
Feature Story
World Refugee Day: ‘What would you do?’
20 June 2012
20 June 2012 20 June 2012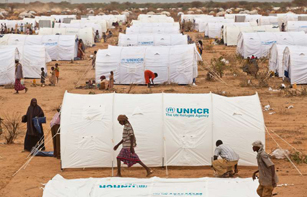
An estimated 4.3 million people were forcibly displaced in 2011, seeking shelter either within their homeland or across a border in another country.
Credit: UNHCR/B.Bannon
How does it feel to become a refugee? How do people fleeing their homes cope with the life and death choices confronting them? To mark World Refugee Day, observed on June 20 every year, stark questions like these are posed by the UN High Commissioner for Refugees (UNHCR) in a new campaign.
The campaign, Dilemmas, seeks to promote understanding of refugees, asylum-seekers, the stateless and internally displaced people by vividly humanizing their experience and reinforcing the fact that they are ordinary individuals faced with extreme and extraordinary situations. A key element of the initiative, along with high profile TV spots by UNHCR Special Envoy Angelina Jolie and other celebrities, is a role playing game called My Life as a Refugee. The game can be played on smartphones and it is being promoted on various digital platforms around the world.
Players choose one of three characters and then have to make a series of difficult decisions to help them reach safety and rebuild their lives. For example, if you opt to be 27 year old Merita, a pregnant mother of two, you will encounter a series of life changing events: ‘Conflict encircles your village, you run for your lives but realize your mother is no longer with you. Do you go back and face death in a war zone or try to escape?’
More people becoming refugees
Such dilemmas are affecting an increasing number of individuals and families. A new publication by the UNHCR, 2011 Global trends: A year of crises, states that 2011 saw more people becoming refugees than at any time this century. 4.3 million people were newly displaced, with around 800,000 of these fleeing their countries and seeking refuge abroad. Cumulatively, by the end of 2011 there were a total of 42.5 million people around the globe forced to move: 15.2 million as refugees, 26.4 million as internally displaced and 895,000 were asylum seekers.
The publication highlights a number of major humanitarian crises in countries such as Cote, d’Ivoire, Libya, Somalia, and Sudan which has led to these mass movements.
According to António Guterres, UN High Commissioner for Refugees, “2011 saw suffering on an epic scale. For so many lives to have been thrown into turmoil over so short a space of time means enormous personal cost for all who were affected….. These are testing times.”
AIDS, Security and Humanitarian Response
Those made to leave their homes and communities in the harshest of circumstances can become more vulnerable to HIV. They often lose their source of income and may have to resort to high-risk behavior to meet their basic needs. Health and education services frequently lapse and information on HIV prevention and treatment provision may be disrupted. Women and girls can be especially vulnerable as rape is often used as a weapon during conflicts. In some cases refugees and internally displaced people also face stigma and discrimination as they are accused of spreading the virus.
“2011 saw suffering on an epic scale. For so many lives to have been thrown into turmoil over so short a space of time means enormous personal cost for all who were affected….. These are testing times.”
António Guterres, UN High Commissioner for Refugees
UNHCR, as one of UNAIDS Cosponsors, promotes and supports the development of comprehensive HIV programmes to make sure refugees have access to HIV prevention, treatment, care and support.
A report on AIDS, Security and Humanitarian Response presented at the 30th UNAIDS Programme Coordinating Board highlights the many and varied ways in which the UNAIDS family and its partners are supporting the HIV response in humanitarian emergencies. A major objective has been mainstreaming AIDS into the overall humanitarian intervention, integrating it as a cross-cutting issue. The report raises a number of concerns that governments and organizations need to take into account, such as providing refugees with continued access to antiretroviral therapy (ART) and HIV prevention services, as well as strategies which deal with broader issues like gender-based violence.
Concrete steps have been taken in a number of areas. For example, several countries have revised their National AIDS Strategic Plans to encompass a range of provisions for the needs of populations of humanitarian concern. In addition, access to ART for refugees has increased markedly. Almost 95% of those in Africa, Latin America and the Middle East and North Africa regions can now get ART at a level similar to the surrounding population. In Africa three quarters of pregnant refugee women have access to programmes to eliminate new HIV infections among children.
A number of other successes are pinpointed. The over half a million Somali refugees in the Dadaab camps in Kenya now benefit from comprehensive reproductive health and HIV services. These include ART, condoms, emergency obstetric interventions and programmes to eliminate new HIV infections among children. This is part of a multi-partner strategy covering refugees and mobile populations across the Horn of Africa. On the Thai-Myanmar border by 2011 tens of thousands of refugees had begun to receive HIV prevention services and post-exposure prophylaxis (PEP) for survivors of sexual violence.
In working with refugees and the displaced to help them get their lives back on track, UNHCR and its partners promote the need for tolerance, empathy and compassion. By presenting real life dilemmas and asking individuals; ‘What would you do?’ the UNHCR’s World Refugee Day campaign provides a powerful spur to understanding the hardships refugees endure and why staying at home may not be an option.
External links
External links
Publications



Feature Story
UNAIDS Board members learn about Kenya’s AIDS response
28 November 2011
28 November 2011 28 November 2011
Credit: UNAIDS
A delegation of the UNAIDS Programme Coordinating Board (PCB) has just concluded a field visit to Kenya. The delegation learned first hand about the government’s strong commitment to a multi-sectoral and integrated AIDS response, including working with civil society organizations in planning and delivering HIV services.
With 1.6 million people currently living with HIV out of a population of 40 million, Kenya has the second largest epidemic in East and Southern Africa and the fourth largest globally.
The PCB delegation included the chair (El Salvador), vice chair (Poland), representatives from Congo, Finland, Mexico, Thailand, PCB NGOs from Africa and Asia Pacific, UNHCR and the UNAIDS Deputy Executive Director, Management and External Relations.
The delegation met with government representatives, including from the Ministry of State for Special Programmes, the National AIDS Control Council (NACC) and the National AIDS and STI Control Program (NASCOP), and civil society organizations.
“We have had the privilege of meeting with a range of institutions and individuals who have been the driving force behind Kenya’s progress in its national AIDS response,” said Jan Beagle, UNAIDS Deputy Executive Director, Management and External Relations. “While challenges remain, we are encouraged by the combination of political will at the highest level, grass-roots activism and support of all partners in advancing the response in Kenya.”
The delegation also met representatives of networks of people living with HIV, children heading households and HIV discordant couples (where only one partner is infected with HIV) during their field visit to Kibera—the largest informal settlement in Eastern Africa. They also visited a Millennium Village Project (MVP) in Nyanza Province, where the delegation witnessed an example of a community and family-centred integrated approach where peer mothers, male champions and community health workers each play a key role in preventing new HIV infections among children.
While challenges remain, we are encouraged by the combination of political will at the highest level, grass-roots activism and support of all partners in advancing the response in Kenya
UNAIDS Deputy Executive Director, Management and External Relations, Jan Beagle
“The Gongo Health Centre in Sauri is a good example of comprehensive and integrated services being made accessible by trained personnel in an efficient manner to those most in need in a rural setting,” said Dr Nieto, Director of the National HIV/STI/AIDS Programme, from the Ministry of Health, El Salvador, current chair of the PCB. “It is a successful model that can and should be replicated in other countries,” she added.
The visit also addressed the crucial role of cultural and traditional leaders, as well as faith-based organizations, in responding to stigma and discrimination against people living with and affected by HIV. The delegation met with the Luo Council of Elders and participated in a meeting of faith-based organizations which focused on the role of these organizations in scaling up HIV prevention and addressing stigma and discrimination.
Kenya’s efforts in promoting a rights-based approach for people living with HIV was evident when the delegation met with the HIV Equity Tribunal that has been established to increase access to justice for people affected by HIV. The Tribunal takes on civil cases of HIV-related stigma and discrimination and is one of the first of its kind in the world.
The delegation also met with representatives of key populations at higher risk, which account for 30% of HIV transmission in the country. “Despite a restrictive legal environment for men who have sex with men, sex workers and people who inject drugs, Kenya has shown that programmes can be extended to key populations at higher risk with the commitment of national AIDS authorities,” said Nadia Rafif, the PCB NGO representative for Africa.
As Kenya’s AIDS response is reliant on external funding–more than 80%—the delegation welcomed the commitment of the Kenyan government to address the issue of sustainable financing and increase domestic resource allocation for HIV.
Resources
Related



Feature Story
Horn of Africa in crisis: famine, displacement and HIV
20 September 2011
20 September 2011 20 September 2011
Credit: UNAIDS/P.Virot
The ongoing drought and famine in the Horn of Africa has put the lives of millions of people in Somalia, Kenya, Djibouti and Ethiopia at serious risk. An estimated 13 million people in the region are in urgent need of humanitarian assistance, including food and medical care.
Central and southern Somalia are the areas hardest-hit in the region, where protracted civil conflicts, weak state structures and limited access to humanitarian assistance pose a complex set of challenges. According to the United Nations High Commissioner for Refugees (UNHCR), there are more than 800 000 Somali refugees in the Horn of Africa, of whom over 250 000 have fled to Kenya, Ethiopia and Djibouti since January 2011.
HIV in emergency settings
While HIV data in central and southern Somalia is scarce, experience and evidence have shown that people in emergency settings tend to have limited access to HIV prevention, treatment, care and support. The health of people living with HIV is put at further risk when their nutritional needs are not met. Displacement, loss of livelihood and increased sexual violence can pose additional risks of HIV infection.
An estimated 3 million Kenyans—among them approximately 90 000 people living with HIV—are affected by drought and food insecurity, especially in the semi-arid regions of northern Kenya. Most HIV services in the country are currently functioning, and treatment interruption is still low. However, the Joint United Nations Programme on HIV/AIDS (UNAIDS) and partners fear this situation may change as community-level interventions and nutritional support for people living with HIV are increasingly interrupted.
In recent weeks, many people in northern Kenya have moved to the slums of Nairobi, seeking a means to survive. City dwellers have faced a doubling of prices for key staple foods. The risk of unprotected transactional sex (or “food for sex”) is rising and could lead to an increase in the number of new HIV infections.
“If HIV-related vulnerabilities are not considered in emergencies, Kenya’s rallying call of an ‘HIV Free Society’ remains a far fetched dream,” said Prof. Alloys S. S. Orago, Director of Kenya’s National AIDS Control Council. “Reducing the vulnerability of people living with HIV in emergency situations requires the effective engagement of all stakeholders,” he added.
Response by UNAIDS and partners
Together with the World Food Programme (WFP) and UNHCR, the UNAIDS Secretariat and other Cosponsors have warned of the urgent need to provide HIV services to emergency-affected populations across the region.
In collaboration with regional partners and national authorities, the UNAIDS family has been working to assess the impact of the current crisis on the HIV epidemic and the related needs of affected populations across the Horn of Africa. This data is being used to effectively integrate HIV in the humanitarian response across the region.
If HIV-related vulnerabilities are not considered in emergencies, Kenya’s rallying call of an ‘HIV Free Society’ remains a far fetched dream
Professor Alloys S. S. Orago, Director of Kenya’s National AIDS Control Council
Many Somalis have fled to a refugee camp in Dadaab, northern Kenya, where comprehensive reproductive health and HIV services are available, including emergency obstetric care, HIV prevention services and the provision of antiretroviral treatment. All camp hospitals provide services for survivors of sexual violence, such as post exposure prophylaxis for HIV prevention, contraception and psychosocial support.
In Kenya, the UN family is collaborating with the national government and non-governmental organizations (NGOs) to ensure that HIV services are available in emergency-affected areas. UNHCR is conducting baseline surveys in the refugee camps and WFP is providing data on nutrition and HIV for the north and north eastern provinces, where drought-affected local populations also require continued HIV prevention, treatment, and care and support services.
In Ethiopia, UNHCR and partners—including more than 10 international NGOs—are working in refugee camps to reduce the transmission of HIV, prevent sexual violence, and provide care for survivors of sexual violence. From the start of the emergency, blood safety measures have been reinforced and male condoms have been made available. For people living with HIV, a national antiretroviral protocol is followed, including CD 4 testing, clinical monitoring and the promotion of treatment adherence.
As part of a wider continental response, the African Union (AU) recently pledged more than US $350 million to the humanitarian crisis in the Horn of Africa. At a meeting of AU Ministers and Heads of State on 25 August, all speakers expressed solidarity with affected populations and emphasized the need to tackle both the current crisis and underlying root causes, including conflict and climate change.
The UNAIDS family and partners will continue to monitor and respond to HIV needs in the Horn of Africa based on the 2010 IASC guidelines for addressing HIV in humanitarian settings. The HIV response in the region is guided by the UNAIDS vision of Zero new HIV infections, Zero discrimination and Zero AIDS-related deaths.
External links
External links
Publications
Publications
Related

Feature Story
Partners come together to lessen HIV-risk for migrants and mobile populations
10 June 2011
10 June 2011 10 June 2011
(Left to Right): Paul De Lay, UNAIDS Deputy Executive Director; Ms. Rosilyne Borland, HIV and Health Promotion Coordinator, IOM; Ambassador William Lacy Swing, Deputy General, IOM; Mr. Udo Janz, Director of UNHCR New York; Dr. Sophia Kisting, Director, ILO/AIDS; at Migration and HIV event, held at UN Headquarters, NYC, on June 10, 2011.
Credit: UNAIDS/B. Hamilton
For the world’s 214 million international migrants and 740 million internal migrants the sometimes challenging conditions of the migration process can leave them vulnerable to HIV infection. Yet, even with the increasing interest in the health and human rights of this key group, the links between migration, population mobility and HIV are still not widely understood.
During the General Assembly High Level Meeting on AIDS in New York governments, civil society partners and intergovernmental agencies came together to explore the relationship between migration and the AIDS epidemic and to examine ways of increasing access to HIV services for people on the move.
The side-event, on 10 June, was sponsored by the International Organization for Migration (IOM), the International Labour Organization (ILO), the UN High Commissioner for Refugees (UNHCR) and UNAIDS.
Ambassador William Lacy Swing, IOM’s Director General and Dr Paul De Lay, UNAIDS Deputy Executive Director, Programme, co-hosted the event. This follows the signing of a revised cooperation of agreement between the two organizations in January this year. The agreement addresses the potential vulnerability of migrants to HIV and strengthens efforts to integrate migrants and mobile populations into AIDS policies and programmes at national, regional and international levels.
“We must harness the benefits of migration for migrants and states, by ensuring migrants can access HIV prevention, care, treatment and support services,” said Ambassador Swing.
We must harness the benefits of migration for migrants and states, by ensuring migrants can access HIV prevention, care, treatment and support services
William Lacy Swing, Director General, IOM
Dr De Lay raised an issue which many ‘people on the move’ face on a daily basis: discrimination. He spoke of the need to vigorously challenge discrimination directed at migrants, and would-be migrants, which prevents freedom of movement. These include the HIV-related entry, stay and residency restrictions in some countries. “Every individual should have equal access to freedom of movement regardless of HIV status. UNAIDS opposes restrictions that single out HIV for special treatment and that restrict movement based on HIV status only. Such restrictions are discriminatory,” he said.
Best practices
The side-event emphasized the importance of sharing best practices and lessons learned by governments and civil society on managing migration and HIV and ensuring the rights of migrants to access health and social services.
It was acknowledged that while mobility in and of itself does not necessarily result in increased health risks, the sometimes challenging conditions of the migration process—before migration, during movement, in destination communities and upon return—may impact the health of migrants and make them more vulnerable to the virus.
International commitments
The meeting explored progress on a number of international commitments and policy frameworks such as sections of the 2001 UNGASS Declaration of Commitment on AIDS which facilitate access to HIV programmes for migrants and mobile workers.
Migration-related aspects of the ILO Recommendation on HIV and AIDS and the World of Work, 2010 (No 200) were also discussed. Dr Sophia Kisting, Director of ILO/AIDS, stressed that stigma and discrimination, difficult working conditions and long separation from their families and cultures increase migrant workers’ vulnerability to HIV. “For these reasons, the Recommendation makes special mention of migrant workers. It calls on countries of origin, transit and destination to take measures to ensure access to HIV prevention, treatment, care and support services for such workers,” she said.
Every individual should have equal access to freedom of movement regardless of HIV status
Dr Paul de Lay, UNAIDS Deputy Executive Director, Programme
In its Technical cooperation projects, the ILO has promoted an integrated approach involving a variety of actors, such as government, recruitment agencies and trades unions. Programmes in Indonesia, Nepal and Sri Lanka have shown the usefulness of this approach and succeeded in including HIV in pre-departure training for labour migrants and initiating policy dialogue between sending and receiving countries.
Addressing such issues is of key importance given that, for example, according to Sri Lanka’s national AIDS committee, some 30-40% of women in Sri Lanka who test positive for HIV have returned home after living in the Middle East.
Udo Janz, Director of UNHCR New York Office, welcomed the chance afforded by the side-meeting to consolidate gains made and chart future action in ensuring migrants and mobile populations, including those forcibly displaced, are provided with HIV services.
UN General Assembly High Level Meeting on AIDS
Thirty years into the AIDS epidemic, and 10 years since the landmark UN General Assembly Special Session on HIV/AIDS, the world has come together to review progress and chart the future course of the global AIDS response at the 2011 UN General Assembly High Level Meeting on AIDS from 8–10 June 2011 in New York. Member States are expected to adopt a new Declaration that will reaffirm current commitments and commit to actions to guide and sustain the global AIDS response.
External Links



Feature Story
UNHCR: Countering stigma and silence about HIV among refugees and host communities in northern Ecuador
04 March 2011
04 March 2011 04 March 2011A version of this story was first published at UNHCR.org

Lucilda, a young mother of two, recently discovered that her husband had infected her with HIV. He recently died and the Colombian refugee finds herself alone in an area where people living with HIV are stigmatized.
Credit: UNAIDS/V. Rodas
Ten years ago, a teenager called Lucilda* ran away from her home in Colombia because she feared her mother's rage after going to a party without permission. At the age of 25 she got married and fled to Ecuador with her husband to escape the conflict in southern Colombia's Putumayo department. Her husband was violent to her and unfaithful. He has since died of an AIDS-related illness and Lucilda is struggling to raise two children alone as a refugee in Ecuador.
"He was very ill, but he didn't want to go to see a doctor. I took him and they told us what was going on. They also said that I was infected," she added. "He knew that he had AIDS, but he never told me."
Lucilda is receiving antiretroviral treatment and both her children are HIV negative. She is one of a small, but growing, number of people living with HIV in northern Ecuador's Sucumbios province and its capital, Lago Agrio, where some 20% of the population of 60,000 are Colombian refugees. At least 30 people here were known to be living with HIV as of the end of last year, double the number for 2009.
"This figure is certainly just the tip of the iceberg with regard to the number of people who are infected with HIV," said Paul Speigel, head of UNHCR's Geneva-based Public Health and HIV Section.
But the lack of openness about HIV is difficult to tackle in a conservative, male-dominated society, where those living with HIV, especially women, face stigmatization. With understanding key to preventing new infections, UNHCR and its partners are trying to counter this mindset and to spread awareness about the virus.
I didn't want him to touch me, but he took a knife and forced me
Lucilda,* a woman living with HIV who is a refugee in Ecuador
A special UNHCR programme to prevent HIV has been implemented by community health workers, and is helping to educate refugees and host communities in isolated areas of the jungle surrounding Lago Agrio. They also give lessons on sexual health, family planning and general health services, explaining the importance of safe sex and ensuring that people have the knowledge and freedom to keep themselves safe from HIV. Tackling gender-based violence is also a major concern in attempts to halt the spread of HIV.
Lucilda has firsthand experience of such violence. When she found out that her husband had been having sex with other women his reaction was harsh.
"I didn't want him to touch me, but he took a knife and forced me," she recalled. "I felt as if I had been raped."
The new UNAIDS strategy 2011-15, promotes zero tolerance of gender-based violence and discrimination. It recognizes that such violence is a human rights violation. It can also hamper people’s ability to adequately protect themselves from HIV infection and make healthy decisions about how, when and with whom they have sex. To successfully challenge the AIDS epidemic it is seen to be of paramount importance that Lucilda and other women live their lives free from the threat of violence.
*Name has been changed to protect her identity


Feature Story
South Sudan addresses concerns of HIV-affected refugees
11 January 2011
11 January 2011 11 January 2011A version of this story first appeared at www.unhcr.org

UNHCR P.Buono
Mary returns to her village during her visit to the Kajo Keji area in southern Sudan
Mary Kiden wants to return to her home in South Sudan more than two decades after fleeing to north-west Uganda, but she has been worried about receiving the health care she needs to stay alive and to support her family.
Forty-one-year-old Mary is living with HIV and takes antiretroviral medicines. At Oliji in the West Nile region of Uganda, she receives the right help, but the infrastructure in South Sudan is in tatters as the region struggles to emerge from years of war between the Khartoum government and the rebel Sudan People's Liberation Army, and five years of fragile peace.
To help her make an informed decision about whether to return to southern Sudan, UNHCR recently invited Mary to join a ‘go-and-see’ visit to Kajo Keji in Central Equatoria state. But on the long drive to her home region, she started finding reasons why she could not return.
She told her fellow refugees that, as the family's only breadwinner, she feared she would not be able to support her mother and children. What worried her most was getting access to antiretrovirals and being stigmatized by people in her village, which did not even have a health clinic when she left all those years ago.
But when Mary finally reached her home region she was pleasantly surprised by what she saw. The town now has a sprawling health centre, complete with new buildings used for HIV testing and counselling, HIV information and drug distribution. The World Health Organization and the Sudanese Ministry of Health have also been supplying antiretroviral drugs for the past year.
Buoyed by her visit to the hospital, Mary next met members of the "Loving Club Association," including a long-lost cousin. This support group, which has received seed funding for livelihood projects from UNHCR, gathers approximately 230 people who are living with HIV. Profits have been used to buy land and provide food for members. According to UNAIDS there were around 260,000 HIV-positive people in Sudan in 2009.
Mary rounded off her visit by spending some time in her village with her cousin, Elia, and his wife, who is also HIV positive. She was delighted when Elia offered her a plot of fertile land if she and her mother returned.
On the drive back to Uganda, Mary said she felt that her concerns about access to drugs, medical care, support and acceptance had been allayed and that she hoped to return to Kajo Keji with her elderly mother and sons in 2012. "I am really very happy," she added.
Related
Feature Story
HIV and conflict: Connections and the need for universal access
27 October 2010
27 October 2010 27 October 2010A Forced Migration Review special supplement

Kibati camp for displaced people, DRC. Credit: Christian Als
The interconnections between conflict and HIV are complex. HIV affects the lives of many people caught up in conflict, including the civilian population but also the protagonists, as well as those whose role it is to provide security during and after conflict.
In conflict, people may be subjected to mass displacement and human rights abuses, including sexual violence, or left in conditions of poverty and powerlessness that might force some individuals to sell sex to survive. In addition, infrastructure may be damaged, and prevention and health services disrupted. Such conditions put populations at increased risk of HIV infection, and women and children are especially vulnerable.
A special supplement on HIV has been published by the journal Forced Migration Review, with support from UNAIDS. This edition is largely based on the work of the AIDS, Security and Conflict Initiative (ASCI), which undertook research over a number of years to gather evidence and advance analysis on the connections between HIV and conflict.
Specially tailored programmes to ensure universal access to vulnerable groups must become an integral part of national HIV policies and strategies, and a key item on the agenda of the international community, according to the article by UNAIDS.
The analysis addresses how to achieve greater and better access to HIV prevention, treatment, care and support for people during and after conflict. It concludes that it is unlikely that Millennium Development Goal 6 will be met without HIV services reaching displaced populations and migrants, regardless of their HIV status, as well as the uniformed services that interact with these populations.
The supplement presents a selection of the ASCI case-studies alongside a number of articles on the subject which were submitted in response to a Forced Migration Review call for articles. UNAIDS and its cosponsors UNFPA and UNHCR as well as various research partners contributed articles. In addition, Dr Nafis Sadik, Special Envoy of the UN Secretary General for HIV/AIDS in Asia and the Pacific authored a piece on the linkages between forced migration and HIV in Asia.
Download the full publication here
Feature Story
16 Days of Activism: The forgotten victims of conflict in the Congo
09 December 2009
09 December 2009 09 December 2009A version of this story was first published at www.unhcr.org

A group of displaced women making handicrafts in eastern Congo.
Credit: UNHCR/D.Nthengwe
Tomorrow, December 10 marks the end of 16 days of activism to end violence against women, an international campaign. UNHCR, the UN refugee agency, is taking the opportunity to draw attention to its work, alongside local partners, in challenging the very high number of rapes occurring in the eastern Democratic Republic of the Congo.
Twenty-eight-year-old widow Kahindo is lucky to be alive after being attacked and abused by armed men while fleeing her village in the Democratic Republic of the Congo (DRC), a country with one of the highest rates of rape in the world.
The young woman and her six children ran into a group of men not far from the village in eastern DRC's volatile North Kivu province. "My reaction was a sigh of relief, thinking we were not going to run anymore," Kahindo recalled. "I was wrong."
She was led away from her children and then "six armed men stripped me naked. They began to rape me one after the other until I went into a coma," an emotional Kahindo told UNHCR near the North Kivu capital, Goma. "They left me for dead."
Today, almost four years later, this forcibly displaced woman sometimes feels that she might as well have died. In between sobs, she told of the terrible price she has paid. "Medical tests showed that I also contracted HIV," she said, adding: "The impact of rape is not just. The stigma that I face is not just, either."
The best strategy to winning this war is to prevent rape from taking place.
Karl Steinacker, coordinator of UNHCR operations in eastern DRC
The widow believes, "I was raped as a punishment for what I am. Those men wanted to degrade me and insult my family, dignity, my culture and everything I stand for."
Her story is appalling, but by no means isolated. According to UN figures, almost 3,500 females were raped by soldiers, militiamen and civilians during the first six months of this year in eastern DRC, compared to some 4,800 for the whole of 2008. The real figures are believed to be higher because many victims do not come forward. During a visit to North Kivu last August, US Secretary of State Hillary Clinton called the widespread sexual violence against women in the conflict-swept region "a crime against humanity."
The forcibly displaced are particularly vulnerable in an area where hundreds of thousands are living with host families or in camps run by UNHCR despite the formal end of war in the DRC in 2003. Civilians live under the constant threat of armed men who pillage, rape, burn houses and confiscate food rations.
These women are very much in the mind of UNHCR and its local implementing partners, such as Women for Women International (WWI) and Search for Common Ground, during the 16 days of activism to end violence against women.
WWI has a project in the DRC to help those who have been raped. "We are making a difference in the lives of rape survivors," said Jose Rugamba, a WWI counsellor based in Goma. "But we cannot say the phenomenon has diminished," she added.
Lena Slachmuijlder, director of Search for Common Ground, said years of war had radicalized attitudes towards women and this was obstructing attempts to combat sexual violence in the DRC. "That is why the scourge of gender-based sexual violence will not reduce, or end, anytime soon."
Most women argue that the failure to jail and punish convicted offenders has led to a culture of impunity and to growing misogyny. "Twenty years is usually the jail term for offenders. But here in Congo, a rapist can be released after paying the equivalent of US$3 to a prison warden," claimed one woman.
Sexual violence can also have a devastating effect on family relationships. Rape survivors are often rejected by family members and their communities, who fail to appreciate the physical and psychological trauma of rape. Changing mindsets will take a long time.
"The best strategy to winning this war is to prevent rape from taking place," said Karl Steinacker, coordinator of UNHCR operations in eastern DRC. That will be a tough task, and one that must tackle immunity and help spread awareness.
Under a UNHCR-sponsored programme, Search for Common Ground is trying to do the latter. The United States-based non-governmental organization has been going through towns and villages in eastern and south-eastern provinces screening films and videos on the issue of sexual and gender-based violence.
Slachmuijlder said the mobile cinema has an impact because the subjects of the films are real people. By allowing the victims of sexual violence to speak out, she said, "We are giving space for interaction and debate on issues people consider taboo, but which should be openly discussed to demystify the issues."
In partnership with other agencies, UNHCR is also assisting rape victims through counselling, medical treatment, micro-finance projects and reintegration activities.
For UNAIDS, this issue is a major concern and its Outcome Framework 2009-11 has stopping violence against women and girls as one of nine priority areas.
16 Days of Activism: The forgotten victims of con
Cosponsors:
Press centre:
Feature stories:
UNHCR chief pledges to keep AIDS response a priority (03 December 2009)
Violence against women and HIV (10 November 2009)
UNAIDS partners in new Clinton Global Initiative to address sexual violence against girls (25 September 2009)
HIV in humanitarian crises: Opportunities and challenges (12 August 2009)
Addressing the HIV-related needs of “people on the move” (19 June 2009)
Challenging violence against women a key task for newly launched Caribbean Coalition on Women, Girls and AIDS (06 March 2009)
Publications:
Partnering with Men to End Gender-based Violence: Practices that work from Eastern Europe and Central Asia (pdf, 1.75 Mb.)
Women and Health: Today’s Evidence, Tomorrow’s Agenda
UNAIDS Outcome framework 2009-11 (pdf, 396 Kb.)


Feature Story
UNHCR chief pledges to keep AIDS response a priority
03 December 2009
03 December 2009 03 December 2009
Rocking in Nepal: A band on stage at the World AIDS Day concert in Damak.
Credit: UNHCR
As the world marked World AIDS Day on Tuesday, UNHCR’s chief, António Guterres, revealed that the UN Refugee Agency had expanded its global HIV interventions.
Guterres, while reiterating his personal commitment to keeping AIDS a priority for UNHCR, also stressed that his agency would continue to advocate for the abolishment of laws discriminating against those with HIV.
In an annual message to staff, the High Commissioner noted: "We now have activities in more than 75 countries, and 75 percent of refugees have access to anti-retroviral therapy when it is available to surrounding host country nationals, whereas 63 percent have access to prevention of mother-to-child transmission programmes (PMTCT)."
We have 100 percent coverage for voluntary counselling and testing, PMTCT and anti-retroviral therapy for refugees.".
UN High Commissioner for Refugees, António Guterres (UNHCR)
He continued that in southern Africa, the epicentre of the AIDS epidemic, "We have 100 percent coverage for voluntary counselling and testing, PMTCT and anti-retroviral therapy for refugees." In 2005, UNHCR only had HIV programmes in Africa and Asia; it has since expanded these to the Americas and Eastern Europe.
Guterres said UNHCR's goal was to ensure that all people of concern to the agency had access to these essential services. "Furthermore, the HIV and AIDS response for internally displaced persons and for high risk groups among UNHCR's persons of concern needs strengthening," he said.
The High Commissioner also pledged to help staff members affected by HIV. "More needs to be done to combat stigma and to support those staff members who live with HIV. We are committed to reaching the 10 UN minimum standards on HIV in the workplace by 2011, so that every staff member has an active knowledge about HIV and AIDS prevention, treatment and related rights within the UN system," he said.

Refugees in Gambia commemorate World AIDS Day.
Credit: UNHCR
"World AIDS Day provides each of us with an opportunity to renew our resolve to fight the epidemic both in our personal and professional lives and I encourage us all to do exactly that," Guterres concluded.
UNHCR held a wide range of activities at Geneva headquarters and in field offices and camps for the forcibly displaced around the world. A banner of a large red ribbon, symbolizing AIDS awareness, was hanging from the façade of the headquarters building, where staff could pick up literature and educational material on HIV as well as purchase silk and cotton clothing items made by people living with HIV in Thailand.
Among overseas events held to mark World AIDS Day, was an awareness-raising concert for refugees and local communities in eastern Nepal. The event, held at a school in Damak with support from FC Barcelona, featured a wide range of music, including Nepali folk, raga, rock, funk, blues and jazz.
UNHCR chief pledges to keep AIDS response a prior
Cosponsors:
Feature stories:
UNHCR reflects on progress and remaining challenges on World AIDS Day (02 December 2009)
Addressing the HIV-related needs of “people on the move” (19 June 2009)
HIV in humanitarian crises: Opportunities and challenges (12 August 2009)
Publications:
Human rights for everyone (pdf, 1.89 Mb.)
Feature Story
HIV in humanitarian crises : Opportunities and challenges
12 August 2009
12 August 2009 12 August 2009
The relationship between humanitarian crises and HIV was the key issue, at a satellite session sponsored by UNHCR and UNAIDS at the 9th International Congress on AIDS in Asia and the Pacific. Credit: UNAIDS/O.O'Hanlon
With millions of people around the world forced to move by conflict and natural disasters, examining the relationship between humanitarian crises and HIV is becoming increasingly critical. This key issue, and its implications for Asia, was highlighted in a satellite session at the 9th International Congress on AIDS in Asia and the Pacific sponsored by the United Nations High Commissioner for Refugees (UNHCR) and the Joint United Nations Programme on HIV/AIDS (UNAIDS).
The connection between humanitarian crises and the HIV epidemic is not straightforward. Emergencies can increase vulnerability to HIV transmission but this does not necessarily result in increased risk behaviors or higher HIV prevalence. People facing conflict or natural disasters often lose their source of income and some may have to resort to high-risk behaviour to meet their basic needs. Social and sexual norms can break down and women can be especially vulnerable as an increase in rape is often associated with conflict and with displacement. However, humanitarian crises can play a protective role, as population mobility is sometimes curtailed and access to quality health and other social services can be improved, especially in long-term displacement.
During the session, Opportunities and challenges in addressing HIV amongst diverse humanitarian populations, panellists working with displaced people or in other humanitarian contexts explored these vexed questions. They also argued that in every instance where a humanitarian crisis occurs, whether in a high or low prevalence setting, minimum interventions to prevent HIV and respond to it are necessary.
The aim of the meeting was to increase awareness of the HIV epidemic among key stakeholders, encouraging them to ensure that humanitarian populations have access to prevention, treatment, care and support services, whatever their situation. The panel and participants were also keen to exchange ideas and expertise, lessons learned, challenges faced and successes achieved in HIV programmes in humanitarian settings in the Asia region, with the aim of developing and strengthening partnerships between relevant actors in the field.
Speakers at the session were set to explore a wide range of ideas and information. Presentations included: an overview of the epidemiology and programmatic principles of HIV in conflict and experience to date in the Asia region; integrating HIV into China’s disaster response scenario; successes and challenges in HIV programmes among Afghan injecting drug users living as refugees in Pakistan; and treatment programmes in stable refugee settings in Thailand.
UNHCR is the lead UN agency for addressing HIV among refugees and people internally displaced as a result of conflict. It aims to ensure access to comprehensive programmes relating to HIV prevention, including prevention of mother-to-child transmission, voluntary counseling and testing, development and dissemination of information-education-communication materials, care, support and treatment and monitoring and evaluation.
HIV in humanitarian crises : Opportunities and ch
Cosponsors:
Feature stories:
Addressing the HIV-related needs of “people on the move” (19 June 2009)
UNHCR reflects on progress and remaining challenges on World AIDS Day (02 December 2008)
Publications:
UNESCO and UNHCR publication “Educational Responses to HIV and AIDS for Refugees and Internally Displaced Persons: Discussion Paper for Decision Makers” (pdf, 820.8 Kb.)
Strategies to support the HIV-related needs of refugees and host populations: A joint publication of the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the United Nations High Commissioner for Refugees (UNHCR) UNAIDS Best Practice Collection
HIV-related needs in Internally Displaced Persons and other conflict-affected populations: A rapid assessment tool. (pdf, 612 Kb.)
Policy Brief: HIV and Refugees (pdf, 267.5 Kb.)
The need for HIV/AIDS interventions in emergency settings (pdf. 335.7 Kb.)
