
Feature Story
Eight-year trend shows new HIV infections down by 17%—most progress seen in sub-Saharan Africa
24 November 2009
24 November 2009 24 November 2009Efforts towards universal access to HIV prevention, treatment, care and support are bringing AIDS out of isolation
UNAIDS Executive Director Michel Sidibé launches double report in Shanghai, 24 November 2009.
Credit: UNAIDS
Geneva / Shanghai, 24 November 2009 – According to new data in the 2009 AIDS epidemic update, new HIV infections have been reduced by 17% over the past eight years. Since 2001, when the United Nations Declaration of Commitment on HIV/AIDS was signed, the number of new infections in sub-Saharan Africa is approximately 15% lower, which is about 400,000 fewer infections in 2008. In East Asia new HIV infections declined by nearly 25% and in South and South East Asia by 10% in the same time period. In Eastern Europe, after a dramatic increase in new infections among injecting drug users, the epidemic has leveled off considerably. However, in some countries there are signs that new HIV infections are rising again.

Credit: UNAIDS
The report, released today by the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the World Health Organization (WHO), highlights that beyond the peak and natural course of the epidemic—HIV prevention programmes are making a difference.
“The good news is that we have evidence that the declines we are seeing are due, at least in part, to HIV prevention,” said Michel Sidibé, Executive Director of UNAIDS. “However, the findings also show that prevention programming is often off the mark and that if we do a better job of getting resources and programmes to where they will make most impact, quicker progress can be made and more lives saved.”
In this first double issue, the UNAIDS Outlook report further explores how “modes of transmission” studies are changing the approach of HIV prevention efforts. The new magazine-style report looks at new ideas and ways to use the data collected in the companion epidemiological report.
An estimated:
- 33.4 million [31.1 million–35.8 million] people are living with HIV worldwide
- 2.7 million [2.4 million–3.0 million] people were newly infected in 2008
- 2 million [1.7– 2.4 million] people died of AIDS related illness in 2008
Universal access to HIV prevention, treatment, care and support

photo caption. Credit:
Data from the AIDS Epidemic Update also show that at 33.4 million, [31.1 million–35.8 million] there are more people living with HIV than ever before as people are living longer due to the beneficial effects of antiretroviral therapy and population growth. However the number of AIDS-related deaths has declined by over 10% over the past five years as more people gained to access to the life saving treatment. UNAIDS and WHO estimate that since the availability of effective treatment in 1996, some 2.9 million lives have been saved.
"International and national investment in HIV treatment scale-up have yielded concrete and measurable results,” said Dr Margaret Chan, Director General of WHO. “We cannot let this momentum wane. Now is the time to redouble our efforts, and save many more lives."
Antiretroviral therapy has also made a significant impact in preventing new infections in children as more HIV- positive mothers gain access to treatment preventing them from transmitting the virus to their children. Around 200 000 new infections among children have been prevented since 2001.
In Botswana, where treatment coverage is 80%, AIDS-related deaths have fallen by over 50% over the past five years and the number of children newly orphaned is also coming down as parents are living longer.
AIDS out of isolation
One of the significant findings of the report is that the impact of the AIDS response is high where HIV prevention and treatment programmes have been integrated with other health and social welfare services. Early evidence shows that HIV may be a significant factor in maternal mortality. Research models using South African data estimate that about 50,000 maternal deaths were associated with HIV in 2008.
“AIDS isolation must end,” said Mr Sidibé. “Already research models are showing that HIV may have a significant impact on maternal mortality. Half of all maternal deaths in Botswana and South Africa are due to HIV. This tells us that we must work for a unified health approach bringing maternal and child health and HIV programmes as well as tuberculosis programmes together to work to achieve their common goal.”
The AIDS epidemic is evolving and HIV prevention programmes are not rapidly adjusting to the changes
The double report also shows that the face of the epidemic is changing and that prevention efforts are not keeping pace with this shift. For example the epidemic in Eastern Europe and Central Asia once characterized by injecting drug use is now spreading to the sexual partners of people who inject drugs. Similarly in parts of Asia an epidemic once characterized by transmission through sex work and injecting drug use is now increasingly affecting heterosexual couples.
Data show that few HIV prevention programmes exist for people over 25, married couples or people in stable relationships, widowers and divorcees. These are the same groups in which HIV prevalence has been found to be high in many sub-Saharan countries. For example in Swaziland people over the age of 25 accounted for more than two thirds of adult infections yet very few HIV prevention programmes are designed for older people.
Funding for HIV prevention has become the smallest percentage of the HIV budgets of many countries. For example in Swaziland, just 17% of the country’s total budget for AIDS was spent on prevention despite a national HIV prevalence rate of 26%. In Ghana, the prevention budget was cut in 2007 by 43% from 2005 levels.
Building capacity: new social networking site for global AIDS community
Building on the need to maximize results and to better connect the 33.4 million people living with HIV and the millions of people who are part of the AIDS response, UNAIDS has launched AIDSspace.org. This social networking site is open to the community and is free.
AIDSspace.org aims to expand informal and established networks to include more people interested in HIV to maximize resources for a stronger AIDS response. The premise behind AIDSspace is simple: if hundreds of millions of people can connect on some of the most popular social networking sites (e.g. Facebook, LinkedIn, MySpace, Twitter, YouTube) to connect, exchange ideas, post and share HIV-related content, they can do the same for HIV related content—including key policies, case studies, multimedia materials, conference posters, reports and other essential resources. Users can also find and post jobs and reviews on service providers on AIDSspace.org
Press conference launch of two publications, Shanghai, 24 November 2009.
Speakers from left) Ms Annemarie Hou, Director Communicaitons UNAIDS; Mr Michel Sidibé, Executive Director, UNAIDS; Dr Chen Zhu, Chinese Minister of Health; Dr Hiroki Nakatani, Assistant Director General, AIDS, TB, Malaria and Neglected Tropical Diseases, WHO; Ms Zhao Chunki, Social worker.
UNAIDS is an innovative joint venture of the United Nations, bringing together the efforts and resources of the UNAIDS Secretariat and ten UN system organizations in the AIDS response. The Secretariat headquarters is in Geneva, Switzerland—with staff on the ground in more than 80 countries. The Cosponsors include UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, ILO, UNESCO, WHO and the World Bank. Contributing to achieving global commitments to universal access to comprehensive interventions for HIV prevention, treatment, care and support is the number one priority for UNAIDS. Visit the UNAIDS website at www.unaids.org
The World Health Organization (WHO) is the directing and coordinating authority for health within the United Nations system. It is responsible for providing leadership on global health matters, shaping the health research agenda, setting norms and standards, articulating evidence-based policy options, providing technical support to countries and monitoring and assessing health trends. For more information, please visit www.who.int
AIDSspace.org is an online community for connecting people, sharing knowledge, and accessing services for the 33.4 million people living with HIV and the millions who are part of the response. Sign up today at www.aidsspace.org
Eight-year trend shows new HIV infections down by
Cosponsors:
Press centre:
Download printable PDF (pdf)
Multimedia from press conference launches in Shanghai and Geneva (24 November 2009)
Feature stories:
UNAIDS Outlook 2010: Fresh perspective on the AIDS epidemic and response (24 November 2009)
Contact:
Sophie Barton-Knott
Tel: +41 22 791 1697
Email: bartonknotts@unaids.org
Publications:
2009 AIDS Epidemic Update (pdf, 3 mb)
Corrigendum to version downloaded before 25 November 14:00
UNAIDS Outlook 2010 (pdf, 4 mb)



Feature Story
UNAIDS Outlook 2010: Fresh perspective on the AIDS epidemic and response
24 November 2009
24 November 2009 24 November 2009
It’s clear that the HIV epidemic the world faces today is not the same as when it peaked in 1996. The number of people living with HIV globally is now at 33.4 million and although 2.7 million people became newly infected with HIV in 2008, good news is that this is a decrease by 17% over the last eight years.
There have been many successes in the AIDS response in recent times including increases in HIV treatment coverage and prevention of mother-to-child transmission services, and an indication of decline in HIV incidence in some regions. However, at the moment globally five people are becoming infected with HIV for every two people accessing treatment.
It is therefore critical that the way we respond keeps pace with and overtakes the epidemic if we are to see a real change in people’s lives, aspirations and futures.
UNAIDS Outlook 2010, a new publication launched today, explores new ideas and ways to use the data collected in the AIDS Epidemic Update companion report.
Outlook gives an overview of the epidemic with global and regional statistics, but also contains analysis offering the UNAIDS interpretation and eyes the data available in the more detailed AIDS Epidemic Update report from different angles.
The cover of Outlook features Prudence Mabele, the first black woman in South Africa to disclose her HIV status publicly in 1992 because she was “tired of the silence and stigma surrounding HIV,” as she puts it. Seventeen years down the road, Prudence is the executive director of the Positive Women’s Network she created in 1996. In Outlook we follow her for day.
The publication also poses a number of bold questions that call for a response: How can we use our knowledge of the HIV epidemic and response for more effective programming at country level? How do we become smarter about HIV prevention to make a real difference? What is the anatomy of a bad law from a human rights perspective?
Features include “Where does the Money for AIDS go?” exploring fund flows in the AIDS response and “Being the Change” digging deeper into issues on young people, sexuality and how behaviors are changing, mixed with captivating images and storytelling narratives to show the plight of individuals.
Tying the Outlook together is an intimate interview with UNAIDS Executive Director, Mr Michel Sidibé who as he approaches the end of his first year in office as UNAIDS head sees real change and is inspired by the perseverance of the human spirit every day. In this one-on-one with the reader, Mr Sidibé renews his commitment to push himself, UNAIDS and the world to deliver in the AIDS response.
UNAIDS Outlook 2010: Fresh perspective on the AID
Multimedia:

UNAIDS OUTLOOK Report 2010 & 2009 AIDS epidemic update full collection of photos
Press centre:
Eight-year trend shows new HIV infections down by 17%—most progress seen in sub-Saharan Africa (24 November 2009)
Publications:
UNAIDS Outlook 2010 (pdf, 4 mb)
2009 AIDS epidemic update (pdf, 3 mb)
Corrigendum to version downloaded before 25 November 14:00
Social media:
Related


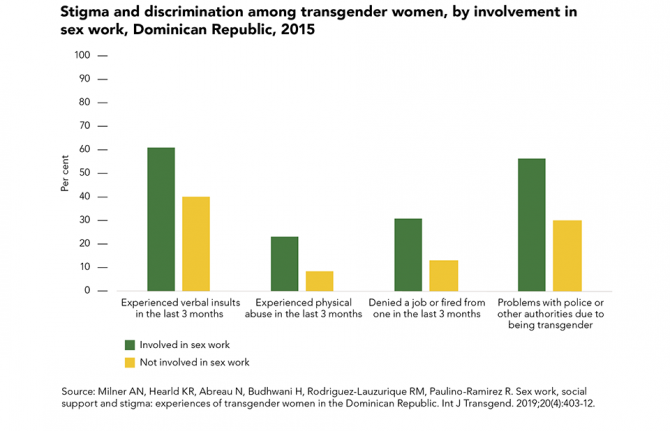 Transgender sex workers face frequent abuse
Transgender sex workers face frequent abuse
29 March 2022
Feature Story
Michel Sidibé commends China’s progress in AIDS response
24 November 2009
24 November 2009 24 November 2009
UNAIDS Executive Director, Michel Sidibé in Shanghai, China on 23 November 2009. Credit: UNAIDS
UNAIDS Executive Director Michel Sidibé, during his visit to China, commended the People’s Republic of China on rises in domestic spending for HIV prevention and care in spite of a global financial crisis where other countries are weighing the risks of making cuts.
Speaking during the opening of the Fifth Conference for the International Cooperation Programme on AIDS in Shanghai, Mr Sidibé congratulated the country, saying, “China’s progress can invigorate an AIDS response that teaches and inspires the world.”
The world eagerly anticipates China’s enhanced role in global governance—and its leadership in the global response to AIDS.
Michel Sidibé, UNAIDS Executive Director
Also on the panel with Mr Sidibé were China’s Health Minister, Dr Chen Zhu; Mayor of Shanghai, Han Zheng; Vice Director of the Department of International Cooperation, Dr Ren Minghui; Dr Wu Zunyou from the National Centre for HIV/AIDS Control and Prevention (China) and UNFPA's Dr Bernard Coquelin.
Earlier during his visit Mr Sidibé held a bilateral meeting with Health Minister Dr Chen Zhu and acknowledged the country’s progress on the AIDS response.
While HIV prevalence in China is estimated to be less than 0.1 per cent of the total population, the epidemic continues to grow – the majority of new infections are related to injecting drug use and sexual transmission.
China’s senior leaders, including President Hu Jintao and Premier Wen Jiabao, have over the years shown commitment towards addressing the AIDS epidemic. The national budget for HIV prevention and care rose from RMB 390 million (US$48.75 million) in 2003 to RMB 983 million (US$144.13 million) in 2008. The Global Fund to Fight AIDS, TB and Malaria has recently approved a disbursement of US$ 500 million to China to scale up its programmes for HIV prevention, treatment and care.
Mr Sidibé added, “The world eagerly anticipates China’s enhanced role in global governance—and its leadership in the global response to AIDS.” It has accomplished some of the lowest child and maternal death rates and lowest prevalence of HIV, TB and malaria.
Its “Four Frees and One Care” policy provides free voluntary counselling and testing, free antiretroviral treatment, free services to prevent mother-to-child transmission, free schooling for children orphaned by AIDS, and care for people with HIV in 127 sites nationwide.
Also, China now has more drug replacement clinics and needle social marketing programmes than any other country in Asia.
Speaking about China’s national AIDS programme, Mr Sidibé noted, “This scale of transformation gives me and many others hope that China can make breathtaking strides in other areas of universal access, if the will is there. And I believe it is.”
Mr Sidibé called for human rights, equity and the involvement of the civil society and affected communities in all aspects of the AIDS response.
Earlier in the day Mr Sidibé launched two publications UNAIDS Outlook 2010 and 2009 AIDS Epidemic Update at a press conference. Dr Chen Zhu, Chinese Minister of Health; Dr Hiroki Nakatani, Assistant Director General, AIDS, TB, Malaria and Neglected Tropical Diseases, WHO; and Ms Zhao Chunki, Social worker also participated in the press conference which was webcast live from Shanghai.
The Executive Director plans to meet with China’s Vice Premier, Mr Li Keqiang, as well as launch the highlights of the China Stigma Index that documents the stigma and discrimination experienced by people living with HIV in China.
Later in the week, Mr Sidibé’s will also participate in the launch of two campaign materials on awareness about AIDS: a poster and a public service announcement featuring Chinese basketball star Yao Ming and a group of people living with HIV.
Michel Sidibé commends China’s progress in AIDS r
Key populations:
People who use injecting drugs
Sex workers and clients
Partners:
The Global Fund to Fight AIDS, TB and Malaria
Press centre:
Eight-year trend shows new HIV infections down by 17%—most progress seen in sub-Saharan Africa
Multimedia:
Feature stories:
UNAIDS Executive Director visit to China opens with focus on civil society
External links:
Global Business Coalition
International Cooperation Programme on AIDS
Publications:
AIDS epidemic update 2009 (pdf, 1.60 Mb)
UNAIDS Outlook Report 2010 (pdf, 4 Mb.)
A joint assessment of HIV/AIDS prevention, treatment and care in China


Feature Story
UNAIDS Executive Director visit to China opens with focus on civil society
23 November 2009
23 November 2009 23 November 2009
UNAIDS Executive Director, Michel Sidibé with Dr. Zhao Hongxin, winner of the Positive Commitment, Treatment and Care Award in Shanghai, China on 23 November 2009. Credit: UNAIDS
UNAIDS Executive Secretary Michel Sidibé arrived in Shanghai this week on the first leg of a two-city visit to China. During the visit, Michel Sidibé will visit Shanghai and Beijing, launch the 2009 AIDS Epidemic Update and meet with many key partners from Chinese government and civil society. Michel Sidibé began his visit by attending a prize giving ceremony organised by the China office of the International Treatment Preparedness Coalition, an organization that works to improve treatment conditions for people living with HIV at the local, regional and international levels.
During the ceremony, prizes were awarded to civil society figures, medical workers, government officials and organizations that have made exceptional contributions to the response to AIDS in China, in the fields of community mobilization, treatment and care, and policy implementation.
Dr Cai Weiping, a doctor renowned for his work with people living with HIV, was awarded a prize for his contributions to treatment and care. Accepting the prize, Dr Cai said “I have received many awards in 26 years of being a practising physician, but this is the first prize I’ve ever received from the community, or from my patients. The best recognition that a doctor can receive is not from the government or from a hospital, but from his patients.”
When I was listening to the people who have been working hard, giving voice to the voiceless, I feel like it is not just about receiving an award, it’s about saving lives, it’s about giving social justice, it’s about redistributing opportunity.
Michel Sidibé, UNAIDS Executive Director
Michel Sidibé highlighted the importance of the dedication shown by prize recipients: “I think what we are talking about today is restoring dignity,” Michel noted, “When I was listening to the people who have been working hard, giving voice to the voiceless, I feel like it is not just about receiving an award, it’s about saving lives, it’s about giving social justice, it’s about redistributing opportunity.”
After presenting awards at the ceremony, Michel Sidibé met for lunch with workers and volunteers from local Shanghai civil society organizations. Joining the lunch were representatives from organizations working with a range of key populations, including sex workers, men who have sex with men and transgender people.
Over lunch, Michel Sidibé heard about the issues and difficulties faced by these populations and the organizations which work to support them. Participants felt that civil society could make a far greater contribution to the response to AIDS, both in Shanghai and in China as a whole. Many felt that the Chinese government needed to work more closely with non-governmental organizations (NGOs) and other civil society partners to provide services and gain access to key populations such as sex workers and drug users. These key populations are often highly reluctant to seek services or accept help from government bodies, particularly due to the fact that they are often criminalised, and therefore remain cut off from vital prevention, treatment and care services.
Michel Sidibé discussed these issues and expressed his agreement, stressing the critical importance of NGO involvement in national AIDS responses, including meaningful participation in policy formulation and implementation of prevention, treatment and care services. Michel commended the participants for the work they were carrying out. He told them that “achieving social change and challenging strongly-held attitudes is not an easy task, and requires time, patience and commitment,” but encouraged them to continue to strive to achieve these important goals.
UNAIDS Executive Director visit to China opens wi


Feature Story
Education sector: Getting to grips with an HIV monitoring and evaluation framework
23 November 2009
23 November 2009 23 November 2009Credit: UNAIDS/L. Taylor
The education sector plays a critical role in national responses to the HIV epidemic. However, this contribution is often poorly appreciated and understood due to limited, difficult-to-measure data and the absence of agreement on core indicators for the sector.
To assist ministries of education and their partners in measuring progress and outcomes of related efforts, a host of international experts met in London on 9-10 November to develop a monitoring and evaluation (M&E) framework for education sector responses to AIDS. This framework aims to assist ministries of education and other partners in outlining and measuring the main programme outputs and outcomes of the education sector, facilitating the development of effective, results-focused interventions.
Convened by the Partnership for Child Development (PCD) of Imperial College, on behalf of the Indicators Working Group of the UNAIDS Inter-Agency Task Team (IATT) on Education, the experts attending the meeting included individuals with significant expertise in M&E, in education sector responses and with a great deal of programme experience. Programme managers from Southern Africa, Latin America and the Caribbean, and South and South-East Asia attended.
Getting things right in the education sector’s monitoring and evaluation of its response to HIV is essential if it is to provide a ‘social vaccine’ to the epidemic, offering knowledge and personal skills which can prevent HIV.
Michael Beasley, director of Partnership for Child Development at Imperial College London
The meeting built on a review of existing indicators used to monitor education sector HIV responses undertaken by PCD on behalf of the UNAIDS IATT on Education Indicators Working Group. It also contributed to an effort underway by a wide range of partners associated with the FRESH (Focusing Resources on Effective School Health) Initiative to develop an M&E framework for school-based health and nutrition and HIV prevention interventions.
As well as reaching agreement on appropriate priorities for the monitoring and evaluation of the sector’s work, the meeting also achieved consensus on prioritising indicators that could be used.
Indicators examined included those helping the education sector address the following questions:
1. Within the context of a national AIDS response, is there a response in the education sector that is guided and enabled by policy, strategy and resources?
2. Is HIV, reproductive and sexual health education a timetabled subject delivered in schools? Is it mandatory and assessed? Are HIV-related life skills delivered through co-curricular means?
3. Are educators receiving pre-service and in-service training about HIV (for themselves) and about teaching HIV to students?
4. Is the education sector facilitating testing, treatment, care and support services for learners and educators? Are measures in place to make schools safe and protective environments?
In addition to indicators to measure these short-term outcomes, the group also considered intermediate outcomes such as knowledge about HIV and those of a long-term nature such as age of sexual debut.
The draft M&E framework and proposed indicators will be presented to the UNAIDS IATT on Education at its meeting on 2-4 December 2009 in Berlin, Germany. Anticipated next steps include field-testing the new proposed indicators, and refining the definitions of existing ones. This will be taken forward by members of the IATT on Education’s Indicators Working Group in early 2010, in consultation with ministries of education and national partners.
According to Michael Beasley, director of Partnership for Child Development at Imperial College, “Getting things right in the education sector’s monitoring and evaluation of its response to HIV is essential if it is to provide a ‘social vaccine’ to the epidemic, offering knowledge and personal skills which can prevent HIV.” He added, “It is estimated that young people who fail to complete a basic education are more than twice as likely to become infected as those who do. Education also reduces the vulnerability of girls, and each year of schooling offers greater protective benefits.”
Empowering young people to protect themselves from HIV is one of the nine priority areas for UNAIDS and its Cosponsors under the Joint Action for Results: UNAIDS Outcome Framework 2009-2011.
Formed in 2002, the UNAIDS IATT on Education is convened by UNESCO and brings together UNAIDS Cosponsors and other multilateral organisations, bilateral agencies, private donors and civil society partners with the purpose of accelerating and improving a coordinated and harmonised education sector response to HIV.
Education sector: Getting to grips with an HIV mo
Cosponsors:
Feature stories:
China’s vocational schools play a key role in AIDS education (16 October 2009)
UNAIDS Task Team develops effective tools to help young people tackle HIV (05 June 2009)
HIV response and the education sector: UNESCO Best practice series (04 May 2009)
Publications:
A review conducted on behalf of the UNAIDS IATT on Education Indicators Working Group (pdf, 508 Kb.)
A Strategic Approach: HIV & AIDS and Education UNAIDS IATT on Education, 2008 (pdf, 2.44 Mb.)
Toolkit for Mainstreaming HIV and AIDS in the Education Sector: Guidelines for Development Cooperation Agencies. (UNAIDS IATT on Education, 2008) (pdf, 1 Mb.)
Related



Feature Story
Business coalitions on AIDS strengthen the private sector response to AIDS in Asia
23 November 2009
23 November 2009 23 November 2009
Participants at the second regional meeting of Business coalitions held on Bangkok, Thailand on November 17-18 2009.
Credit: UNAIDS
Business coalitions on AIDS (BCA) have emerged as an effective platform for the private sector to respond to the HIV epidemic and strengthen their corporate social responsibility efforts.
In order to take stock of progress made by BCAs in the Asia Pacific region and to ensure that standards are upheld as services are scaled up by BCAs, UNAIDS, the Asia Pacific Business Coalition (APBCA) and the Asian Business Coalition on AIDS (ABCA) organized a regional meeting of BCAs from the region in Bangkok, Thailand on November 17-18 2009.
"The meeting of business coalitions in the Asia Pacific region has been a tremendous opportunity for the coalitions to learn from each other and find ways to enhance the private sector's contribution in the AIDS response," said Stephen Grant, Asia Pacific Business Coalition on AIDS Chief Executive Officer.
Over twenty participants gathered to discuss key issues around the activities and services offered by BCAs in the region, the challenges and opportunities they face as well as key partnerships and relationships developed with national and international stakeholders. Participants also analyzed the impact and value of BCA, their business models (membership and funding models), organizational structures and governance, and the advocacy work they do.
Strengthening the private sector response to AIDS
Although some companies are already addressing HIV in the workplace, others do not know how or what to do to start mitigating risks. Business coalitions have emerged to fill this gap and provide the private sector with tools and processes needed to effectively address HIV in the workplace and surrounding communities. The comprehensive business responses can be seen in corporate policies for HIV management. Businesses focus on prevention through peer education, provision of antiretroviral treatment and support for affected staff and their dependants.
"People who are at the core of the epidemic include men who are mobile and who practice sex with multiple partners. Many of them are workers who are employed by thousands of businesses and industrial establishments across Asia and the Pacific. Accessing them through well planned workplace programmes is a good way to counter the epidemic and business coalitions are well placed to assume leadership in this area," said Prasada Rao, UNAIDS Regional Director for Asia and Pacific.
Business responses can start within the workplace and respond beyond to form mature partnerships with business, business associations, and communities as well as governmental authorities to form a private public partnership, which will enhance society’s efforts to combat the epidemic.
The workshop was attended by coalitions from Cambodia, Indonesia, Malaysia, Myanmar, PNG, Singapore, Thailand, and Vietnam, the regional coalitions (Asia Pacific Business Coalition (APBCA) and the Asian Business Coalition on AIDS (ABCA) as well as private sector representatives from Bangladesh, Indonesia, Nepal, Philippines and Sri Lanka. The Asia Pacific Network of people living with HIV/AIDS, the Global Fund, ILO, the Burnet Institute (the leading medical research and public health Institutes in Australia) and the HIV Alliance also participated.
One of the deliverables of the meeting will be a manual designed to help BCAs set priorities and next steps. It will guide BCAs on where to seek technical assistance (and what type) to address hurdles, on how to ensure they promote sustainable programs in support of the national AIDS response and target the most vulnerable communities, etc.
The first established Business coalition on AIDS (BCA) was launched in Thailand in 1993. Today, there are 47 coalitions around the world that have emerged and four regional business coalitions. In most countries in Asia Pacific, BCA now exist in various forms and in different stages of development.
This second regional meeting was a follow up to the 2003 meeting on BCAs which took place in Bali and brought together 55 participants from 11 countries – Cambodia, China, Fiji, Indonesia, Kiribati, Philippines, Papua New Guinea, South Africa, Thailand and Viet Nam.
Business coalitions on AIDS strengthen the privat
Esternal links:
Asia Pacific Business Coalition
Asia Business Coalition
ILO/AIDS
Related
Feature Story
Acclaimed photo exhibition by women living with HIV opens in New York
20 November 2009
20 November 2009 20 November 2009 “Circle in the sun” from The House is Small but the Welcome is Big exhibition
“Circle in the sun” from The House is Small but the Welcome is Big exhibition Credit: www.thehouseissmall.org/Aires
On 17 November UNAIDS hosted a reception for the opening of an exhibition at the United Nations in New York entitled The House Is Small But The Welcome Is Big, a project of the Los Angeles–based Venice Arts of over 40 extraordinary photographs made by South African women living with HIV and Mozambican children who lost both parents to AIDS.
The exhibit, which runs until 11 December, sheds light on the hopes and aspirations of people affected by the epidemic, as well as the discrimination and stigma associated with HIV.
Accompanied by biographical panels, the exhibit conveys the daily lives of 15 women and 18 children who face tremendous challenges because of HIV. The photos are simultaneously stark and hopeful, lively and compelling. Some are difficult to look at. All of them are hard to dismiss.
The exhibit evokes the words of United Nations Secretary-General Ban Ki–moon: “HIV is about everyone. It is not about ‘us versus them’. There is no ‘them’ – only ‘us’, together.”
Bertil Lindblad, Director of the UNAIDS New York Office
Bertil Lindblad, Director of the UNAIDS New York Office, said that the exhibit evokes the words of United Nations Secretary-General Ban Ki–moon: “HIV is about everyone. It is not about ‘us versus them’. There is no ‘them’ – only ‘us’, together.” The exhibit is one of many events worldwide commemorating World AIDS Day on 1 December.
 “The Mozambican handshake” from The House is Small but the Welcome is Big exhibition
“The Mozambican handshake” from The House is Small but the Welcome is Big exhibition Credit: www.thehouseissmall.org/Farida
Neal Baer, M.D., Emmy-nominated writer/executive producer of the television series Law & Order: Special Victims Unit and a co-founder of the project, commented “These women and children have a lot to say through these images about living on their own and raising younger siblings by themselves,” said Baer. “That’s the harsh truth about AIDS. Millions of children are growing up without the guidance or love of one or both parents, with many carrying parental responsibilities.” Law & Order: Special Victims Unit star Stephanie March joined Dr Baer at the event.
Also attending the reception was Ambassador Baso Sangqu, Permanent Representative of South Africa to the United Nations.
The name of the exhibition comes from one of the photographs taken by 28 year-old Funeka Nceke of Cape Town. On the wall of her friend’s home hangs an embroidered cloth that reads, “The House Is Small But the Welcome Is Big.” Funeka lives in a shack with no electricity or running water with her two children and two additional family members.
One beautiful photograph titled “My Memories” shows a pair of hands gently touching old black and white photographs. “Photographs of my parents are displayed, which show their past. I show everyone my parents [when they were] alive through these photos, which is a joy for me,” says Joaquim Macamo, the 16 year-old photographer. Macamo lost both of his parents to AIDS in 2001 and lives with his 20 year-old sister.
The exhibit has been featured at venues around the world, including New York City; Los Angeles, Oakland, and Palo Alto, CA; Boston, MA; Colorado Springs and Denver, CO; Tallahassee, FL; Maputo, Mozambique; Toronto, Canada; Mexico City, Mexico; and Paris, France.
Award–winning Venice Arts has run innovative programs in documentary photography, filmmaking, and digital media/arts since 1993. The organization also implements participant-produced photo documentary projects with adults and children, and co–directs the Institute for Photographic Empowerment in collaboration with the University of Southern California Annenberg Center for Communication Leadership.
Acclaimed photo exhibition by women living with H
Partners:
The House is Small but the Welcome is Big
Feature stories:
Artists in Russia come together to spread awareness about HIV (18 November 2009)
Related

Feature Story
Michel Sidibé awarded Monaco distinction by His Serene Highness Prince Albert II
19 November 2009
19 November 2009 19 November 2009
His Serene Highness Prince Albert II of Monaco (right) awards UNAIDS Executive Director Michel Sidibé the Order of Saint Charles. Monaco, 18 November 2009.
Copyright: G. Luci-Palais Monaco
UNAIDS Executive Director Michel Sidibé was awarded the Order of Saint Charles along with UNESCO Director-General Koïchiro Matsuura in the Principality of Monaco during the country’s National Day.
The order rewards merit and service to the state or Prince of Monaco and is one of the country’s most prestigious distinctions.
The medal was awarded in the presence of His Serene Highness Prince Albert II of Monaco, Her Royal Highness Princess Caroline of Hanover and Her Serene Highness Princess Stéphanie.
Expressing his appreciation for the award, Mr Sidibé emphasized the importance of Monaco’s efforts in the response to the AIDS epidemic, noting Monaco’s financial contribution to the response in priority countries Madagascar and Burundi and the personal commitment of the royal family.
Her Serene Highness Princess Stéphanie, Goodwill Ambassador for UNAIDS, has been working with the organization since 2006 focusing on HIV prevention and raising awareness on the impact of discrimination against people living with HIV.
Mr Sidibé praised the leadership of Her Serene Highness in her work to increase the visibility of issues related to AIDS.
During his last visit to the country in May 2009, Mr Sidibé renewed the existing funding agreement between UNAIDS and Monaco until 2011.
Michel Sidibé awarded Monaco distinction by His S
Cosponsors:
Press centre:
Feature stories:
Michel Sidibé, UNAIDS Executive Director visits the Principality of Monaco (29 May 2009)
UNAIDS and Principality of Monaco commit to strengthened cooperation in AIDS response (29 May 2009)
Related



Feature Story
UNFPA report: Exploring links between HIV and climate change
18 November 2009
18 November 2009 18 November 2009
State of the Worlds Population, 2009
Credit: UNFPA
The success of the global response to AIDS will rely on tackling not only the encroaching virus itself but also the affects of climate change such as food and water shortages, growth in poverty and an increase in natural disasters, argues the State of World Population 2009, released today by the United Nations Population Fund (UNFPA).
The report also contends that, equally, strengthening the response to the AIDS epidemic will mean that individuals, communities and societies will have greater social resilience in the face of a range of climate change threats and will be better able to deal with their consequences. HIV and climate change are perceived as profoundly linked, a perception shared by a range of UN bodies, including UNAIDS and the United Nations Environment Programme, UNEP.
Subtitled, ‘Facing a changing world: women population and climate’, The State of World Population places women at the very centre of the attempt to confront climate change and maintains that policies, programmes and interventions are more likely to mitigate its worst effects if they reflect the rights and needs of women.
Poor women in poor countries are among the hardest hit by climate change, even though they contributed the least to it.
UNFPA Executive Director Thoraya Ahmed Obaid
Women are said to bear the brunt of climate change, partly because in many countries they make up the majority of the agricultural workforce hard hit in an environmental crisis, and because they often do not have sufficient control of their lives and access to as many opportunities to generate income as men – they are more likely to be poor and to see their poverty increase. As UNFPA Executive Director Thoraya Ahmed Obaid has it, “Poor women in poor countries are among the hardest hit by climate change, even though they contributed the least to it.”
Numerous examples of extreme climate change are cited, from melting glaciers in Bolivia, to the destruction of crops by typhoons in the Philippines, and from drought in east and southern Africa to floods in Vietnam. In each scenario, women are shown struggling to keep their livelihoods and families intact, and, in some cases, fighting for their lives.
According to the report, empowering women and girls, especially through investments in health and education, help boost economic development and reduce poverty, thus having a beneficial impact on coping with climate change. Girls with more education are more likely to protect themselves against HIV and to have smaller and healthier families as adults. In general, access to reproductive health services such as family planning means lower fertility rates and this has a clear bearing on lessening the potential impact of environmental crises and making sustainable development more likely.
“Women should be part of any agreement on climate change—not as an afterthought or because it’s politically correct, but because it’s the right thing to do,” says Ms Obaid. “Our future as humanity depends on unleashing the full potential of all human beings, and the full capacity of women, to bring about change.”
The State of World Population 2009 argues that ensuring gender inequity is challenged in all its facets is an urgent necessity, not just to improve the lives of individual women but to stave off the worst consequences of environmental crisis. This sense of urgency is relayed to the leaders and negotiators due to meet in Copenhagen for December’s critical climate change conference. They are urged to “think creatively” not just about emissions and targets but about population, reproductive health and gender equality and how they can contribute to “a just and environmentally sustainable world.”
UNFPA report: Exploring links between HIV and cli
Cosponsors:
UNFPA
WHO: HIV
WHO: Gender, Women and Health
Partners:
UN Worldwide Campaign on Climate Change
The Global Coalition on Women and AIDS (GCWA)
Feature stories:
Food by Prescription: A Landscape paper from GAIN (16 November 2009)
Violence against women and HIV (10 November 2009)
WHO report on the health of women: AIDS leading cause of death globally in women of reproductive age (09 November 2009)
Examining links between AIDS and climate change (07 July 2009)
Publications:
The State of World Population 2009 ( fr | ru | ar )
State of World Population 2009: Youth supplement ( fr | ru | ar )
Women and Health: Today’s Evidence, Tomorrow’s Agenda



Feature Story
Artists in Russia come together to spread awareness about HIV
18 November 2009
18 November 2009 18 November 2009
Yulia Lasker, Russian singer, who purchased a tapestry at the opening of the exhibition.
Credit: UNAIDS
UNAIDS and the All-Russian Union of People Living with HIV came together for the second time to support the international project Art Against AIDS that unites well-known artists in the response to the HIV epidemic in Russia. This year, proceeds from the sale of art at the exhibition went to low-income families raising children living with HIV.
More than 30 contemporary artists, photographers, and musicians from Russia, the United States, Japan, Greece and Spain offered their work for the charitable exhibition-sale held at the Central House of Artists from 12 - 26 November 2009. Last year, funds raised during the exhibition-sale went to children living with HIV at the Vsevolozhsk Orphanage in Leningrad Oblast.
There is increasing political and financial commitment for universal access to HIV prevention, treatment and care in Russia, even in the face of a global financial crisis. The country is set to increase the number of people on antiretroviral treatment by 50,000 in 2009. Through this exhibition, artists, photographers and musicians are helping to speak openly about HIV and to draw the attention of the wider public towards this issue.

One of the art pieces sold at the launch of Art Against AIDS on the 12 of November.
Credit: UNAIDS
Earlier in October during the 3rd HIV/AIDS Conference in Eastern Europe and Central Asia, UNAIDS Executive Director Michel Sidibé said that there has been progress in the region with many countries set to achieve universal access target goals. But the UNAIDS head also noted that the AIDS epidemic continues to outpace the response as the estimated number of adults and children living with HIV in the Eastern Europe and Central Asia region has doubled since 2001.
Injecting drug use is the main mode of HIV transmission across Eastern Europe and Central Asia. HIV prevention among drug users and their sexual partners is a vital component of an evidence-informed response. Although the HIV epidemic in the Russian Federation is the largest in the region, there are rising numbers in Azerbaijan, Georgia, Kazakhstan, Kyrgyzstan, the Republic of Moldova, Tajikistan, and Uzbekistan.
Artists in Russia come together to spread awarene
Key populations:
Cosponsors:
Feature stories:
“Artists Against AIDS” help fight stigma and discrimination in Russia (17 November 2008)
All-Russian Union of People Living with HIV (09 July 2009)
“Art for AIDS” receives Keith Haring sculptures (27 November 2008)
"Stars against AIDS" in Eastern Europe (19 May 2008)


