
The guidelines emphasize that journalists must ensure their story is objective, factual and sensitive, even more so when they are reporting on HIV. This includes highlighting positive stories where appropriate, without underplaying the fact that HIV is a serious issue. Telling the whole story means giving it a human face, and allowing the voices of people living with HIV to be heard.
Accuracy of reporting is critical since important personal and policy decisions may be influenced by media reports and so distortion of facts in any manner is unacceptable. In the context of HIV this means that journalists need to be very careful about the scientific and medical details as well as statistics.
Adopt existing terminology
The guidelines also recommend that journalists and news organizations adopt and widely disseminate existing standardized terminology on reporting on HIV, such as UNAIDS Terminology Guidelines to encourage responsible coverage of the issue.
New guidelines for media reporting on HIV in Indi
Feature stories:
Police in India commit to support community AIDS responses (11 November 2008)
Publications:
Press Council of India - Guidelines on HIV and Media
UNAIDS’ Terminology Guidelines (pdf, 326 Kb)



Feature Story
HIV response in Moldova
17 November 2008
17 November 2008 17 November 2008
Professor Lars Kallings, the UN Secretary-General’s Special Envoy for HIV in Eastern Europe, last month visited the Republic of Moldova.
Professor Lars Kallings, the UN Secretary-General’s Special Envoy for HIV in Eastern Europe, last month visited the Republic of Moldova. During his visit, which coincided with United Nations Day, he emphasized the importance of agencies joining their efforts for a more effective HIV response with enhanced visibility and impact. In a series of meetings Professor Kallings met with the Deputy Prime Minister as well as the Minister of Health, Social Protection, Family and Child and Minister of Education and Youth.
Professor Kallings welcomed the Government of Moldova’s commitments and efforts in the AIDS response and reaffirmed the UN commitment to provide technical support to strengthen the capacity of the Government, trade unions, business and civil society organizations in the national response to AIDS.
During his advocacy mission, he took the opportunity to discuss the following priorities with government officials:
1. Review of legislative framework, with a focus on amending the law on HIV prevention and control of HIV which was adopted in 2007. While largely consistent with human rights standards, it contains certain discriminatory provisions which may limit freedom of movement.
2. Greater sustainability of the efforts in the context of the national AIDS response through increasing contributions from the state budget and institutionalizing mechanisms for improved management of financial resources and better resource needs estimations
3. Scaling-up efforts on HIV prevention based on a strategic framework for clearer focus on results, better accountability and enhanced coordination, with a definite focus on youth, targeted through health education institutionalized in the school curricula
4. Improved inter-sectoral coordination in the national response to HIV, and better involvement of key Ministries like the Ministry of Education and Youth and Ministry of Finance He also held discussions with representatives from the private sector, civil society and international organizations
HIV in Moldova

The Republic of Moldova is classified as a low prevalence country with HIV more likely impacting key populations including people who inject drugs
The Republic of Moldova is classified as a low prevalence country with HIV more likely impacting key populations including people who inject drugs. However there are signs of HIV spreading into the general population as unprotected sex is an increasing mode of transmission in Moldova. According to the World Bank, Moldova, as a proportion of the population, is one of the largest emigration countries in the world. Large-scale emigration by people in search of work, particularly to neighbouring countries like Russia and Ukraine mean there are many migrant workers who may be more vulnerable to HIV infection. Analysts think this may become a determinant in the future evolution of HIV in the Republic of Moldova.
The proportion of women among newly reported HIV cases with sexual route of transmission is also growing (62% in 2007, compared to 57% in 2006).
HIV prevention
Given these trends the UN Envoy emphasized the importance of HIV prevention among the general population for a successful response to AIDS.
“Efforts should be strengthened to reach every woman, every man, and every young person with general prevention information and behavior changing techniques, including HIV prevention programmes in schools and other education institutions and in the workplace,” stressed Professor Lars Kallings.
“Moldova is on the right track towards achieving the goals of the 2001 Declaration of Commitment on HIV/AIDS and the 2006 Political Declaration, and is in the fortunate position of still having a unique window of opportunity that if the HIV is recognized as the highest priority the effectiveness of the national response would be to the utmost and Moldova may become one of the countries in the region which would halt and revert the epidemic by 2015,” noted Dr Sergei Furgal, Director, a.i., UNAIDS Regional Support Team for Eastern Europe and Central Asia.
HIV response in Moldova
Feature stories:
Interview with UN Special Envoy Lars Kallings (20 October 2008)
Journal of Internal Medicine: Review article by L. O. Kallings (21 February 2008)
Professor Lars Kallings’ advocacy visit to Belarus (25 October 2006)
UN Special Envoy for AIDS in Africa Elizabeth Mataka (15 September 2008)
Related

Feature Story
ICC and UNAIDS celebrate partnership and look to future
17 November 2008
17 November 2008 17 November 2008
UNAIDS Deputy Executive Director Michel Sidibé (right) welcomed International Cricket Council President David Morgan to UNAIDS to discuss their continued partnership on AIDS. Geneva, 17 November 2008. Credit: UNAIDS/D. Bregnard
The President of the International Cricket Council (ICC), David Morgan, today visited the UNAIDS Secretariat in Geneva where he was welcomed by UNAIDS Deputy Executive Director Michel Sidibé.
In a meeting with UNAIDS and UNICEF staff the ICC President reaffirmed the Cricket Council’s commitment to the partnership which began in September 2003 when UNAIDS and ICC first teamed up to bring messages of HIV prevention to young people across cricket playing nations. In 2006 UNICEF also joined the partnership which now also supports the “Unite for Children, Unite against AIDS” campaign.
Michel Sidibé reviewed the global successes in the short history of this partnership where through high-profile international events as well as local initiatives, players as well as coaches have spread messages to dispel stigma and misplaced fear and misunderstanding about HIV. He also spoke about the importance of HIV prevention and support services reaching young people.
“We must focus on supporting and working alongside a new generation of young leaders in the AIDS response, including those living with HIV. The work of this partnership can be instrumental in this,” noted Mr Sidibé.
“I would especially like to congratulate the ICC leadership on its commitment to this work and personally thank you for your visit to UNAIDS today.”

(from left): International Cricket Council President David Morgan, UNAIDS Intern Shashank Mane, UNAIDS Youth Intern Korey Chisholm and UNAIDS Deputy Executive Director Michel Sidibé. Geneva, 17 November 2008. Credit: UNAIDS/D. Bregnard
A series of Public Service Announcements on HIV have been recorded by leading stars such as Graeme Smith, Kumar Sangakkara and Mahendra Singh Dhoni for use in stadia at ICC Events and by broadcasters. Activities have taken place at international events including the ICC Cricket World Cup and the ICC World Twenty20 2007. This has included leading players visiting local community projects and wearing red ribbons to show their support for people living with HIV.
A “Cricket HIV and AIDS curriculum” has been developed by the ICC and UNAIDS for players and coaches to help inform young people about HIV and how they can use their influence to make a positive change in their communities. Under the programme “The Captain’s Pledge,” Captains of all Test Cricket playing nations took part in a series of initiatives to help young people understand how HIV is transmitted.
Spirit of Cricket
An interactive discussion on strategic planning for the coming years was led by UNICEF Partnerships Manager, Andres Guerrero.
At the meeting, UNAIDS Youth Intern Korey Chisholm spoke of how sport can be a force for change through breaking down age barriers and building self-esteem. He thanked the ICC for replacing stigma with support. UNAIDS Intern Shashank Mane, from India, also shared his thoughts on the partnership:
“Looking at the influence of cricket in my life, I feel that UNAIDS and the ICC have a lot to offer each other, as well as the world, when it comes to connecting young people through sports with AIDS awareness.”
“The influence of cricket is growing around the world; unfortunately, AIDS continues to be transmitted as well. I could not think of a better way to spread HIV prevention messages and to eradicate HIV-related stigma and discrimination than through a partnership such as this one.”
ICC and UNAIDS celebrate partnership and look to
Cosponsors:
Press centre:
ICC Cricket World Cup West Indies 2007 to Shine Spotlight on Children and Young People Affected by HIV (06 Mar 2007) (pdf, 113 Kb)
India and Pakistan fight AIDS through cricket (08 Apr 2004) (pdf, 107 Kb)
International cricket teams to support World AIDS Day (28 Nov 2003) (pdf, 119 Kb)
Feature stories:
Aussie stars support Love Life project (12 September 2007)
“Cricket can help combat HIV and AIDS”, says Graeme Smith (12 September 2007)
Pakistan cricket team talks about HIV prevention (12 September 2007)
AIDS focus at ICC South Africa cricket championship (10 September 2007)
AIDS events continue at World Cricket Cup (03 April 2007)
Cricket World Cup raises AIDS awareness (11 March 2007)
Multimedia:
View photo gallery of the visit of ICC President to UNAIDS
View the PSAs: Cricketers and their teams speak about HIV/AIDS
External links:
International Cricket Council
Unite for children. Unite against AIDS
Speeches:
Address by Shashank Mane, UNAIDS Intern, during the visit of ICC president to UNAIDS (17 November 2008) (pdf, 31.5 Kb)
Publications:
The ‘Cricket HIV and AIDS Curriculum’ publication (pdf, 1.16 Mb)
Related

Feature Story
“Artists Against AIDS” help fight stigma and discrimination in Russia
17 November 2008
17 November 2008 17 November 2008
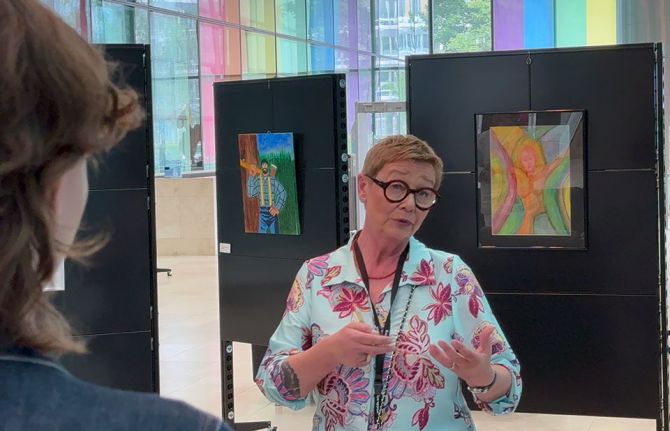
UNAIDS in the Russian Federation launched the initiative “Artists Against AIDS” which aims to decrease stigma and discrimination against people living with HIV.
On 11 November UNAIDS in the Russian Federation launched the initiative “Artists Against AIDS”. The initiative, aims to decrease stigma and discrimination against people living with HIV while raising funds for an orphanage that cares for HIV positive children.
Twenty-three artists, including several well known Russian painters as well as artists from Greece, the Ukraine, the Unites States of America and Spain contributed their works for the exhibition and sale which is being held at the Central House of Artists from 11 – 20 November 2008. More than 200 guests attended the exhibition’s opening ceremony, including representatives from the private sector, the artistic and diplomatic communities, as well as governmental and non-governmental organizations.
Lisa Carty, UNAIDS Country Coordinator opened the exhibition noting that, “In a country like Russia, that has such a deep respect for the arts, it sends a powerful signal when prominent artists speak out against stigma and discrimination. We know that this can make a real difference in mobilizing broader public awareness and support.”
Participating artists welcomed the event as an opportunity to speak about AIDS to help people overcome their prejudices and misconceptions about the disease, as well as to directly help children impacted by HIV.
Sergey Tsigal, one of the twenty three artists who donated their work for the exhibition said, “While I am not a rich man I consider this type of charity project an essential part of my life. Artists can play an important role in the response to AIDS through their art work.”

Artist Sergey Tsigal and Dr. Antonina Petrova, Chief Doctor of the Lomonosov Orphanage at the opening ceremony of the exhibition, 11 November 2008.
The artists have donated 35 paintings and graphic works for the exhibition and sale and all proceeds will be provided to the Lomonosov Children’s Home in Leningrad region.
In Russia about 440,000 cases of HIV infection are officially registered; however, many Russian and international experts believe that the actual number of people living with HIV in the country could be closer to one million. Injecting drug use remains the main mode of transmission, but in recent years the percentage of women living with HIV has grown. In 2007, 44% of all new cases of HIV infection were among women.
The number of children born to women living with HIV has also increased. Even though special preventive therapy makes it possible to reduce a newborn’s risk of infection to a minimum, mother-to-child transmission of HIV continues to occur in children during pregnancy, labour and delivery, or breastfeeding.
Good progress has been made in providing pregnant women with access to preventive treatment to reduce the risk of HIV transmission to their infants. However, in Russia today there are more than three thousand children who were infected at birth.
Among them, a significant number are abandoned children who are cared for in orphanages throughout the country.
Dr. Antonina Petrova, the Chief Doctor of the Lomonosov Orphanage, said that the exhibit and sale gave her an unprecedented opportunity to share with the public the situation of children living with or affected by HIV and for the public to understand that HIV positive children can lead happy, successful lives.
“Artists Against AIDS” help fight stigma and disc
Cosponsors:
External links:
Central House of Artists, Moscow
Publications:
Artists Against AIDS Booklet (pdf, 875 Kb)
Related
 Women, HIV, and war: a triple burden
Women, HIV, and war: a triple burden
12 September 2025
 Displacement and HIV: doubly vulnerable in Ukraine
Displacement and HIV: doubly vulnerable in Ukraine
11 August 2025