
Feature Story
Male Circumcision and HIV: the here and now (Part 2)
28 February 2007
28 February 2007 28 February 2007In the second of a special three-part series on the issue of male circumcision and its links to the reduction of HIV acquisition, unaids.org considers current research findings.
It’s a subject that hits headlines, fuels discussions, sparks debate and causes some of the men in the room to wince and cross their legs. Male circumcision and its links to HIV is one of the most talked about issues within the AIDS response over the last years, with latest research findings driving potential change in the way male circumcision is practiced and implemented for the future in relation to HIV prevention.
In scientific circles, the perceived links between male circumcision and HIV infection are nothing new. For years, AIDS researchers have observed that many African tribes that circumcise boys or young men had lower HIV rates than those that do not, and that Africa's Islamic nations, where circumcision is near universal, had far fewer AIDS cases than predominantly Christian ones.
Now, trials in Kenya, Uganda and South Africa have all shown that male circumcision significantly reduces a man’s risk of acquiring HIV. The three sets of trials have shown circumcised men are up 50 to 60% less likely to acquire HIV during heterosexual intercourse.
Research findings
The first research proof came in 2005, when a study in South Africa, supported by the French agence nationale de recherches sur le sida (ANRS) and known as the 'Orange Farm Intervention Trial', was stopped early in the face of evidence that the men who had been randomly assigned to be circumcised were getting 60% fewer HIV infections than the men assigned to the control group.
In December 2006, on the recommendation of their Data and Safety Monitoring Board (DSMB), two similar studies in Uganda and Kenya were halted early by the United States National Institutes of Health (NIH) because the interim results showed a significant effect of male circumcision in preventing HIV acquisition in men.
The trial carried out in Kisumu, Kenya by researchers from the University of Nairobi, University of Illinois at Chicago, the University of Manitoba, and RTI International involving 2,784 men aged 18 to 24 showed a 53% reduction of HIV infections in circumcised men compared to uncircumcised men.
In Uganda, the trial, carried out in Rakai by researchers from Makerere University, the Uganda Virus Research Institute, Johns Hopkins University, and Columbia University New York, involved 4996 men aged 15 to 49 years old and showed that adult male circumcision reduced by 51% the risk of becoming infected with HIV.
Dr. Anthony Fauci, director of the NIH's National Institute of Allergy and Infectious Diseases, said the institute ended both trials early and offered circumcision to all men involved in them. The trials began in 2005 and were due to go until mid-2007.
The biology
Male circumcision involves the surgical removal of the foreskin, the tissue covering the head of the penis. Previous research shows that removing the foreskin is associated with a variety of health benefits including lower rates of urinary tract infections in male infants who are circumcised and reduced risk of certain inflammations and health problems associated with the foreskin.
Scientists say male circumcision probably reduces the risk of HIV infection because it removes tissue in the foreskin that is particularly vulnerable to the virus, and because the area under the foreskin is easily scratched or torn during sex. “Uncircumcised men may also be more vulnerable to sexually transmitted diseases, which in turn increase the risk of contracting HIV, because the region under the foreskin provides a moist, dark place in which germs can thrive,” said UNAIDS Chief Scientific Adviser, Dr Catherine Hankins.
No ‘magic bullet’
The results of the trials in South Africa, Uganda and Kenya indicate that in certain settings, adult male circumcision could become an important addition to an HIV prevention strategy for men. “The trials indicate that male circumcision can lower both an individual's risk of infection and hopefully the rate of HIV spread through the community," NIH’s Dr Fauci said.
But experts— including the United Nations bodies working on the issue—caution that circumcision is no cure-all. Male circumcision does not provide complete protection against HIV infection; it only lessens the chances that a man will acquire the virus.
Circumcision is "not a magic bullet, but a potentially important intervention," said Dr. Kevin M. De Cock, director of the World Health Organization’s AIDS department.
“Men and women must understand that circumcised men can still become infected with the virus and if HIV-positive, can infect their sexual partners,” said UNAIDS’ Dr Hankins
“ Male circumcision should never replace other known effective prevention methods and should always be considered as part of a comprehensive HIV prevention package, which includes correct and consistent use of male or female condoms, reduction in the number of sexual partners, delaying the onset of sexual relations, and abstaining from penetrative sex”, she said.
Safety, sanitation and communication
To ensure safe and clean operations, male circumcision should only be performed by well-trained practitioners in sanitary settings under conditions of informed consent, confidentiality, proper counseling and safety. “If male circumcision is to be promoted, this should be done in a culturally appropriate manner and people should be provided sufficient and correct information on HIV prevention to prevent them from developing a false sense of security and engaging in risky behavior,” said Dr Hankins.
These considerations and others in relation to the AIDS response, including the fact that male circumcision has the potential to be an expensive intervention, that more research is needed to address whether male circumcision reduces risk of transmitting HIV-particularly for female partners, and the different ethical and human rights issues raised by male circumcision, will form discussions of the United Nations consultation on male circumcision that will take place in Geneva from 5 March. Here, WHO, the UNAIDS Secretariat and their partners will review the detailed trial findings and will, if deemed appropriate, then define specific policy recommendations for expanding and/or promoting male circumcision.
“Male circumcision is a complicated issue which involves sometimes difficult discussion on issues of culture, tradition, religion, ethnicity, human rights and gender. The consultation will provide an excellent arena for moving the discussion and policy forward within the United Nations,” said Dr Hankins.
Male Circumcision: context, criteria and culture (Part 1)
Male Circumcision and HIV: the here and now (Part 2)
Moving forwards: UN policy and action on male circumcision (Part 3)
Related



Feature Story
Male Circumcision: context, criteria and culture (Part 1)
26 February 2007
26 February 2007 26 February 2007With male circumcision and its links to HIV acquisition hitting the headlines and sparking debates around the world, in the first of a special three-part series on the issue, www.unaids.org takes a closer look at the historical, traditional and increasingly social reasons behind the practice of male circumcision across the world.
Male circumcision is one of the oldest and most common surgical procedures known, traditionally undertaken as a mark of cultural identity or religious importance.
Historically, male circumcision was practised among ancient Semitic people including Egyptians and those of Jewish faith, with the earliest records depicting circumcision on Egyptian temple and wall paintings dating from around 2300 BC.
With advances in surgery in the 19th century, and increased mobility in the 20th century, the procedure was introduced into some previously non-circumcising cultures for both health-related and social reasons.
According to current estimations, approximately 30% of all males across the world— representing a total of approximately 670 million men — are circumcised. Of this number, about 68% are of Islamic faith, less than 1% of Jewish faith, and 13% are non-Muslim, non-Jewish Americans.
“With the recent findings that male circumcision significantly reduces a man’s risk of acquiring HIV the practice is receiving renewed interest as the world looks to understand what this will mean for HIV prevention,” said UNAIDS Chief Scientific Adviser, Dr Catherine Hankins. “Looking at the determinants of male circumcision, and the acceptability of male circumcision in non-circumcising societies give a better picture of how to take the latest research findings forward.”
Religious practice
In the Jewish religion, male infants are traditionally circumcised on their eighth day of life, providing there is no medical contraindication. The justification, in the Jewish holy book the Torah, is that a covenant was made between Abraham and God, the outward sign of which is circumcision for all Jewish males. The Torah states: “ This is my covenant, which ye shall keep, between me and you and thy seed after thee: every male among you shall be circumcised " (Genesis 17:10). Male circumcision continues to be almost universally practiced among Jewish people.
Islam is the largest religious group to practice male circumcision. As an Abrahamic faith, Islamic people practice circumcision as a confirmation of their relationship with God, and the practice is also known as ‘tahera’, meaning purification. With the global spread of Islam from the 7th century AD, male circumcision was widely adopted among previously non-circumcising peoples. There is no clearly prescribed age for circumcision in Islam, although the prophet Muhammad recommended it be carried out at an early age and reportedly circumcised his sons on the seventh day after birth. Many Muslims perform the rite on this day, although a Muslim may be circumcised at any age between birth and puberty.
The Coptic Christians in Egypt and the Ethiopian Orthodox Christians— two of the oldest surviving forms of Christianity— retain many of the features of early Christianity, including male circumcision. Circumcision is not prescribed in other forms of Christianity. In the New Testament, St. Paul wrote: "in Christ Jesus neither circumcision nor uncircumcision count for anything" (Galatians 5:6) and a Papal Bull issued in 1442 by the Roman Catholic Church stated that male circumcision was unnecessary: “Therefore it strictly orders all who glory in the name of Christian, not to practise circumcision either before or after baptism, since whether or not they place their hope in it, it cannot possibly be observed without loss of eternal salvation,” it stated. Focus group discussions on male circumcision in sub-Saharan Africa found no clear consensus on compatibility of male circumcision with Christian beliefs. Some Christian churches in South Africa oppose the practice, viewing it as a pagan ritual, while others, including the Nomiya church in Kenya, require circumcision for membership and participants in focus group discussions in Zambia and Malawi mentioned similar beliefs that Christians should practice circumcision since Jesus was circumcised and the Bible teaches the practice.
Ethnicity
Circumcision has been practiced for non-religious reasons for many thousands of years in sub-Saharan Africa, and in many ethnic groups around the world, including aboriginal Australasians, the Aztecs and Mayans in the Americas, inhabitants of the Philippines and Eastern Indonesia and of various Pacific Islands, including Fiji and the Polynesian islands.
In the majority of these cultures, circumcision is an integral part of a rite-of-passage to manhood, although originally it may have been a test of bravery and endurance. “Circumcision is also associated with factors such as masculinity, social cohesion with boys of the same age who become circumcised at the same time, self-identity and spirituality,” Dr Hankins explained.
The ethnographer Arnold Van Gennep in his 1909 work ‘The Rites of Passage’ , describes various initiation rites which are present in many circumcision rituals. These include a three stage process: separation from normal society; a period during which the neophyte undergoes transformation; and finally reintegration into society in a new social role.
“A psychological explanation for this process is that ambiguity in social roles creates tension, and a symbolic reclassification is necessary as individuals approach the transition from being defined as a child to being defined as an adult. This is supported by the fact that many rituals attach specific meaning to circumcision which justify its purpose within this context,” said Dr Hankins. For example, certain ethnic groups including the Dogon and Dowayo of West Africa, and the Xhosa of South Africa view the foreskin as the feminine element of the penis, the removal of which (along with passing certain tests) makes a man of the child.
Tradition plays a major part for many ethnic groups. Among ethnic groups of Bendel State in southern Nigeria, 43% of men stated that their motivation for circumcision was to maintain their tradition. In some settings where circumcision is the norm, there is discrimination against non-circumcised men. For the Lunda and Luvale tribes in Zambia, or the Bagisu in Uganda, it is unacceptable to remain uncircumcised, to the extent that forced circumcisions of older boys are not uncommon. Among the Xhosa in South Africa, men who have not been circumcised can suffer extreme forms of punishment, including bullying and beatings.
Circumcision as a social statement
Social reasons behind male circumcision are becoming ever more common. “The desire to conform is an important motivation for circumcision in places where the majority of boys are circumcised,” said Dr Hankins.
A survey in Denver, US where circumcision occurs shortly after birth, found that parents, especially fathers, of newborn boys cited social reasons as the main determinant for choosing circumcision (e.g. not wanting the son to ‘look different’ from the father).
In the Philippines, where circumcision is almost universal and typically occurs at age 10-14, a survey of boys found two-thirds of those surveyed choosing to be circumcised simply ‘to avoid being uncircumcised’, and 41% stating that it was ‘part of the tradition’. Social concerns were also the primary reason for circumcision in South Korea with 61% of respondents in one study believing they would be ridiculed by their peer group unless they were circumcised.
The desire to ‘belong’ is also likely to be the main factor behind the high rate of adult male circumcisions among immigrants to Israel from non-circumcising countries (predominantly the former Soviet Union).
In a number of countries, socio-economic factors also influence circumcision prevalence, especially in countries with more recent uptake of the practice such as English-speaking industrialised countries. When male circumcision was first practised in the United Kingdom in the late 19th and early 20th century, it was most prevalent among the upper classes. In the US, a review of 4.7 million newborn male circumcisions nationwide between 1988 and 2000 also found a significant association with private insurance and higher socioeconomic status.
Perceived health and sexual benefits
In more recent times, perceptions of improved hygiene and lower risk of infections through male circumcision have driven the spread of circumcision practices in the industrialised world.
In a study of US newborns in 1983, mothers cited hygiene as the most important determinant of choosing to circumcise their sons, and in Ghana, male circumcision is seen as cleansing the boy after birth. Improved hygiene was also cited by 23% of 110 boys circumcised in the Philippines and in South Korea, the principal reasons given for circumcision were ‘to improve penile hygiene’ (71% and 78% respectively) and to prevent conditions such as penile cancer, sexually transmitted diseases and HIV. In Nyanza Province, Kenya, 96% of uncircumcised men and 97% of women irrespective of their preference for male circumcision stated their opinion that it was easier for circumcised men to maintain cleanliness.
Perceived improvement of sexual attraction and performance can also motivate circumcision. In a survey of boys in the Philippines, 11% stated that a determinant of becoming circumcised was that women like to have sexual intercourse with a circumcised man, and 18% of men in the study in South Korea stated that circumcision could enhance sexual pleasure. In Nyanza Province, Kenya, 55% of uncircumcised men believed that women enjoyed sex more with circumcised men. Similarly, the majority of women believe that women enjoyed sex more with circumcised men, even though it is likely that most women in Nyanza have never experienced sexual relations with a circumcised man. In northwest Tanzania, younger men associated circumcision with enhanced sexual pleasure for both men and women, and in Westonaria district, South Africa, about half of men said that women preferred circumcised partners.
Expected increase in demand
Global estimates in 2006 suggest that about 30% of males — representing a total of approximately 670 million men — are circumcised.
With latest research findings suggesting that circumcised men have a significantly lower risk of becoming infected with HIV, demand for safe, affordable, male circumcision is expected to increase rapidly.
“Since male circumcision is now shown to be effective in reducing the risk of HIV acquisition, care must be taken to ensure that men and women understand that the procedure does not provide complete protection against HIV infection,” said Dr Hankins, underlining that these issues will be discussed at the “ Male Circumcision and HIV Prevention Research - Policy and Programme Implications” International Consultation to be held in Montreux from 6-8 March 2007. “Male circumcision must be considered as just one element of a comprehensive HIV prevention package that includes the correct and consistent use of male or female condoms, reductions in the number of sexual partners, delaying the onset of sexual relations and abstaining from penetrative sex. Just as combination treatment is the best strategy to treat HIV, combination prevention is the best strategy to avoid acquiring or transmitting HIV”, she added.
“Action is also required to improve the safety of circumcision practices in many countries and to ensure that health care providers and the public have up-to-date information on the health risks and benefits of male circumcision,” she said.
Links:
Read Part 2 - Male Circumcision and HIV: the here and now
Read Part 3 - Moving forward: UN policy and action on male circumcision
Related
Feature Story
Male circumcision and HIV: a web special series
23 February 2007
23 February 2007 23 February 2007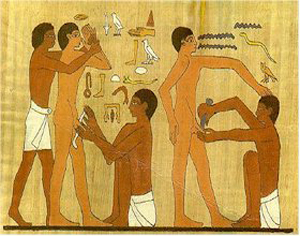
Male circumcision is one of the world’s oldest surgical practices; carvings depicting circumcisions have been found in ancient Egyptian temples dating as far back as 2300 BC.
In recent months, the issue of male circumcision and its links to the transmission of HIV has hit the headlines and sparked debates across the world. Trials in Kenya, Uganda and South Africa have now all shown that male circumcision significantly reduces a man’s risk of acquiring HIV.
As UNAIDS, the World Health Organization and other partners prepare to look at how to take these findings forward, in terms of UN guidance to countries on policy and programming, at a consultation to be held in Geneva from 5-8 March 2007, www.unaids.org takes an in-depth look at the issue of male circumcision in a special three-part series. Where did male circumcision originate, who practices it and why? These questions and others relating to the history and determinants of male circumcision will be considered in part one of the series – ‘Male Circumcision: context, criteria and culture’, published on Monday 26 February. On Wednesday 28 February, part two –‘Male circumcision and HIV: The here and now’ will summarize current research findings on male circumcision and HIV acquisition. Part three, to be published on Friday 2 March will discuss future action and developments from the United Nations and feature a special interview with UNAIDS Chief Scientific Adviser, Dr Catherine Hankins.
Male Circumcision: context, criteria and culture (Part 1)
Male Circumcision and HIV: the here and now (Part 2)
Moving forwards: UN policy and action on male circumcision (Part 3)
Related
Feature Story
HIV and refugees
23 February 2007
23 February 2007 23 February 2007
According to the 1951 Convention relating to the Status of Refugees, "A refugee is a person who, owing to a well-founded fear of persecution for reasons of race, religion, nationality or political opinion, is outside the country of his nationality and is unable or, owing to such fear, unwilling to avail himself of the protection of that country". Conflict,
persecution and violence affect millions of people worldwide, forcing them to uproot their lives and seek refuge in a different country.
At the end of 2005, there were 8.4 million refugees worldwide. Of these, approximately 30% were in sub-Saharan Africa, 29% in Central and South-West Asia, North Africa and the Middle East and 23% in Europe.
Displacement of people from their country of origin has an enormous effect on their lives, as well as upon the lives of host communities.
Conflict and displacement make women and children highly vulnerable to the risk of HIV. As refugees struggle to meet their basic needs such as food, water and shelter, women and girls are often forced to exchange sexual services for money, food or protection.

“Women and girls are often disproportionately affected by displacement. They need special attention in terms of HIV including protection from violence and exploitation,” said Dr. Purnima Mane, Director of Policy, Evidence and Partnerships at UNAIDS.
Among other problems, refugees often do not have access to HIV prevention commodities and programmes. Access to basic HIV-related care and support is also rarely given adequate attention. Despite improvements in the availability of antiretroviral therapy in low- and middle-income countries, very few refugees have access to it.
“We advocate for refugees to access HIV services in the same manner as that of the local population. Some countries in Southern Africa provide both refugees and the host population free antiretroviral drugs using Government services,” said Dr. Paul Spiegel, Head of HIV Unit, United Nations High Commissioner for Refugees (UNHCR).
Many host countries are already overburdened by the impact of HIV, and are often unable or unwilling to provide the HIV-related services refugees need and to which they have a right under international refugee and human rights law.

In order to reduce the risk of HIV infection and improve access to HIV-related prevention, treatment, care and support of refugees, UNAIDS in collaboration with one of its Cosponsors, UNHCR, has developed a new policy brief that focuses specifically on actions required to prevent HIV and mitigate the effect of HIV on refugees and their host communities.
The policy brief focuses on emergency and post-emergency phases and suggests actions for governments, civil society and international partners in order to ensure that refugee and human rights laws are applied, and that the needs of refugees are included into national HIV policies and programmes.
All photo credit: UNAIDS



Feature Story
UNAIDS at country level
21 February 2007
21 February 2007 21 February 2007
In 2005 and early 2006, the landscape of the AIDS response shifted dramatically. Global pessimism over the unchecked spread of the disease in the developing world receded in the face of impressive efforts to expand access to treatment. Signs that prevention efforts were bearing fruit were seen in a growing number of countries from the hardest-hit regions, which started to report drops in HIV rates, particularly among the young.
The global community had responded to urgent appeals by enormously increasing the financial resources available to fight the disease.
While millions continued to die annually, these developments gave rise to hope that there was a light at the end of the tunnel. Unimaginable even a year or two earlier, it was now possible to start talking about the prospects of providing access to HIV prevention, treatment, care and support services to all who needed them.
During this period, UNAIDS focused its country support work on two main areas. The first was improving the architecture of the AIDS response in the face of increasing complexity, growing resources and the involvement of new actors. This consisted of assisting countries in translating three key principles—the “Three Ones” of one national AIDS action framework, one coordinating authority and one monitoring and evaluation system—into operational reality. This focus was enabled by the Global Task Team on Improving AIDS Coordination Among Multilateral Institutions and International Donors, a high-level international discussion on how to streamline and better coordinate external support to national AIDS programmes.
The second priority of country work was securing political commitment to a dramatic expansion of services for prevention, treatment, care and support. Through the universal access process, countries and regions assessed the current state of the epidemic, identified barriers preventing the expansion of services and began to develop roadmaps to considerably expand key services.
Meanwhile, the core work of the UNAIDS Secretariat and Cosponsors continued unabated, with technical support being provided for the roll-out of antiretroviral treatment programmes, the procurement of key prevention commodities such as condoms, the training of teachers and youth peer educators and the drafting of policy reforms to help address stigma and discrimination against people living with HIV.
This period also saw an increasing emphasis on the importance of understanding the regional dimensions of the AIDS epidemic, both in how the disease is spreading in different ways in different parts of the world, and in how to better share lessons learnt across similar countries.
This publication examines the country-level work of UNAIDS in 2005 and early 2006 within the context of regional and global efforts to move towards universal access. Rather than chronicle every effort undertaken by UNAIDS at country level, this report discusses the major centres of work and illustrates them through examples from specific countries.
Links:
Download full report (pdf, 1.33 Mb)
Related


 Upholding dignity for everyone: Ariadne Ribeiro Ferreira
Upholding dignity for everyone: Ariadne Ribeiro Ferreira
21 November 2024
Feature Story
Be smart – protect yourself
14 February 2007
14 February 2007 14 February 2007
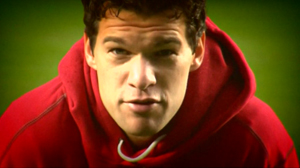
Photo credit: Al jazeera
Michael Ballack is known and admired across the world for his footballing skills but now Michael is going for a new goal and reaching out to young people around the globe by speaking about HIV prevention in a new UNAIDS public service announcement (PSA).
The PSA, generously produced by Al Jazeera, was filmed at Chelsea Football Club’s famous football ground Stamford Bridge, where Michael has been playing since his move from Bayern Munich in 2006.
Michael is helping people to make the smart choices and to help prevent the spread of HIV by appearing in the 30 second clip for UNAIDS. His message plays on sporting metaphors: ‘On the pitch you can play hard and take risks to score. But with HIV you are playing with your life––Be smart––protect yourself.’
"A lot of people know footballers, they look up to us, and I think we should all fight AIDS together,” said Michael Ballack while shooting the short film.
During the video, Ballack delivers key HIV prevention messages while demonstrating the footballing skills he is so famous for on the pitch. AIDS statistics are displayed on the stadium's big screen: ‘During the course of a 90 minute football match more than 500 people will have died of AIDS, 180 under 25 years old.’ After reading the statistics, Michael switches from player to referee: blowing his whistle, shaking his head and rather than holding out a red card he holds up a red condom. This epidemic must stop and there is one very simple way – HIV prevention!
Michael Ballack accepted his appointment as UNAIDS Special Representative in May 2006, pledging to raise awareness around HIV in the sporting arena. He said, “AIDS is everyone’s business. Sport and especially football can help break social barriers and fight the stigma around HIV.…I want today’s youth to know the facts about AIDS.”
Do you want to win a Ballack signed UNAIDS sweatshirt ?
Answer this question: “How many people were newly infected with HIV in 2006?”
Find the answer and more about HIV and AIDS on http://www.unaids.org/
Send your answer to competition@unaids.org with your name and postal address by March 31st 2007
The winners will be picked in a draw on April 2nd 2007. The winners will be notified directly by UNAIDS and the prizes will be shipped by mail.
Links:
Read statements from participants
Watch Michael Ballack's Public Service Announcement (PSA) (Video will open in a new window)
Read note to broadcasters
Go to Michael Ballack's UNAIDS Special Representative page
Related



Feature Story
Strengthening collaboration on AIDS
13 February 2007
13 February 2007 13 February 2007In recent years Spain has shown strong commitment to the AIDS response and has been working with UNAIDS on a broad range of AIDS and social development issues. Spain has shown particular commitment in several areas of the AIDS response including; reducing stigma and discrimination, promoting gender equality, improvements to health services and scaling-up HIV prevention efforts.
UNAIDS Executive Director was in Spain from 9-12 February to meet with government officials to discuss ways of enhancing collaboration and strengthening the response to the AIDS epidemic.
During his visit, Dr Piot met with the Spanish Minister of Health, Elena Salgado, in Madrid to discuss the ongoing collaboration between UNAIDS and the Spanish Government and to brief her on the latest developments in the AIDS response.

From L to R: The Basque Minister of Housing and Social Affairs, Javier Madrazo, UNAIDS Executive Director, Dr. Peter Piot and the Basque Minister of Health, Gabriel Inclán. Vitoria-Gasteiz, 12 February, 2007.
Dr Piot also travelled to the Basque Country where he met with leading members of the Basque Government including President Juan José Ibarretxe, the Minister of Health, Gabriel Inclán and the Minister of Housing and Social Affairs, Javier Madrazo.
Whilst in the Basque Country, Dr Piot signed a multi-year Cooperation Agreement between UNAIDS and the Basque Government. The agreement, the first of its kind between the two institiutions, outlines two specific areas of support and collaboration, the first being to enhance HIV prevention efforts in Central and Eastern Europe and the second to support UNAIDS in scaling-up the response to AIDS in Rwanda.
The Basque Government also announced plans to host a seminar on HIV prevention with global HIV experts to discuss ways of scaling HIV prevention efforts in Latin America, sub-Saharan Africa and Central and Eastern Europe.
During his visit, Dr Piot also met with civil society representatives and other professionals working on AIDS in the Basque region to learn more about their work.
During the discussions, Dr Piot stressed that it is one of UNAIDS’ key priorities to strengthen civil society engagement in the response to AIDS and to ensure that people living with HIV are equal partners in the process of scaling-up towards universal access to HIV prevention, treatment, care and support––from planning to implementation.
The visit wrapped up at the Guggenheim museum in Bilbao where Dr Piot spoke at an open conference on the future of Africa and the AIDS epidemic. The conference was organised by the museum as part of an educational programme to provide different visions of the African continent.
Links:
Guggenheim Museum Bilbao
Contemporary African art and AIDS
Related



Feature Story
Contemporary African art and AIDS
09 February 2007
09 February 2007 09 February 2007
African art has traditionally been perceived by western societies as being folklore or handicrafts. It wasn’t until late 20 th century that the so-called art critics reexamined the uniqueness of the contemporary African art, which finally found its place in the cultural conscience of western countries.
In 1986, one exhibition in Paris became pivotal in changing the perception of non-western contemporary art. The exhibition, called Magicians of the Earth, showed the works of contemporary artists from all continents. This event led to the creation of the Contemporary African Art Collection (C.A.A.C) by art collector Jean Pigozzi, who has become one of the major promoters of African art.

Pigozzi’s collection, one of the most important in the world, includes works of artists that live and work in sub-Saharan Africa who use different formats of expression ranging from paintings and sculptures to video and multi-media.
The importance of the collection and of most contemporary African art lies in the fact that artists have liberated themselves from the aesthetic tutelage imposed by western models and are able to express local or universal ideas with their own language, icons and formats.
African artists live and work closely in touch with their public and are aware of both local and global current affairs. Furthermore, the representation of collective problems has become a recurrent pattern which underlines the importance of the community in Africa.
Cheri Samba, one of the most famous Congolese painters, stated: “My art is part and parcel of my environment. It draws its inspiration from the people, it is concerned with the people, and it is meant for them”(1).
African art digs into its own reality, which makes artists the chroniclers of their times. Tradition, nature, myths and day-to-day life are sources of inspiration that shape the works of contemporary African artists. But common to all those artists, is the unavoidable influence that AIDS, and its impact on their societies, has in the conception of their art.
AIDS has shaped the lives of millions of people, especially in sub-Saharan Africa, and its impact it is embedded in the artists’ perceptions of their communities. Their works of art reflect in many ways the effects that the AIDS epidemic has on the societies they live in. However, art can and in fact should play an important role in the response to AIDS.
The proximity of African artists to their communities and the fact that they use a common language, place them in a privileged position to raise awareness of the epidemic as well as to provoke thought and dialogue around AIDS issues such as stigma and discrimination, poverty, gender and human rights.
UNAIDS Art for AIDS collection
In late 2006 UNAIDS launched the Art for AIDS collection in its new headquarters in Geneva, a building it shares with the World Health Organization.
“We are very fortunate to have art on loan from the Jean Pigozzi Geneva collection,” said Annemarie Hou, curator of the UNAIDS collection. “There are several pieces that have provoked hallway conversations and heated discussions—to hear people talk about the art was when we knew the collection was working.
”The UNAIDS’ Art for AIDS collection are museum quality pieces that provoke thought and dialogue. With an initial emphasis on African art and artists, the pieces have been assembled through the generous support of artists, collectors and donors.
All photo credit: O. O'Hanlon
(1) Cheri Samba, 100% Africa, TF Editores & FMGB Guggenheim Bilbao Museoa, Bilbao, 2006, p.142
Related



Feature Story
Traditional healers join the AIDS response
07 February 2007
07 February 2007 07 February 2007
UNAIDS/M.Jensen
African traditional medicine is often the primary, and frequently the only, accessible health-care option for many people living in sub-Saharan Africa.
Attempts to bring biomedical and traditional health care together for people living with HIV began in the early 1990s when the World Health Organisation recommended that traditional medicine be included in national responses to HIV.
“People all over the world have always sought advice from both biomedical doctors and traditional healers for all kinds of physical, emotional and spiritual problems. HIV is no exception” said Purnima Mane, Director of Policy, Evidence and Partnerships at UNAIDS. “It is our responsibility to ensure that people have access to the best possible care which they need and seek.” she added.

UNAIDS/L.Gubb
Early attempts to combine the best of both systems included a variety of projects that looked at the usefulness of traditional herbal remedies for the treatment of HIV-related illnesses. Studies looking at traditional healers’ perceptions of sexually transmitted infections and HIV infection were also conducted. With this information, collaborative projects began, training traditional healers as educators and counsellors to disseminate information on HIV and sexually transmitted infections in their communities and to their peers.
One such project involved the Inanda healers from the Valley of a Thousand Hills, Kwa-Zulu Natal, South Africa. In 2000, community leaders called for help in strengthening their response to the AIDS epidemic. They identified local traditional healers as having an important role to play. In response to their request, social scientists and medical doctors began working in partnership with the local traditional healers on HIV prevention projects.
A group of around 16-20 healers attended one-day monthly workshops where they learnt about HIV transmission, prevention, treatment and care. Discussions took place around traditional and cultural sexual practices that could prevent HIV transmission and safer sexual practices involving more than just condoms.
Herbal treatments such as Sutherlandia frutescens, also known as the ‘cancer bush’, which is produced in pill form and enhances appetite and immunity, were debated alongside other traditional medicines used by the healers.

WHO/UNAIDS/P.Virot
Coordination of the needs of the patient within a family and community context was an important part of the discussions. Traditionally, healers apply holistic healing approaches to problems and illnesses during their consultations, and whilst the patient remains the focus, equal importance is given to the socio-cultural background where the support network and the family interaction are essential.
“We must find more ways of facilitating and supporting the unique contribution healers can make to the response to AIDS,” said Andy Seale, Chief of Civil Society Partnerships at UNAIDS.
Through the regular meetings, the healers have established an informal support network and rely on each other for referral and resources. Increasingly, ways are being found to stimulate both referral networking with the formal health sector and with the traditional healers.
The ripples of the Inanda healers’ work have become increasingly widespread and more and more people are requesting HIV testing, counselling and support through the healers. There is hope in the Valley of a Thousand Hills and the commitment to make a difference.
As part of the best practice collection, UNAIDS has published practical guidelines to help health authorities develop productive relationships between traditional healers and moder biomedical professionals and strengthen the response to AIDS. http://data.unaids.org/Publications/IRC-pub07/JC967-TradHealers_en.pdf
Other Links:
UNAIDS "Best Practice Collection" - Learning from experiece

Feature Story
Fashionable jobs for people living with HIV
02 February 2007
02 February 2007 02 February 2007Latest styles, smartest colours and trendiest cuts will be central to an AIDS initiative in Algeria designed to help people living with HIV get back into the workplace.
The Algerian association of people living with HIV, El Hayet, has launched a pilot project for people living with HIV where participants will be trained in the production of haute-couture and prêt-à-porter clothing.
The training is led and designed by a professional dressmaker and the course will allow participants to learn about the tools and techniques of the fashion industry, in particular designing, model making, styling and sewing. Candidates who successfully complete the course will be able to obtain official recognition of their new trade from the National Chamber of Trade and Handicraft.

Zohira Merah, President of El Hayet with
workshop trainer Mr Redouane
The 12-month programme, which began in September 2006, is supported by the UNAIDS Secretariat and UNAIDS Cosponsors ILO and UNDP. The project has been made possible through grants from the Global Fund to fight AIDS, Tuberculosis and Malaria.
The initiative provides innovative economic opportunities for the participants, who will be paid for their work during the 12-month period. In addition, all the garments created during the course of the year will be sold with funds raised going to support people living with or affected by HIV in Algeria. “The economic element of this project will both help to attract new candidates and ensure motivation is kept alive to build a longer term career plan,” Zohira Merah said.
“In this world we need to learn how to take care of ourselves, that’s why I enrolled in this programme,” said one of the participants. “It’s hard to find work in today’s society, particularly for a woman. I’ve been living with HIV for 12 years and this course given me the opportunity take control of my life and be independent. When I’ve finished I’ll be able to pass on what I’ve learnt to other people living with or affected by HIV which is a good feeling,” she added.
On completion, the course offers new opportunities for people living with HIV to access sustainable economic independence thanks to the agreement established between the National Agency for Administration of micro-credits and the El Hayet. Specialized trainers will help interested and successful participants to apply for micro-credits ranging from US$ 400 to US$ 5,500, reimbursable over a period of up to five years.
“This project is a clear example of how the principle of greater involvement of people living with HIV can be achieved,” said Andy Seale, Chief of Civil Society Partnerships at UNAIDS. “Longer term sustainable solutions such as this workshop in Algeria are an essential part of the response to AIDS,” he added.
“As life-saving anti retroviral therapy becomes more widely available we need more focus on ensuring people living with HIV have the opportunity to fulfil their potential as productive members of society and be economically independent. Often this entails reintegration into the workforce but due to the stigma and discrimination still associated with HIV infection this is not always an easy process. The project is an excellent example of how this can be facilitated in a thoughtful way,” said Kate Thomson, Partnership Adviser at UNAIDS.

