

Feature Story
Three Years On: From crisis to prospective recovery
20 February 2025
20 February 2025 20 February 2025Ukraine has been reeling from three years of war since 24 February 2022. One out of two Ukrainians have been affected by the conflict and more than 12 million people need humanitarian assistance and protection while another 6 million have still not been able to return to their homes.
A war-driven economic crisis has severely impacted healthcare funding, putting access to HIV services at risk. With HIV services entirely dependent on external aid and humanitarian support that is becoming increasingly unstable, the uncertainty of the continuity of U.S. funding has further worsened an already dire situation in Ukraine. In January, the new U.S. Administration froze all foreign assistance for a 90-day period. A waiver to allow life-saving services was subsequently issued allowing support for some HIV services.
The U.S. President's Emergency Plan for AIDS Relief (PEPFAR) contributed US$15.6 million to the HIV response in Ukraine during 2023 and 2024. This includes $11 million for antiretroviral therapy and $2 million for various types of rapid test kits, while the rest was used for laboratory expenses.
UNAIDS and partners estimate that 92,840 Ukrainian people could see their HIV treatment disrupted if U.S. funding was to be entirely cut – that is 78% of all people living with HIV on treatment. In addition, stocks of life-saving treatment and HIV prevention drugs are low, with people only getting three versus six months of drug supply.
The threat of a potential financial void left by the U.S. is forcing Ukraine’s health system to search for alternative sources of funding. From Global Fund reprogramming to private sector donations to bulk medicine offers from pharmaceutical companies. Many options are being explored to patch together a lifeline. However, even collectively these efforts may not be enough to fill the PEPFAR gap should the U.S. permanently withdraw its support.
There are hopeful signs of recovery like HIV testing increased 23% last year compared to 2023 but obtaining comprehensive epidemiological and clinical data remains difficult.
This inevitably affects the accuracy of overall assessments due to the ongoing conflict, loss of administrative control in certain regions, missing persons, and mass displacement.
Despite ongoing challenges, Ukraine remains committed to the HIV response, supported by a strong coalition of government, civil society, international organizations, and donors. The UNAIDS Secretariat, Co-sponsors, UN agencies, and member states continue working together to ensure essential services for women, people living with HIV, and key populations, reinforcing the response's sustainability even in the face of adversity.
Related information
Special page
Region/country
Related
 Ukraine: Keeping people in care
Ukraine: Keeping people in care
23 February 2026
 Women, HIV, and war: a triple burden
Women, HIV, and war: a triple burden
12 September 2025
 Displacement and HIV: doubly vulnerable in Ukraine
Displacement and HIV: doubly vulnerable in Ukraine
11 August 2025

Feature Story
The critical impact of the PEPFAR funding freeze for HIV across Latin America and the Caribbean
19 February 2025
19 February 2025 19 February 2025The U.S. decision in January to freeze all funding for U.S. foreign assistance, including for the U.S. President's Emergency Plan for AIDS Relief (PEPFAR), has had a critical impact on several countries in Latin America and the Caribbean, exacerbating existing challenges in the HIV response. More than 20 countries in the region rely on these funds to deliver HIV treatment, prevention, and care services, including community-led services focused on the most discriminated and marginalized communities.
Following the decision to freeze all U.S. funding for foreign assistance, the U.S. Government issued a waiver allowing some funding to support lifesaving services. However, confusion about which services may be supported and a lack of support for some services means the situation remains critical, posing a serious risk of setbacks in the AIDS response in the region. While some key treatment services and prevention of vertical transmission have been gradually coming back into operation, most countries have been facing disruptions in their HIV treatment programs.
The lack of funding has led to a significant decrease in community-led HIV prevention efforts, a reduction in treatment adherence, counseling, and social support and monitoring activities. Consequently, there are increased risks of new HIV infections, of higher mortality rates, and a deterioration in the quality of care for people living with HIV, directly impacting their capacity to access treatment and to achieve viral suppression – crucial steps towards the global target of eliminating AIDS as a public health challenge by 2030.
In Colombia and Peru, the freeze has severely affected migrants and refugees, who are estimated to have an HIV prevalence two times higher than the general population. Approximately 4,000 migrants and refugees are receiving antiretroviral treatment (ART) in Colombia thanks to the government efforts and cooperation funds, but the withdrawal of such resources is directly impacting this vulnerable group and the country's capacity to include them in the health system. One community-led organization supporting HIV services among migrant and LGBT communities had to end contracts for 40 out of 70 team members, significantly reducing their capacity to provide essential services to reach such populations.
In the Dominican Republic, even though the government guarantees access to antiretroviral treatment, the pause in PEPFAR funding has left thousands without access to essential HIV services. PEPFAR supports around a third of HIV care services, including PrEP services, health human resources, and laboratory networks. The reduction in community assistance has made it difficult for people to access their medications, especially those who live far from care. The quality of services offered by the Comprehensive Care Services (known by the acronym SAI in Spanish) in the Dominican Republic has been highly compromised, with many staff and services entirely dependent on PEPFAR funds.
El Salvador has also been impacted, with PEPFAR projects supporting comprehensive HIV care clinics now suspended. This has caused a slowdown in care, and the opportunity for new diagnoses and early initiations of antiretroviral treatment is likely lost.
In Guatemala, the HIV epidemic is mainly concentrated among key populations such as transgender individuals, gay men and other men who have sex with men, and sex workers. The distribution of PrEP for these groups has been severely disrupted, with many organizations that rely on U.S. Government funding suspending their work. The reduction of personnel, including medical staff as well as outreach workers that were funded through PEPFAR has resulted in people being unable to access HIV prevention and treatment services.
Haiti has seen a significant impact on its HIV response, with PEPFAR covering around 60% of the national response. The stop-to-work order has thrown the response into disarray, causing anxiety for the 127,000 Haitians living with HIV who are on treatment. In the context of the humanitarian crisis and gang violence, more than 1 million people are now internally displaced in Haiti, many of them displaced multiple times– among them women, girls and children. Escalating violence has also led to the closure of 39% of health facilities, including two of the capital’s three major hospitals. Access to healthcare has never been more limited. The quality-of-service delivery of medicines has also been affected, with approximately 5,000 health workers receiving directives to stop working.
In Jamaica, 70% of HIV resources come from external sources – with PEPFAR covering around 50% of services. The pause in funding has raised concerns about the delivery of HIV prevention services for at risk populations delivered via civil society organizations. Civil society groups have reported that their institutional stability and survival are at risk, with many unable to guarantee the continuous employment of their field staff in charge of liaising with the most discriminated and affected populations who need HIV services.
In Panama, the suspension of a study on recent HIV diagnoses and the halt in laboratory sample transportation have further limited essential diagnostic and monitoring services. The country had already been facing significant disruptions, particularly among the indigenous Ngäbe-Buglé population, who are expected to face increased obstacles to accessing HIV services. In 2023, despite representing only 5% of Panama's population, the territory, which is home to approximately 225,000 residents, accounted for 30% of the nation's AIDS-related deaths among individuals aged 29 or younger, as reported by the Panama Ministry of Health.
In Brazil, on the other hand, the Unified Health System (SUS) guarantees uninterrupted universal and free access to health services, including HIV diagnosis, treatment and prevention for all people living in Brazil. The “A hora é agora” project, carried out in five capital cities with PEPFAR resources, worked to provide specific services such as doctors, reception and delivery of antiretroviral drugs and PrEP in addition to public health services, so the national response to HIV was not impacted by the cut in resources.
Latin America is one of the three regions in the world where new HIV infections have increased since 2010, with a rise of 9%, which highlights the urgency of addressing these disruptions. The Caribbean region has made significant progress in reducing new HIV infections and increasing access to treatment. Still, the freeze on PEPFAR funds threatens to reverse these gains and the ongoing process of creating sustainability roadmaps to increase national funding for the HIV response.
UNAIDS continues to work with various partners to help mitigate the impact and find the best solutions and calls for the continuity of all essential HIV services in the region.
"United States support through PEPFAR has been a cornerstone of the HIV response in our region, including a key driver for strengthening the sustainability and resilience of national responses. The recent humanitarian waiver reflects the commitment of the American people to save lives and maintain momentum to end AIDS by 2030," says Luisa Cabal, UNAIDS Regional Director for Latin America and the Caribbean. "UNAIDS will continue to convene communities, civil society organizations, governments, and partners to advocate for continued support and critical HIV services supported by PEPFAR. It is also time for the governments of the region to play a leadership role in guaranteeing the right to health of their most marginalized populations."




Feature Story
How the shift in US funding is threatening both the lives of people affected by HIV and the community groups supporting them
18 February 2025
18 February 2025 18 February 2025On 20 January 2025 the United States announced a 90-day freeze on US foreign aid which has had a devastating impact on people living with and affected by HIV, on the people and organizations supporting them and on the global response to HIV as a whole.
Community organizations have been particularly impacted by the freeze in funding. Community healthcare workers are losing their jobs, clinics are having to be shut down and, as a result, people in need of HIV testing or prevention or who are living with HIV and dependent on daily antiretroviral medicine are unable to access the life-saving HIV services they need.
On 10 February, UNAIDS convened an emergency meeting with community organizations to monitor the impact of the unfolding crisis. Community groups reported that HIV services around the world are facing serious challenges. Some are grinding to a halt. Supplies of antiretroviral medication, pre-exposure prophylaxis (PrEP), post-exposure prophylaxis (PEP) and condoms have been disrupted, leaving many without essential tools of HIV treatment and prevention.
HIV testing kits are increasingly scarce and outreach services – essential for connecting people in need of HIV testing – are being suspended. As a result, HIV and sexually transmitted infection testing are disrupted, threatening detection and prevention efforts.
“The damage is immediate and severe,” said one advocate. “People who rely on [U.S.-funded] programmes for [safety and] survival are suddenly left with nothing.”
The US pause in administering foreign assistance while it reviews recipients is not just a bureaucratic delay; it is a direct threat to continued progress against AIDS and will quickly erode decades of hard-won gains in the global HIV response. It will destroy many community organizations without which the world cannot close the gaps in HIV testing, prevention and treatment.
The US Government has invested more than US$ 100 billion to date in the global fight against AIDS with the US accounting for around 73% of donor funding for HIV worldwide; millions of people at risk for and living with HIV rely on US funded clinics to stay healthy in the face of HIV.
Community-led data reveals community organizations are bearing the brunt of the pause
A survey conducted by the Uganda Key Populations Consortium found that 97% of respondents reported negative effects on their HIV service due to the freeze on US foreign assistance. A staggering 43% of organizations supporting key populations surveyed said they relied on US funding for at least 76% of their budgets.
Another joint survey by Aidsfonds, the Global Network of People Living with HIV (GNP+), and the Robert Carr Fund found similarly worrying results. Of 564 organizations surveyed across 25 countries, 95% reported direct impacts from the US funding freeze. 43% of programmes have paused implementation, while 35% have fully suspended operations.
“The results are alarming,” said Mark Vermeulen, Director of Aidsfonds. “More than half (57%) of the organizations estimate that this crisis will impact more than a million people. The longer these disruptions persist, the greater the risk of a new generation of preventable HIV infections. This threatens to undo the hard-earned progress in reducing new infections among children.” (New HIV infections among children had been reduced by 62% from 2010 to 2023, largely thanks to investment and commitment from the US Government).
It’s not just people living with or at risk for HIV that face an existential threat
The financial void left by the US aid freeze of its foreign assistance is forcing community groups to fire employees and/or to close up shop entirely. Many community organizations do not have sufficient funding reserves to stay afloat through the 90-day (or perhaps longer) period of no US funding.
“The leadership of national networks of people living with HIV have been forced to let go of community cadre staff- peer educators, adherence counselors, community health facilitators, and mentor mothers,” said Florence Anam, Co-executive Director of GNP+.
GNP+ recently convened with leaders from national and regional networks of people living with HIV and released a statement with the main concerns.
“These organizations are not a luxury – they are critical for ending AIDS,” said Christine Stegling, Deputy Executive Director, UNAIDS. “Serving as advocates, peer educators, care providers and watchdogs, community-led organizations ensure that lifesaving HIV testing, prevention and treatment reaches those most in need.”
Many organizations have spent years garnering the trust of the communities they serve. If these organizations disappear, even if others replace them one day, it will take years to reestablish the bonds of trust that allow them to be so instrumental in encouraging people to seek HIV care.
In a joint survey by Aidsfonds, GNP+ and the Robert Carr Fund 22% of organizations reported increased experiences of discrimination, including reports of discrimination within healthcare settings, where people faced barriers to accessing care.
LGBTQ+ communities in need of HIV testing, prevention and treatment fear increased risks of violence and discrimination as funding for protective services – led by HIV community groups – disappear.
Since the earliest days of the AIDS pandemic, communities and community-led services have been instrumental in ensuring equitable, accessible HIV testing, prevention and treatment – as well as the supportive services that make all three possible.
Communities have been at the forefront, driving the delivery of comprehensive care, life-saving treatment and offering regular monitoring and prevention services and psychosocial support. Their unwavering dedication has not only saved millions of lives but also reshaped the trajectory of the AIDS pandemic. Their leadership and work on HIV are a model for all other responses to communicable diseases.
By paralyzing frontline response efforts led by community groups, the US decision to freeze funding is weakening health systems across the Global South. The freeze not only jeopardizes precious gains made to date against HIV – it also threatens to usher in a new wave of entirely preventable HIV infections and AIDS-related deaths.
The community groups stressed that this crisis extends beyond HIV treatment. The funding cuts impact efforts to provide clean water, basic education and to prevent human trafficking of girls. The loss of funding is dismantling the fragile safety net that has been built over decades around the world
“We are deeply concerned about the sustainability of the HIV response, particularly support for key populations, HIV prevention, human rights and community led responses. We are re-orienting our own efforts to support the communities and organizations that are both bearing the brunt of the loss of funding and facing targeted attacks on their rights and their very lives,” said John Plastow, Executive Director of Frontline AIDS, a global partnership, headquartered in the UK and South Africa, that works with 60 partners across 100 countries around the world. Over 20 of their partners have said they are affected by the US foreign aid freeze.
Since the US funding freeze on foreign assistance was announced, UNAIDS has conducted daily assessments led by its regional and country teams to track disruptions and to relay urgent needs to donors and to governments of affected countries. At country and regional levels, UNAIDS has also been convening people living with HIV and other affected communities to assess the impact and discuss mitigation measures. For the latest updates: Impact of recent U.S. shifts on the global HIV response - The global impact of PEPFAR to date | UNAIDS
UNAIDS stands in solidarity with community leaders calling on the US, other donors and governments of affected countries to step in before irreversible damage is done. UNAIDS and communities call on the US to maintain its global leadership on, and unparalleled support for the global response to AIDS. Without immediate intervention, decades of progress in the global HIV response will be undone, leaving the world on the precipice of a public health disaster that we have the power and tools to avert.



Feature Story
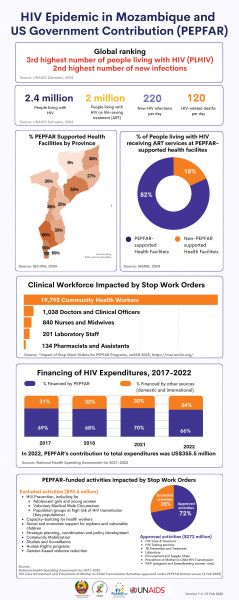
HIV Epidemic in Mozambique and US Government Contribution (PEPFAR)
18 February 2025
18 February 2025 18 February 2025

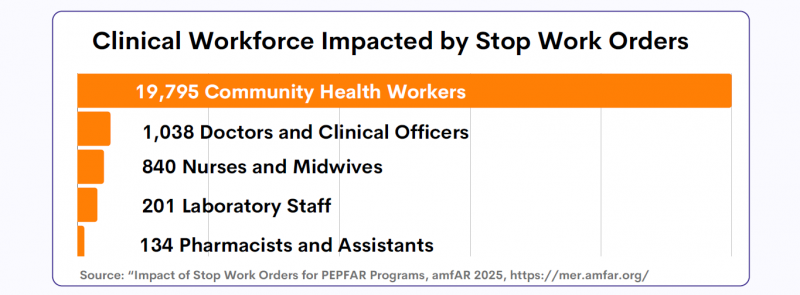
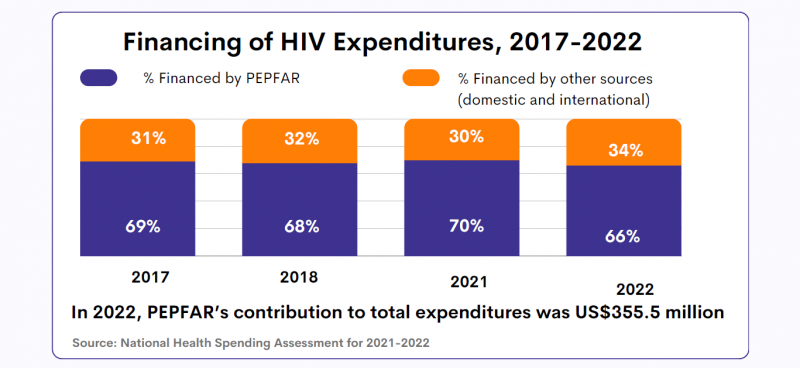


HIV epidemic in Mozambique and US Government contribution (PEPFAR)
Region/country




Feature Story
A crisis unfolding: hard-won progress in Ethiopia’s HIV response at risk
13 February 2025
13 February 2025 13 February 2025Ethiopia has made significant progress in its HIV response in recent years and is on track to reach the UNAIDS 95-95-95 targets with 90% of people living with HIV in the country being aware of their HIV status; 94% of those diagnosed with HIV receiving antiretroviral (ARV) therapy; and 96% of people on ARV therapy achieving viral suppression.
But now, that progress is at risk. The recent pause in United States foreign assistance poses a direct threat to the lives and well-being of thousands of people living with HIV in Ethiopia and millions globally. Critical services are grinding to a halt, leaving people who rely on them facing an uncertain and dangerous future.
Ethiopia is heavily reliant on external funding for its AIDS response. PEPFAR provides 53% of HIV funding in the country. In 2023, UNAIDS’ estimates show that there were 610 000 people living with HIV in Ethiopia, 510 000 of whom were accessing antiretroviral treatment.
For women living with HIV, uncertainty is growing. Limited and unclear communication from healthcare providers and policymakers has left them in the dark about treatment changes, medication availability, and service disruptions. With no clear answers, they are forced to rely on rumors, fueling fear and anxiety.
“We don’t know what’s happening. Are services being cut permanently? Will we still get our medication next month? No one is telling us anything,” one woman shared.
To make matters worse, case workers and counsellors—once a vital source of medical and emotional support—are disappearing. These professionals were more than healthcare providers; they were trusted confidants who ensured women received care in a stigma-free environment. Their absence is leaving many feeling abandoned.
“They understood our struggles, checked in on us, and made sure we had what we needed,” another woman explained. “Without them, we feel forgotten.”
As services become increasingly unreliable, distress and fear are taking hold.
Shortages and desperate measures
Funding cuts bring shortages, and for women living with HIV, the fear of running out of medication is overwhelming. Access to antiretroviral therapy (ART) is essential—it keeps people alive. Yet many are already facing supply disruptions, and whispers of medication shortages are spreading panic.
“If I can’t get my medicine, what happens to me?” one woman asked. Women living with HIV who have been healthy for years now fear an uncertain future where their treatment is no longer guaranteed. People living with HIV who do not access antiretroviral therapy will eventually develop AIDS and die. To cope, many have resorted to stockpiling medication, traveling long distances and spending entire days at clinics in hopes of securing extra supplies. While understandable, this survival strategy comes at a heavy cost—disrupting work, family life, and daily routines. No one should have to live in fear of their next refill. The urgent need for stable, uninterrupted HIV treatment cannot be overstated.
Adding to the crisis, shortages extend beyond medication. The dwindling supply of test kits, including viral load tests, is threatening the future of diagnosis and monitoring. These tests are crucial to ensure that people living with HIV maintain undetectable viral levels, reducing transmission risks and protecting their health.
Fears have also been expressed around the availability of medications for HIV prevention, particularly for the prevention of vertical transmission of HIV. If the current pause in the supply of medical resources continues, the availability of these vital medications could be severely compromised, putting the lives of women and children at even greater risk. For women living with HIV who are pregnant, a lack of lifesaving medications for themselves also means their children can be born with HIV even though this is entirely preventable.
Without test kits and prevention measures, undiagnosed and untreated cases could rise dangerously. “We can’t afford to go backward,” one woman said.
A Plea for Action
The voices of these women reveal a stark and urgent reality—funding cuts have left people living with HIV in a state of uncertainty, with no clear path forward.
"Urgent intervention is needed,” stressed Tina Boonto, Country Director for UNAIDS Ethiopia. “UNAIDS is gathering information and developing funding solutions to address the shortfall, with proposals for both the government and external partners to ensure continuity of critical services. We hope Ethiopia's government will step up and lead in covering these essential services. We must act now to safeguard gains that have been made and succeed in securing sustainable support to people living with HIV."
While the future remains uncertain, one thing is clear: without swift action, the hard-won progress in Ethiopia’s HIV response is at risk.
Impact of recent U.S. shifts on the global HIV response
Region/country

Feature Story
Government ensures continuity of treatment in Malawi
10 February 2025
10 February 2025 10 February 2025There is minimal disruption to HIV services in Malawi. People living with HIV are receiving services. People living with HIV who go to facilities that have been are closed are being referred to government services that are open. Early last week, in response to UNAIDS’ advocacy, the government issued a press release assuring the public that HIV services will continue uninterrupted. Also last week the government developed a contingency plan, which will form Part B of the ongoing work to develop a Sustainability Plan for Malawi. The government issued a circular of the activities it will prioritize going forward. It has redeployed its staff to fill the positions that are vacant because of the stop order. In general services are ongoing.
Unfortunately, PrEP and long-acting injectables are not part of the package the government will prioritize. Civil Society groups are concerned about the omission of prevention interventions beyond treatment and PrEP for pregnant and breastfeed women. UNAIDS is working with other international partners to see if they would be willing to support PrEP and long-acting injectables.
Staff partner reduction
Non-government organisations such as Partners in Hope, Partners in Health, Baylor College, Lighthouse Trust, Pakachere, CEDEP, EGPFAP, Right to Care, JPPHEIGO, MACRO employ more than 4000 cadre of staff in support of the AIDS response using PEPFAR and CDC resources. These cadre include 180 Doctors, 1640 Health Diagnostic Assistants, and 1870 treatment supporters received stop orders and ceased their activities. Some of these NGOs did not receive the Stop Orders but stopped activities as a precaution. They surrendered the work equipment, including computers and vehicles at the district health offices. Civil society organizations including the Malawi AIDS Services Organisation and the Malawi network of people living with HIV work has been impacted. They have stopped or slowed their community-led monitoring work.
Interruptions to Services at Key Populations Drop-In Centres
The drop-in centers for key population are not staffed because most of the staff are PEPFAR or CDC supported, who are not working. The drop-in centres are open but minimally staffed. PLHIV are worried about what will happen when the stocks in country – approximately 9-months-worth – run out. Members of civil society are keen to understand how the government will move Malawi’s response to HIV forward, sustainably. They are also concerned about the continuity of prevention and treatment efforts going on in Global Fund Grant Cycle 7 given that the US government provides the bulk of contributions to the GFATM.
The UN Family Responds Together
The UNCT met to discuss the situation. Beyond HIV, the impact of the Stop Order was widespread including on support for the forthcoming elections, maternal and child health and resettlement of refugees. The UNCT agreed on a series of support and advocacy efforts to move forward including reaching out to the government to find out where they need our support and what austerity measures they will take given the freeze on funding.
Last week, the U.S. Ambassador assured the UNAIDS Country Office that PEPFAR-supported services will recommence early next week. She indicated the country needs to complete the sign the Sustainability Plan.
The UCO met the Minister of Health and reached out to other Senior Government Officials and the Sustainability plan has now been cleared by the Minister of Health. The UCO understands the Sustainability plan and the Contingency Plan are one of the key items that the Minister will share with the President this Friday.
The UCO will continue to meet with the Minister of Health and Ambassadors from other countries, the NAC, and civil society to understand the flow of services in the districts and see how best we can support.
Region/country
Related
Feature Story
Government mitigation measures in Cameroon
09 February 2025
09 February 2025 09 February 2025The Ministry of Health in Cameroon has developed a set of mitigation measures to ensure continuity of HIV services to people living with HIV and vulnerable populations that could be impacted by the suspension of Unites States Government funding. The mitigation measures describe immediate, medium and long-term actions that also represent an accelerated move towards sustainability.
The minister has issued a circular to all regional delegates and directors of hospitals to take appropriate measures within their authority to ensure continuation of HIV, TB and Malaria services with priority given to the most vulnerable, these include reallocation of health personnel and readjusting of workload to fill the gaps of the 2332 personnel that were under PEPFAR funding. The objective is to ensure that there would be no interruption of services to anyone. Talks are ongoing with the Global Fund country team and other partners to find possibilities of reallocation of resources.
Region/country
Related
Feature Story
Impacts of U.S. pause of foreign assistance on global AIDS programmes in Kenya
09 February 2025
09 February 2025 09 February 2025Overall National Response
A Cabinet memo on the current situation and recommendations for the government of Kenya (GOK) to mitigate the situation has been developed by Ministry of Health and domestic resource allocation is a key recommendation as well as fast-tracking the development of the ongoing HIV sustainability roadmap.
A special national HIV inter coordination committee (ICC) that includes CSOs, communities, private sector, UN Agencies and government stakeholders was convened by UNSDCC on Friday, January 31st to assess the impact and suggest solutions.
Commodity Security
UNAIDS’ Country Office (UCO) has been part of the commodity security meetings.
All requests to distribute PEPFAR-supported products in country through USAID are on hold until further guidance is provided to unfreeze the initial communication.
Products that were to be distributed in January 2025 under USAID/PEPFAR include ARVs (Nevirapine syrup, Dolutegravir 10 mg and 50 mg). For these products, health facilities had a stock balance between 2 to 4 months by 31st December 2025.
The country may start experiencing erratic supply of Nevirapine syrup and Dolutegravir (DTG) 50 mg towards the end of March and May 2025, respectively, if the stop work order is not lifted.
The current stocks at Kenya Medical Supplies Authority (KEMSA) for DTG 10 mg will sustain the country beyond June 2025.
Viral load and EID products are mainly procured through PEPFAR support. This will be adversely affected if the stop order is not lifted as soon as possible as the quantity under the Global Fund is minimal, targeting specific point of care testing sites.
Stop Gap Measures for Commodity Security
GOK will be required to allocate funds for the distribution of these products from Missions for Essential Drugs and Supplies (MEDS) to health facilities. The estimated cost by KEMSA is approximately USD 10 million.
Procurement and delivery of health products will be facilitated by the Global Fund and government counterpart financing. Additionally, discussion to front load commodities under Global Fund year two will be initiated.
If the stop order continues, GOK will be required to allocate funds to cover the deficit.
Discussions to allow Government to distribute HIV commodities under MEDS is to be initiated if the stop work order is not lifted. (To note, as of February 2, 2025, there has been a reprieve with the new circular on waiver for administration costs for procurement and supplies of essential drugs. The circular is however yet to be implemented as it is a new directive)
Human Resources for Health
All PEPFAR-supported medical personnel/health workers have been requested to stop work as per the stop work order effected in PEPFAR supported counties and facilities.
All PEPFAR-supported implementing partners (CSOs, FBOs, UN) and sub-grantees have been requested to stop work and consequently, staff have been requested to proceed on leave for the duration of the stop work order (90 days).
In some of the counties, the county government has recalled all health workers who are on leave to cushion the situation.
UCO programs supported by PEPFAR through COAG (Community led monitoring and Strategic Information) have been halted.
Consequently, the five UCO CLM partners (CSOs, KP led organizations) have stopped work and over 148 staff IP staff have been affected, and service delivery constrained.
Way Forward
UCO to consider supporting a national communities’ meeting to discuss the impact on service delivery and make recommendations to national and county governments.
As mentioned above, as of February 2, 2025, there was a reprieve with the new circular on waiver for administration costs for procurement and supplies of essential drugs, including continued support for human resources. Hopefully, measures will be implemented this coming week to avert potential risks.
Region/country
Related
Feature Story
Impacts of U.S. pause of foreign assistance on global AIDS programmes in Botswana
09 February 2025
09 February 2025 09 February 2025Funding for the HIV Response in Botswana
Prior to the U.S pause of foreign assistance, the Government of Botswana funded two thirds of its HIV response (approximately US$ 90 - 95 M). The remaining costs were covered by the U.S. Government (US$ 55 M via the U.S. President’s Emergency Plan for AIDS Relief, PEPFAR, and US$ 12M via the Global Fund to Fight AIDS, Tuberculosis and Malaria).
Immediate Risks
The pause and stop order will:
- Undermine Botswana’s ability to fully achieve UNAIDS’ 95-95-95 targets and the efforts to finding the missing 5-2-2 in Botswana. That means reaching an additional five percent of all people living with HIV with testing so they are aware of their HIV status; ensuring that an additional two percent of all people who are living with HIV and are aware on treatment and ensuring an additional two percent of all those aware of their status and on treatment have their viral load suppressed.
- Take away safe spaces for key populations (KPs) and adolescent girls and young women (AGYW) and increase their vulnerability to HIV-related sigma and discrimination, gender-based violence, mental health problems and other related social ills.
- Reduce access to early diagnosis and treatment for HIV which leads to health complications and higher default rates for treatment adherence which correlates to a lack of viral suppression.
Impact on Civil Societies and Communities
In Botswana, the impact of the pause on U.S. foreign assistance and related stop order has already affected delivery of HIV prevention and treatment services by civil society organisations (CSOs) and will have implications for the entire system across the national HIV response.
UNAIDS consulted with a significant number of CSOs to establish the impact of the pause and stop order on the provision of services. Additionally, a task force set up by NAHPA and the Ministry of Health and cochaired by UNAIDS met to establish a complete picture of disruptions not just for CSOs but also within MOH and NAHPA where a total of about 207 positions are funded by PEPFAR.
Most of the affected CSOs are those providing some services for key and vulnerable populations (AGYW, MSM, SW, PLWHIV). The government continues to provide services and encourages the affected CSOs to refer and link clients to government facilities. While CSOs have been funded to provide demand creation activities, only three of those consulted have clinics or drop-in centres that were considered safe by the aforementioned population groups. They offer HIV counselling and testing Services, ART dispensing, PrEP dispensing, adherence and psychosocial support, condom distribution and referral and linkages to other services. The stop order has led to the closure of these CSO clinics and drop-in centres and disrupted service delivery.
Government Response
Botswana’s government health facilities continue to operate and provide services. The Ministry of Health issued a press release on 29 January assuring Batswana living with HIV that the pause of U.S. assistance will not affect the availability of ARVs as they are directly procured by the Government of Botswana. This was followed by another press release on 6 February further assuring continuity of services.
Mitigation Measures
Through the Joint Oversight Committee, a task team will be established to monitor developments and ensure that HIV services are not disrupted, clients are referred and linked to care at government facilities and that CSO’s providing services will receive domestic funding.
Consultative meetings between stakeholders are ongoing as per the Ministry of Health’s press release.
Region/country
Related
Feature Story
Impact of the pause of U.S. foreign assistance in Ethiopia
06 February 2025
06 February 2025 06 February 2025The pause of U.S. foreign assistance on Ethiopia will affect many areas of development, however its impact on Ethiopia’s national HIV response is particularly severe.
Ethiopia is on track to reach the global 95-95-95 targets: with 90% of people in Ethiopia living with HIV being aware of their HIV status; 94% of those diagnosed with HIV receiving antiretroviral (ARV) therapy; and 96% of people on ARV therapy achieving viral suppression. ARV treatment is currently provided to 503,000 people via 1,400 health facilities across the country. However, with ongoing challenges to the country health system and socio-economic development, Ethiopia remains reliant on external donors for its HIV response.
SERVICE DISRUPTION: Pause of U.S. assistance to community programs and drop in centres serving women, young girls and priority populations at higher risk of HIV infection means tens of thousands of individuals will no longer be able to access critical services such as HIV testing, antiretroviral treatment, pre-exposure prophylaxis (PrEP) for HIV prevention, and screenings for tuberculosis, sexually transmitted infections and support to address gender-based violence. The closure of many drop -in centres and the termination of outreach workers’ and peer educators’ contracts will effectively shut off support to vulnerable groups.
Table: Breakdown of Service Disruption in three regions in Ethiopia: Addis Ababa; Oromia and Gambella
| Number of people | Type of service |
| 2,385 | People will not be able to continue to access ARV treatment; TB treatment; STI treatment |
| 18,075 | People will no longer receive support for health and care services (differentiated service that facilitates easier access to health care providers) |
| 14,811 | People will not be encouraged and supported to access HIV testing (key to the success of HIV programmes is people knowing their status and starting treatment early) |
| 879 | People will stop accessing pre-exposure prophylaxis to prevention new HIV infections (PrEP) |
| 100 | People will stop the pilot programme for the new simplified, twice annual injectable PrEP |
| 235,560 | People will no longer receive condoms to prevent new HIV infections and sexually transmitted infections. |
SUPPLY CHAIN DISRUPTIONS: The funding freeze has caused critical delays in the supply of essential HIV services, including testing kits and other resources. Notably, PEPFAR is responsible for 100% of the procurement of viral load and Early Infant Diagnosis (EID) reagents. The interruption in funding is limiting the availability of these crucial supplies, undermining the program’s ability to conduct timely viral load and EID testing, which are essential for effective patient monitoring and treatment.
REDUCED CAPACITY FOR HEALTHCARE SUPPORT: The pause threatens to stall efforts to build local healthcare capacity. It impacts the training and support of health workers, slowing progress in Ethiopia’s fight against HIV. This reduction in capacity limits the ability of healthcare professionals to respond effectively to the growing HIV epidemic. The disruption of ICAP’s capacity building, M&E, and clinical mentoring threatens care for advanced HIV patients, putting Ethiopia’s progress at risk. The freeze is also likely to scale back key prevention programs, including outreach, education, and services for key populations, worsening the epidemic
HEALTH INFORMATION SYSTEM DISRUPTION: Ethiopia's Health Information System is severely affected by the stop work order. The termination of 10,000 data clerks, who are essential for entering ART data into the health information management system, is compromising data management, particularly in tracking lost-to-follow-up cases. This disrupts key national activities, such as HIV estimations and studies of key populations. Furthermore, the cessation of the HIV surveys and surveillances, and HIV Estimation Technical Working Group (TWG) which includes CDC, USAID, and PEPFAR undermines the accuracy of HIV data and threatens the continuity of critical HIV data management systems.
HUMAN RESOURCES IMPACT: Ministry of Health shared that 5,000 public health workers’ contracts funded by U.S. assistance from all regions in Ethiopia have been terminated. These health workers are supporting Ethiopia’s HIV response – improving regional capacity to accelerate progress towards Ending AIDS. While the government of Ethiopia will take over the gap, the sudden loss of programmatic experience and the transition period will be rough.
ACTIONS TO ADDRESS THE SITUATION: On 4 February 2025, The Ministry of Health of Ethiopia issued a circular to all regional health bureau to assure regional health offices that the government will step in to manage the work that was performed by the US-funded personnel in order to ensure programme continuity.
UNAIDS Ethiopia together with WHO will be convening a situation assessment briefing on 11 February 2025 with government, CSOs and development partners to identify solutions to address gaps in the HIV, TB, Malaria and health andcCommunity systems responses in Ethiopia.
