
Feature Story
Judicial officials convene in Dakar for consultation on HIV, the law and human rights
08 February 2011
08 February 2011 08 February 2011
On 7 February, UNAIDS Executive Director Michel Sidibé spoke at the opening ceremony of a high-level consultation on HIV, the law and human rights in Dakar, Senegal.
Ministers of Justice and judges from across West and Central Africa gathered on 6-8 February in Dakar, Senegal, for a high-level consultation on HIV, the law and human rights. The meeting aimed to increase the engagement of judicial officials in the HIV response at national levels.
Eighty percent of countries in West and Central Africa have laws that criminalize HIV transmission, same-sex relations or sex work. Across the region, people living with HIV experience widespread stigma and discrimination in access to employment, education, health and social services. In many countries, people living with HIV and key populations at higher risk of HIV exposure—including sex workers and men who have sex with men—have limited access to legal support when injustices are committed.
“Laws should work for the AIDS response, not against it—they should never obstruct the health or survival of any individual,” said UNAIDS Executive Director Michel Sidibé, in his opening remarks at the consultation. “We must truly address discrimination and injustice related to AIDS,” he added. Mr Sidibé urged justice ministers to base their laws on science and ensure that all people have equal access to HIV prevention, treatment, care and support.
“We can no longer ignore the law as a means of combating HIV,” said Senegal’s Minister of Justice, Cheikh Tidiane Sy, noting that the epidemic had generated complex legal and human rights issues in the jurisprudence of countries across the region. Mr Sy underscored that judicial officials should not be limited to rendering decisions in a court of law. “It is equally important that magistrates involve themselves in activities that will increase legal knowledge among populations and ensure that they have access to justice,” he said.
The consultation—organized by the Joint United Nations Programme on HIV/AIDS (UNAIDS), the United Nations Development Programme (UNDP), the African Association of Highest Francophone Jurisdictions (AA-HJF) and the Office of the High Commissioner for Human Rights (OHCHR)—offered an opportunity for discussion on a range of HIV-related judgements, legal instruments and country-level initiatives. The meeting also provided a forum for individuals directly impacted by HIV-related laws, including people living with HIV, to share their experiences and perspectives.
Laws should work for the AIDS response, not against it—they should never obstruct the health or survival of any individual
UNAIDS Executive Director Michel Sidibé
Speaking to meeting participants on Sunday, Jeanne Gapiya Niyonzima, an HIV-positive woman and President of the Burundian Association of People Living with HIV, recalled how her doctor immediately ordered the termination of her pregnancy and removal of her uterus after she tested positive for HIV. “As magistrates, you can appreciate the gravity of this kind of assault on the physical and social integrity of a human being,” said Ms Niyonzima. “If we fail to provide a conducive social and legal environment, we risk losing all gains in the HIV response,” she added.
Judicial officials can play a critical role in protecting human rights and pushing forward the HIV response. In Burkina Faso, for example, where an estimated 1.2% of the adult population is living with HIV, the UNDP-led Programme d’appui au monde associatif et communautaire (PAMAC) is collaborating with other non-profit organizations and David Kaboré—a judge and human rights defender—on a legal literacy project to promote and safeguard the rights of people living with HIV. Launched in 2003, the project offers free and confidential legal advice to people living with HIV and has been instrumental in highlighting and addressing cases of HIV-related discrimination in the country.
Many countries around the world continue to have laws or policies that undermine HIV responses and punish, rather than protect, people in need. Seventy-nine countries criminalize same-sex relations between consenting adults. More than 100 countries, territories and areas criminalize some aspect of sex work. And 48 countries, territories or entities impose some form of restriction on the entry, stay or residence of HIV-positive people based on their HIV status.
UNAIDS advocates for protective laws and measures to ensure that all people in need benefit from HIV programmes and have access to justice, regardless of health status, gender, sexual orientation, drug use or sex work.
Last year, UNAIDS and UNDP launched the Global Commission on HIV and the Law, bringing together public leaders from many walks of life and regions, as well as experts in law, human rights and HIV. The UNDP-led Commission is working to ensure that laws support effective AIDS responses.



Feature Story
Thirty years into the AIDS epidemic, leaders will gather in June for 2011 UN General Assembly High Level Meeting on AIDS
04 February 2011
04 February 2011 04 February 2011
Thirty years into the AIDS epidemic, and 10 years since the landmark UN General Assembly Special Session on HIV/AIDS, the world will come together to review progress and chart the future course of the global AIDS response at the 2011 UN General Assembly High Level Meeting on AIDS from 8 –10 June 2011 in New York.
Member States are expected to adopt a new Declaration that will reaffirm current commitments and commit to actions to guide and sustain the global AIDS response.
The meeting will be convened by the President of the 65th Session of the United Nations General Assembly H.E. Joseph Deiss, who has urged countries to participate in the event. “I call on all nations to unite at the High Level Meeting on AIDS. Together we can chart the future of the AIDS response,” wrote Mr Deiss.
I call on all nations to unite at the High Level Meeting on AIDS. Together we can chart the future of the AIDS response
President of the 65th Session of the United Nations General Assembly H.E. Joseph Deiss
UNAIDS data shows that steady progress is being made towards the vision of zero new infections, zero discrimination and zero AIDS-related deaths through universal access to HIV prevention, treatment, care and support. However, stigma and discrimination continue to be obstacles and services do not reach everyone in need. There are still 10 million people waiting for HIV treatment and for every person starting treatment, two others become infected.
The Secretary-General of the United Nations Ban Ki-moon has highlighted the need for global solidarity and partnership at this time. “The 2011 High-Level Meeting on AIDS comes at a pivotal moment in the history of the epidemic. Thirty years into the AIDS response, let us unite for universal access. Let us, once and for all, set the course for zero new HIV infections, zero discrimination, and zero AIDS-related deaths,” wrote Mr Ban.
Thirty years into the AIDS response, let us unite for universal access. Let us, once and for all, set the course for zero new HIV infections, zero discrimination, and zero AIDS-related deaths
Secretary-General of the United Nations Ban Ki-moon
The event will take place in a global context of fiscal austerity. Both donor and recipient countries face new opportunities and challenges through such issues as innovative financing, technology transfer and the integration of AIDS and health and other services.
Remembering the 33.3 million people living with HIV, UNAIDS Executive Director Michel Sidibé reminds us: “The decisions made at this High Level Meeting on AIDS will change lives today and for future generations.”
Get more information on the civil society application process to participate in the 2011 United Nations General Assembly High Level Meeting on AIDS and Civil Society Hearing.
More information on the 2011 High-level meeting on AIDS
Related


Feature Story
Preventing new HIV infections among children is the focus of a meeting of African First Ladies
01 February 2011
01 February 2011 01 February 2011
(from left) 11-year-old Oluebuechukwu Sylvia Taylor and her mother Uchechukwu Florence
Preventing mother-to-child transmission of HIV (PMTCT) was high on the agenda at a General Assembly of the Organization of African First Ladies Against HIV/AIDS (OAFLA), held 31 January in Addis Ababa, Ethiopia.
“For every dollar spent preventing HIV among children, we save thousands more in treatment avoided,” said UNAIDS Executive Director Michel Sidibé, addressing the gathering of African First Ladies, as well as representatives from civil society and the United Nations. “We are making so much progress for mothers and children, but gains are fragile.”
In recent years, African countries—together with national and international partners—have made great strides in reducing the rate of new HIV infections among children. In 2009, an estimated 54% of pregnant women living with HIV in sub-Saharan Africa received antiretroviral medicines to prevent HIV transmission from mother to child, up from 15% in 2005. Several countries are leading the way, including Botswana, Namibia, South Africa and Swaziland, where coverage of antiretroviral drugs for PMTCT is now higher than 80%.
Empowering women is not an abstract term. It means ensuring that African women have adequate food and shelter, are free from disease, deliver their babies safely and stand alongside men equally and confidently
H.E. Woizero Azeb Mesfin, First Lady of Ethiopia and Chair of OAFLA
In the 10 countries of southern Africa*, the number of children under 15 who became newly infected with HIV fell from 190 000 in 2004 to 130 000 in 2009—a 32% reduction. AIDS-related deaths among children in southern Africa have declined by 26%, from an estimated 120 000 in 2004 to 90 000 in 2009.
Despite progress, some 2.3 million children in sub-Saharan African are living with HIV. In many countries across the continent, stigma and discrimination prevent HIV-positive pregnant women from accessing the services they need.

UNAIDS Executive Director Michel Sidibé addressed the General Assembly of the Organization of African First Ladies Against HIV/AIDS (OAFLA), 31 January 2011, Addis Ababa, Ethiopia.
“I am pleading with you all to join hands and save our future,” said 11-year-old Oluebuechukwu Sylvia Taylor, the daughter of an HIV-positive woman who spoke at the OAFLA meeting. “No child should have to die because of HIV. Let’s work together to ensure zero mother-to-child transmission of HIV in Africa.” Ms Taylor was born HIV-negative as a result of her mother taking antiretroviral drugs during the pregnancy.
In nearly all countries in sub-Saharan Africa, a majority of people living with HIV are women, especially girls and women aged 15-24. The most recent prevalence data show that 13 women in sub-Saharan Africa become infected with HIV for every 10 men. Addressing gender inequalities and empowering women and girls are seen as critical to effective HIV responses in the region.
We are seeing success in the fight against HIV/AIDS. As partners of Africa, our challenge is to maintain and increase this momentum
United Nations Secretary-General Ban Ki-moon
“Empowering women is not an abstract term,” said H.E. Woizero Azeb Mesfin, First Lady of Ethiopia and Chair of OAFLA. “It means ensuring that African women have adequate food and shelter, are free from disease, deliver their babies safely and stand alongside men equally and confidently.” With funding from UNAIDS, the First Ladies recently launched a campaign aimed at increasing PMTCT services and eliminating mother-to-child transmission of HIV.
African Union Summit
The meeting of First Ladies was held alongside the 16th African Union Summit, a gathering of 24 Heads of State from across the African continent and a host of other leaders and dignitaries, including United Nations Secretary-General Ban Ki-moon.
“We are seeing success in the fight against HIV/AIDS,” said Mr Ban, in his remarks at the opening ceremony of the Summit. “As partners of Africa, our challenge is to maintain and increase this momentum,” he added.
The HIV response is one successful example of “humanity acting in solidarity,” said Bingu wa Mutharika, the President of Malawi and outgoing Chair of the African Union, in discussions with the UNAIDS Executive Director. “We must continue our efforts to deploy antiretroviral treatment to those affected, and we should not be complacent about fighting stigma,” he said.
* Angola, Botswana, Lesotho, Malawi, Mozambique, Namibia, South Africa, Swaziland, Zambia and Zimbabwe.
Related



Feature Story
UN Secretary-General reaffirms commitment to be an activist alongside UNAIDS during visit to headquarters
27 January 2011
27 January 2011 27 January 2011
UNAIDS Executive Director Michel Sidibé (left) welcomes United Nations Secretary-General Ban Ki-moon to UNAIDS Secretariat headquarters in Geneva on 26 January. Credit: UNAIDS/D. Bregnard
United Nations Secretary-General Ban Ki-moon paid a visit to the UNAIDS Secretariat headquarters in Geneva on 26 January.
He was welcomed by Michel Sidibé, UNAIDS Executive Director and senior staff, as well as by Kate Thompson a UNAIDS staff member representing UN Plus and Jason Sigurdson from the UNAIDS Staff Association. Christopher Davis, Campaigns Director of The Body Shop was also present and thirteen year old Vilasini Mahesh greeted Mrs Ban with flowers.
In his welcome address to the Secretary-General, Michel Sidibe noted that Mr Ban was a “passionate supporter” of UN Cares and UN Plus and expressed his pride to work with such a leader. He described how UNAIDS follows Mr Ban’s call for organizations to be built around accountability, transparency and efficiency.
The Secretary-General, visiting UNAIDS for the second time, took the opportunity to share his thoughts and vision with staff, and encouraged them to work even harder to “remove the hidden obstacles” in the AIDS response. Regional Support Teams based in Johannesburg, Dakar, Port of Spain, and Panama City joined by videoconference.
As Secretary–General I have a responsibility to take care of all people suffering and experiencing discrimination
United Nations Secretary-General Ban Ki-moon
Mr Ban highlighted the importance of doing more to prevent HIV infections and pledged to be an activist in this issue. He also drew attention to the need for countries to remove travel restriction laws that discriminate against people living with HIV saying, "I am continuing to raise this issue whenever I meet leaders of countries with these restrictions. This is a very important part of human rights." Endorsing UNAIDS vision, he said he would be an activist and a champion for “no new infections, no discrimination and no AIDS-related deaths.”
Mr Ban has shown special interest in issue of UN staff living with HIV and he thanked representatives from UN Plus broadening his vision on the issue of HIV and the workplace. He restated his personal commitment to the importance of the UN in providing an enabling environment for staff living with HIV and removing discrimination based on sexual orientation.
He also took the opportunity to interact with the UNAIDS staff and answer some of their questions. On being asked what motivates him to champion for rights of sex workers, drug users, men who have sex with men and transgender people, Mr Ban said, "As Secretary–General I have a responsibility to take care of all people suffering and experiencing discrimination."
Earlier in the day, Mr Ban co-launched an accountability commission for the Global Strategy for Women’s and Children’s Health which was launched at the MDG Summit in New York in 2010. The strategy, developed with support and facilitation by The Partnership for Maternal, Newborn & Child Health, calls for all partners to unite and take real action towards recognizing that the health of women and children is key to progress on all development goals. He urged UNAIDS staff and UN country teams to take a strong role in integrating HIV response with this initiative.
After the staff interaction, the Secretary-General held a separate meeting with the UNAIDS Cabinet.


Feature Story
Innovation for the AIDS response focus as USAID head visits UNAIDS
27 January 2011
27 January 2011 27 January 2011
Dr Rajiv Shah, administrator of the United States Agency for International Development (USAID) with Mr Michel Sidibé, Executive Director of UNAIDS. 27 January 2011. Credit: UNAIDS.
Dr Rajiv Shah, administrator of the United States Agency for International Development (USAID) visited UNAIDS headquarters in Geneva to meet with Executive Director Michel Sidibé on 27 January.
During the meeting Mr Sidibé thanked Dr Shah for the continued strong partnership with the US government and shared his priorities for action for the AIDS response as outlined in the new UNAIDS Strategy. This strategy sets out ten key results aimed at achieving UNAIDS’ vision of Zero new infections, Zero discrimination and Zero AIDS-related deaths.
Under the leadership of Dr Shah USAID has recently embarked on a comprehensive reform effort, called USAID FORWARD, with an emphasis on development aid delivering results and driving innovation.
Dr Shah and Mr Sidibé discussed how to ensure that recent breakthroughs in research and development of new HIV prevention technologies, such as the microbicide gel Tenefovir, can reach the people who need them. Dr Shah and Mr Sidibé also considered how the two organizations could strategically work together to ensure HIV prevention efforts are evidence informed.
The United States of America is a leader in development of new HIV prevention technologies and is the largest donor to UNAIDS as well as the largest funder of aid towards the global AIDS response.
Related



Feature Story
“Score the Goals” comic book launched: Ten football Goodwill Ambassadors embark on a journey facing the challenges of the Millennium Development Goals
26 January 2011
26 January 2011 26 January 2011
In the comic UNAIDS International Goodwill Ambassadors Michael Ballack and Emmanuel Adebayor talk about HIV
Credit: 'Score the Goals' An educational comic book about the MDGs
A new comic book for children featuring Michael Ballack and other football stars who are United Nations Goodwill Ambassadors was launched on 24 January at the United Nations in Geneva, Special Adviser to the UN Secretary-General on Sport for Development and Peace, Mr Wilfried Lemke.
“Score the Goals: Teaming Up to Achieve the Millennium Development Goals” is a 32-page educational comic book aimed at 8 to 12 year old children to provides a fun interactive way to help understand and reflect on the eight Millennium Development Goals.
The story features ten football United Nations Goodwill Ambassadors, including Michael Ballack, Emmanuel Adebayor, Roberto Baggio, Iker Casillas, Didier Drogba, Luis Figo, Raúl, Ronaldo, Patrick Vieira, and Zinédine Zidane.
The star-studded team journey to play an “all-star” charity football game in support of the United Nations. On the way they shipwreck on a deserted island and the story explores how the team copes by team spirit and survivor skills with the challenges that life on a deserted island brings.
The story simultaneously educates and entertains the young readers who are also invited to take action through several activities provided in the adjoining educational guide. The reader is invited to learn about the world’s challenges in ending hunger, universal education, gender equity, child health, maternal health, HIV, environmental sustainability, global partnership.
In 2000, the largest gathering of world leaders at United Nations Headquarters in New York adopted the United Nations Millennium Declaration. The Declaration, endorsed by 189 countries, committed nations to a new global partnership to reduce extreme poverty and it set out a series of targets to be reached by 2015. These have become known as the Millennium Development Goals (MDGs).
Everybody should have equal access to information and I hope that with this comic book we can reach out to a large young audience with important messages
Michael Ballack, UNAIDS Goodwill Ambassador and football star
In the comic Michael Ballack and fellow UNAIDS International Goodwill Ambassador Emmanuel Adebayor talk about HIV in reference to Goal 6 which sets out by 2015 to have halted and begun to reverse the spread of HIV.
Michael Ballack who has been a UNAIDS International Goodwill Ambassador since 2006 is convinced of the importance of reaching young people with accurate information about HIV.
“I want people to know more about HIV as well as the other Millennium Development Goals because health and development are interlinked,” said Michael Ballack. “Everybody should have equal access to information and I hope that with this comic book we can reach out to a large young audience with important messages.”
The project has been carried out in a ‘One-UN’ spirit as an inter-agency collaboration between the UN Office for Sport for Development and Peace (UNOSDP), the UN Development Programme (UNDP), the Food and Agriculture Organization (FAO), the Joint United Nations Programme on HIV/AIDS (UNAIDS), the UN Department of Public Information (DPI), and the Stop TB Partnership.
The comic book is available in English, French and Spanish and other languages, including Arabic, Chinese and Russian, will be made available in the near future.
Related

Feature Story
Efficiency, results, and value for money top of discussions during visit of UK Secretary of State for International Development to UNAIDS
26 January 2011
26 January 2011 26 January 2011
Secretary of State for International Development Andrew Mitchell (right) and UNAIDS Executive Director Michel Sidibé. UNAIDS headquarters, 26 January 2011. Credit: UNAIDS
Secretary of State for International Development Andrew Mitchell met with UNAIDS Executive Director Michel Sidibé at UNAIDS headquarters on 26 January. The UK government has pledged to put the wellbeing of women and children at the centre of its international aid policy.
Mr Mitchell, who leads the Department for International Development (DFID) stressed the need for efficiency, results and value for money from the AIDS response. Mr Sidibé shared his vision of the priorities of the AIDS response including the new UNAIDS Strategy. He highlighted how collective investments in AIDS have brought unprecedented results including increased access to treatment and the prevention of mothers from dying and babies being infected with HIV.
Related

Feature Story
“Get the Facts, protect yourself”: World-class cricketers champion HIV campaign at 2011 Cricket World Cup
25 January 2011
25 January 2011 25 January 2011
Sri Lankan cricket player Kumar Sangakkara in a new public service announcement that encourages young people to inform themselves about HIV
Credit: International Cricket Council (ICC)
They may be rivals on the field of play, but international cricketing stars Virender Sehwag and Kumar Sangakkara have joined together to support a new “Think Wise” campaign ahead of the ICC Cricket World Cup 2011.
The players feature in a public service announcement—released today and available to all broadcasters across the globe—that encourages young people to inform themselves about HIV, take appropriate action to prevent HIV infection, and stand together against HIV-related stigma and discrimination. The new campaign is led by the International Cricketing Council (ICC), in partnership with UNAIDS and UNICEF.
“The ICC Cricket World Cup 2011 provides an opportunity to use our status as cricketers to deliver important social messages to the millions of supporters who will be watching the tournament across the world,” said India’s Virender Sehwag. “I hope this public service announcement can encourage young people to get the facts and protect themselves from HIV.”
The ICC Cricket World Cup 2011 provides an opportunity to use our status as cricketers to deliver important social messages to the millions of supporters who will be watching the tournament across the world
Virender Sehwag, India cricket team
Sehwag and Sangakkara have been active supporters of the ICC partnership since it was formed in 2003, visiting HIV projects at ICC events and promoting HIV prevention and stigma reduction messages. Other cricketing stars in the partnership include Graeme Smith (South Africa), Shakib-Al-Hasan (Bangladesh) and Ramnaresh Sarwan (West Indies).
“It is important that young people around the world have access to the right information to help them make informed decisions and break down stigma and discrimination,” said Sri Lanka’s Kumar Sangakkara. “Through this public service announcement, I want to help stop the spread of HIV.”
A number of other “Think Wise” activities are planned during this year’s Cricket World Cup, which runs from 19 February through 2 March, with matches across India, Bangladesh and Sri Lanka. Cricket players will participate in a series of interactions focused on HIV prevention with local community groups in the three host countries. Cricket teams will wear red ribbons on their shirts in key matches during the competition and HIV prevention messages will be promoted at venues on all match days.
Notes to editors
The public service announcement is available to broadcasters, for editorial use, from an ICC ftp site. Visit via Windows Explorer ftp://internationalcricketcouncil.net/ThinkWise.
Username: thinkw-read
Password: icchiv_123



Feature Story
UNAIDS mission highlights HIV response among female sex workers
24 January 2011
24 January 2011 24 January 2011
Ms Jan Beagle, Deputy Executive Director of UNAIDS with H.E the Vice President and Chair of the Ghana AIDS Commission Mr John Dramani Mahama. Credit: UNAIDS
About 2% of the adult population in Ghana is living with HIV—a figure that has remained unchanged for the past 10 years. The number of new HIV infections in this West African nation, estimated at about 22 000 per year, has also stabilized over the past decade.
Despite a relatively stable HIV prevalence in the country, several populations appear to be at high risk of HIV, including female sex workers and men who have sex with men. According to a recent survey, HIV prevalence among sex workers in Accra and Kumasi was 25% in 2009. Sex work in Ghana also contributes to a significant proportion of new HIV infections.
In an official mission to Ghana, Jan Beagle, UNAIDS Deputy Executive Director (Management and External Relations), met with a group of female sex workers at the Accra headquarters of the West African Program to Combat AIDS and STI (WAPCAS), a non-government organization that develops and implements HIV programmes for female sex workers, their clients and men who have sex with men.
With 20 satellite offices nationwide, the organization provides a range of services, including reproductive health education, condom promotion, HIV counselling and testing, and clinical services such as the management of sexually transmitted infections. WAPCAS is also working closely with UNAIDS, UNFPA and local police to address discrimination and human rights abuses against sex workers.
All forms of discrimination against key affected populations, such as sex workers, block access to HIV services and impact the quality of care for people living with HIV
Jan Beagle, Deputy Executive Director of UNAIDS
“I can’t stop sex work because I have five children that I am taking care of by myself,” said one female sex worker, during the visit with Ms Beagle. “Engaging in sex work is the only way I can provide for my family since I don’t have any employable skills,” she added. Other sex workers told the Deputy Executive Director that they were unable to report human rights abuses to police because their work is considered illegal in Ghana.
Ms Beagle said that UNAIDS is serious about focusing HIV resources and attention on sex workers, as they form one of the most important populations at higher risk of HIV infection in Ghana. “All forms of discrimination against key affected populations, such as sex workers, block access to HIV services and impact the quality of care for people living with HIV. We must do more to address stigma and discrimination in Ghana.”
During her mission, Mr Beagle met with Mr John Dramani Mahama, Vice President of the Republic of Ghana. Ms Beagle congratulated Ghanaian authorities on the political and financial commitment they have shown in the national AIDS response, while underscoring the urgent need to prioritize HIV resources for populations at higher risk of HIV infection.
Mr Mahama reiterated his Government’s commitment at the highest level to “vigorously combat” the HIV epidemic in Ghana. He pledged to provide the necessary resources to eliminate mother-to-child transmission of HIV and reduce stigma and discrimination against key affected populations.
Related
 Impact of US funding cuts on HIV programmes in Ghana
Impact of US funding cuts on HIV programmes in Ghana
08 April 2025
Feature Story
UNAIDS and IOM sign agreement to improve access to HIV services for migrants
21 January 2011
21 January 2011 21 January 2011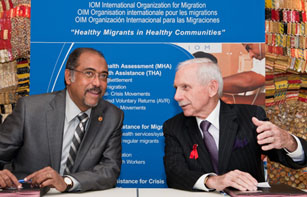
Mr Michel Sidibé, Executive Director of UNAIDS and Mr William Lacy Swing, IOM Director General signed a new cooperation agreement to overcome HIV-related challenges faced by many migrants. 21 January, 2010. Credit: UNAIDS/ D. Bregnard
The Joint United Nations Programme on HIV/AIDS (UNAIDS) and the International Organization for Migration (IOM) today signed a new cooperation agreement to overcome HIV-related challenges faced by many migrants.
The agreement seeks to integrate human rights and the needs of migrants and mobile populations into national and regional HIV responses and ensure universal access to HIV prevention, treatment, care and support.
“Healthy migrants contribute significantly to achieving healthy economies,” said Michel Sidibé, Executive Director of UNAIDS. “States and other actors in the AIDS response have a fundamental duty to ensure the safety and well-being of migrants—this must include access to HIV services.”
Under the new agreement, IOM and UNAIDS will also focus on enhancing social protection for migrants affected by HIV; stopping violence against migrant women and girls and removing punitive laws, policies, practices, stigma and discrimination related to HIV and population mobility that block effective responses to AIDS.
States and other actors in the AIDS response have a fundamental duty to ensure the safety and well-being of migrants—this must include access to HIV services
Michel Sidibé, Executive Director of UNAIDS
"Government and civil society are becoming increasingly concerned about the potential vulnerability of migrants to HIV infection. By strengthening our partnership and pooling our respective expertise on HIV and migrants, our two organizations can address this critical issue more effectively," said IOM Director General William Lacy Swing.
In addition UNAIDS and IOM will work on strengthening technical support to help governments, regional institutions and civil society reduce vulnerability to HIV among mobile and migrant populations. The two organizations will also continue cooperation on research to deepen the understanding of HIV and population mobility.
IOM and UNAIDS have a long-standing partnership, formalized in a 1999 Cooperation Framework which was updated in 2002. This is now replaced by today’s new agreement. IOM’s HIV and population mobility programme not only complements the work of UNAIDS globally, but the Organization is also part of the UN Joint Team on HIV/AIDS at the country level.
By strengthening our partnership and pooling our respective expertise on HIV and migrants, our two organizations can address this critical issue more effectively
William Lacy Swing, IOM Director General
UNAIDS is committed to improving access to HIV services for migrants and has included mobility in its Strategy 2011-2015 which states that HIV responses must create space to involve marginalized and disempowered people, such as migrants.
HIV projects are a significant part of IOM’s work, comprising the second largest area of migrant health projects implemented after health assessments. They are part of IOM’s broader efforts to ensure migrant access to health services regardless of migration status, throughout the migration process.
Related
 Keeping up the momentum in the global AIDS response
Keeping up the momentum in the global AIDS response
24 April 2019
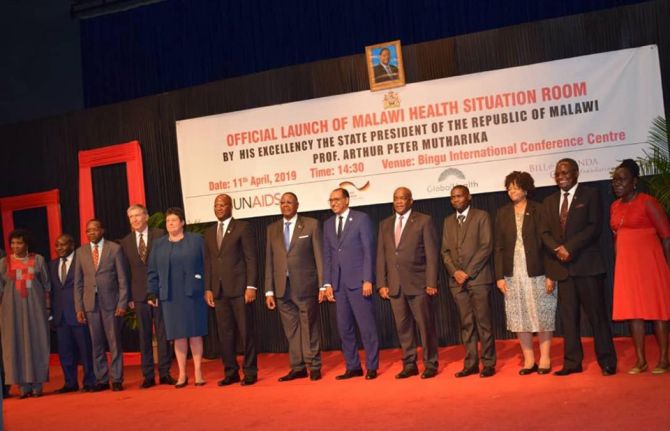 Malawi launches its health situation room
Malawi launches its health situation room
12 April 2019
 Learning lessons on evaluation
Learning lessons on evaluation
02 April 2019