
Feature Story
'Never abandon, never give up’: ILO film helps China’s migrant workers challenge AIDS stigma
30 April 2009
30 April 2009 30 April 2009

Wang Baoqiang, star actor and former migrant construction worker is now a spokesperson for the ILO HIV/AIDS project in China Credit: courtesy of ILO
Zhang Xiao Hu is one of China’s estimated 200 million migrant workers. He is also one of the stars of ‘Never abandon, never give up’, a short Charlie Chaplin-style film aimed at reducing HIV stigma and promoting condom use among the country’s migrant workers. Beginning on 4 May, the International Labour Organization (ILO) and Mega-info Media, the company which runs China’s national railway station television network, will begin screening the film in 500 stations in 450 cities across the country. Over a three month period, 40 million people will have an opportunity to see the film.
In the film Zhang plays a construction worker stigmatized because he is living with HIV. This mirrors his real life situation as he is China’s first internal migrant worker to speak out publicly about his HIV status and has suffered stigma in the past from colleagues. As he says, “No one wanted to work with me, eat with me or share a dormitory.”
Leading filmmaker Gu Changwei
‘Never abandon, never give up’ is produced and directed for the ILO by Gu Changwei, a winner at the 2005 Berlin Film Festival and considered one of the leading filmmakers working in China today. Established star Wang Baoqiang, who is now serving as a spokesperson for the ILO HIV/AIDS project in China, also takes a lead role in the movie. He befriends Zhang Xiao Hu at his workplace and uses his celebrity persona to encourage his colleagues to cast aside their prejudices.
‘Hometown Fellows’ campaign
The project forms part of the ‘Hometown Fellows’ campaign where the ILO, in partnership with the Ministry of Labour, employer and worker bodies, and the State Council AIDS Working Committee Organization is collaborating with 19 large-scale enterprises in construction, mining and transport sectors in China’s provinces most affected by HIV. Although overall prevalence of the virus is relatively low in China (UNAIDS reported a 0.1% prevalence in 2008), there are pockets of high infection among specific populations and in some localities. With support from grass roots non-governmental organizations, the ILO is carrying out a comprehensive, multi-channel behaviour change programme for 190,350 internal migrant workers in Guangdong, Yunnan and Anhui provinces.
According to Constance Thomas, Director of the ILO in China, partnering with authorities on such projects, “helps us reach out to the workers for social protection to ensure their occupational safety and health…They do have the right to work in China and they have the right not to be discriminated against.”
The ‘Hometown Fellows’ project is intended to address high HIV-related stigma and low condom use among migrants and taps into powerful social networks among migrant workers who often move from rural areas and work together in large cities throughout China.
Formative research among the migrants shows a strong social bond based on common provincial origin that is potentially influential on attitudes and behaviour. This is in sharp contrast to migrant worker perceptions of health officials, company management and receiving communities, where there is, typically, considerable distrust and a sense of alienation.
The ILO behaviour change communication strategy has two tiers. Firstly, it has developed a range of communication tools based on the hometown fellowship concept where key message are delivered through migrant voices. Never abandon, never give up forms part of this intervention.
This movie is an excellent production which can help to reduce stigma and discrimination against people living with HIV far beyond the labour sector. It addresses not only stigma related to HIV, but also vulnerabilities linked with living at the margins of society.
Dr Bernhard Schwartlander, UNAIDS Country Coordinator in China
Secondly, working through enterprise structures, the programme taps into existing migrant social networks to deliver peer education in the workplace, dormitories and nearby entertainment areas. This peer education is reinforced through group training in enterprises as well as targeted messages delivered through company owned television and radio channels.
Dr Bernhard Schwartlander, UNAIDS Country Coordinator in China applauds this production, "This movie is an excellent production which can help to reduce stigma and discrimination against people living with HIV far beyond the labour sector." He added, "It addresses not only stigma related to HIV, but also vulnerabilities linked with living at the margins of society."
Migrant workers make up some 15% of the total Chinese population according to official estimates and they are considered vulnerable to HIV due to challenging social conditions, low HIV knowledge and lack of access to quality health services.
Right Hand Content
Cosponsors:
Feature stories:
‘Love and Relationships’: Film festival in Cambodia addresses HIV prevention (06 April 2009)
New report shows Asian migrant women in the Arab states have heightened vulnerability to HIV (10 March 2009)
Love in a Time of HIV (19 December 2008)
Powerful film brings AIDS issues to communities in Democratic Republic of Congo (16 June 2008)
Publications:
Migrants and HIV: Far away from home club (pdf, 899 Kb.)
Reducing HIV stigma and discrimination: a critical part of national AIDS programmes (pdf, 598 Kb.)
Art for AIDS (pdf, 2.11 Mb.)
Related



Feature Story
Funding for AIDS drugs in jeopardy as global financial crisis hits health sector
28 April 2009
28 April 2009 28 April 2009The current crisis in financial markets and the world economy is having a profound effect on both governments’ global development commitments and national resources. Households already most vulnerable to poverty, risk further impoverishment as unemployment rises and incomes are reduced. There is widespread concern that progress in health and education will be severely undermined.
This is the second in a series of articles on the how the economic downturn impacts people already affected by HIV and how investment in sustainable financing is critical for global AIDS and development responses. The World Bank has just published a report that explores these issues in depth.

Averting a Human Crisis during the Global Downturn: Policy Options from the World Bank's Human Development Network states that a number of countries are already facing shortages of AIDS drugs due to the economic crisis.
Credit: Courtesy of the World Bank
The worldwide economic downturn may already be causing hardship in supplying life-saving drugs to people with HIV, according to a new World Bank report which highlights the clear and rising human cost of the current financial climate.
Averting a Human Crisis During the Global Downturn: Policy Options from the World Bank's Human Development Network, reports preliminary findings from a survey in 69 countries showing that 8 countries already face shortages of antiretroviral (ARV) drugs or other disruptions to AIDS treatment. The survey, conducted by the World Bank, UNAIDS and the World Health Organization last month also contends that, in total, respondents in 22 countries in Africa, the Caribbean, Europe and Central Asia, and Asia and Pacific expect the crisis to impact treatment programmes over the coming year. Together, these countries are home to more than 60 percent of people worldwide on ARVs.
This is a serious development. Despite rapid recent expansion in the numbers of people receiving treatment, two thirds of those in need of such drugs still do not get them. And unmet need is growing faster than treatment access is expanding. The global crisis seems likely to exacerbate the situation.
"This new report shows that people on AIDS treatment could be in danger of losing their place in the lifeboat,” says Joy Phumaphi, the World Bank's Vice President for Human Development and former Health Minister for Botswana.
Prevention programmes in jeopardy
We cannot afford a ‘lost’ generation of people as a result of this crisis. It is essential that developing countries and aid donors act now to protect and expand their spending on health, education and other basic social services and target these efforts to make sure they reach the poorest and most vulnerable groups.
Joy Phumaphi, the World Bank's Vice President for Human Development
HIV prevention programmes are also in jeopardy. The report states that survey respondents in 34 countries, where 75 percent of people with the virus live, expect prevention programmes for their key populations at higher risk (including sex workers and people who inject drugs) to be adversely affected as they are marginalized and tend to get lower priority than say pregnant women and children.
The world has made an international commitment to providing universal access to HIV prevention, treatment, care and support services to those in need by 2010. The global scale up towards this key goal, which has been gathering momentum, may well be threatened by what the report calls “these extraordinarily challenging times for the global economy.”
In Averting a Human Crisis During the Global Downturn, the Bank is encouraging countries which depend extensively on external donor AIDS financing to identify impending cash shortages as far as possible in advance, and to liaise with the Bank and other partners to help to mobilize 'bridge financing' that prevents interruptions to AIDS treatment. At the same time, the Bank warns that maintaining and expanding effective HIV prevention programmes during the current crisis is essential to guard against a resurgence of new infections.
Potential cuts in health and education financing
The World Bank is concerned that the downturn will lead to cuts in health and education financing across the board, not only in the sphere of AIDS. The report also shows how previous crises have forced developing countries to cut back on spending in these areas. Evidence from past downturns in Argentina, Indonesia, Thailand, and Russia shows that governments were forced to cut health services as a result of shrinking budgets and that returning health spending to pre-crisis levels took up to 10-15 years.
”We cannot afford a ‘lost’ generation of people as a result of this crisis,” Phumaphi contends. “It is essential that developing countries and aid donors act now to protect and expand their spending on health, education and other basic social services and target these efforts to make sure they reach the poorest and most vulnerable groups.”
In support of this strategy, on 24 April the World Bank stated that it was mobilizing up to US$ 3.1 billion this year in health financing to help poor countries battle threats to their social services during the global crisis. This effectively triples Bank support from US$ 1.0 billion in 2008 and will be used to strengthen health systems in poor countries, boost their performance in preventing and treating communicable diseases, and improving child and maternal health, hygiene and sanitation.
The Bank also said it was doubling its education financing this year in low- and middle-income countries to US$ 4.09 billion.
This report draws heavily on ongoing collaborative work by the World Bank, UNAIDS and WHO which will be released soon in a joint publication. Information was collected by agency representatives working closely with the National AIDS authorities in 69 low- and middle-income countries, which together include most people on treatment in the developing world. Preliminary conclusions are referenced here for consideration at the 2009 IMF World Bank Spring Meetings in Washington DC.
Funding for AIDS drugs in jeopardy as global fina
Cosponsors:
Feature stories:
HIV and high food prices (01 April 2009)
Minister of Foreign Affairs of the Russian Federation discusses financial crisis with UN agencies (09 March 2009)
As global economy slows International Health Partners push for faster health progress (12 February 2009)
Publications:
Averting a Human Crisis During the Global Downturn: Policy Options from the World Bank's Human Development Network (pdf, 1.09 Mb.)
Related



Feature Story
International Technical Consultation on ‘Positive Prevention’
27 April 2009
27 April 2009 27 April 2009 The concept of ‘positive prevention’ provides an opportunity to highlight the prevention needs of people who know their positive serostatus.
The concept of ‘positive prevention’ provides an opportunity to highlight the prevention needs of people who know their positive serostatus.Ever since HIV testing was developed in the early days of the epidemic, the role of people living with HIV in HIV prevention has been an important aspect of the AIDS response. Following the advent of combination antiretroviral treatment which significantly prolongs life and improves quality of life for people living with HIV, there have been increasing calls to incorporate what is known as ‘positive prevention’ in the continuum of prevention and care programmes and services.
The concept of ‘positive prevention’ provides an opportunity to highlight the prevention needs of people who know their positive serostatus, and is a useful lens through which to understand the important linkages between prevention, treatment, care and support.
However, despite increasing funding directed towards positive prevention, there is a lack of clear understanding globally and regionally of the concept, objectives and programmatic features of ‘positive prevention’, either within the community and representatives of people living with HIV, or between civil society and other partners.
As a direct consequence, the Global Network of People living with HIV (GNP+) and UNAIDS are convening a technical consultation on 27-28 April 2009 in Tunisia on the subject to help develop a common understanding of ‘positive prevention’, as well as guidelines and action plans to inform policies and programmes.
The term ‘positive prevention’ itself will be discussed during the technical consultation as, even though it is the most commonly used term, other terms are also used by different organizations and programmes such as ‘Prevention and Care for People Living with HIV/AIDS’ or ‘prevention with HIV-positive people’.
Participants at the consultation will represent civil society, government agencies, UNAIDS Cosponsors and Secretariat and international development agencies. A majority of the participants will be people living with HIV as the conversation around positive prevention has too often occurred without the involvement of people living with HIV at the design stage and has led to significant shortcomings in most current approaches.
The technical consultation follows the significant Positive Leadership Summit held in Mexico in 2008 and is part of an ongoing process to ensure that positive prevention efforts are based on a solid consensus among positive people. To that end, experts will identify strategies to gather experiences and knowledge of stakeholders, in particular people living with HIV at regional, national and local levels.
 If the prevention needs of positive people are to be adequately addressed, people who know they are living with HIV must be involved in defining and developing programmes.
If the prevention needs of positive people are to be adequately addressed, people who know they are living with HIV must be involved in defining and developing programmes.It is expected that the meeting will facilitate the development of a set of principles that will guide the work of and partnerships between multilateral, bilateral, governmental and civil society organizations in designing positive prevention programmes. Participants will also develop recommendations on the scaling up of programmes and policies, informed by the local context.
“Positive prevention” programmes
Many HIV programmes worldwide seek to include people living with HIV in their prevention efforts. Diverse programmatic activities are undertaken, including support for self-help groups and community empowerment, counselling in the context of HIV testing or of family planning, engagement of positive people in education programming (e.g. in delivering personal testimonies), and behaviour change programming directed at HIV-positive people or discordant partners. The aims of these programming efforts vary widely, and are not always explicit or consistent. Quite often, positive prevention programmes have focused on HIV testing and so are seen as irrelevant to people who already know their serostatus. Most existing interventions focus almost entirely on preventing the onward transmission of HIV, which may be counter-productive to programmes intended to address prevention, care and support for HIV positive people in a holistic manner.
If the prevention needs of positive people are to be adequately addressed, people who know they are living with HIV must be involved in defining and developing programmes. A human rights approach combating stigma and discrimination is essential to the success of positive prevention. Positive prevention requires addressing social vulnerabilities such as poverty, gender-based violence, xenophobia and homophobia. It is also inextricably linked with access to treatment, care and support.
While most agree that among the measures of success of positive prevention is the reduction of HIV transmission, it is also widely felt that positive prevention should not be exclusively about preventing onward transmission of HIV. The discussion about positive prevention needs to explore the efforts of people who know they are living with HIV to learn and practice ways to promote their own health and prevent disease.
Right Hand Content
Feature stories:
Positive Leadership Summit 2008 (31 July 2008)
HIV positive leaders meet in Monaco (25 January 2008)
Multimedia:
Listen to Rodrigo Pascal, UNAIDS Partnerships Officer
External Links:
Global Network of People Living with HIV/AIDS (GNP+)
Publications:
Practical guidelines for intensifying HIV prevention (pdf, 1.87 Mb)
Related


Feature Story
World AIDS Campaign: An opportunity to spark changes in society
24 April 2009
24 April 2009 24 April 2009
(from left) Allyson Leacock, Chair of the Steering Committee of World AIDS Campaign; Michel Sidibé, Exective Director of UNAIDS; Marcel van Soest, Executive Director of The World AIDS Campaign.
Credit: UNAIDS/O. O'Hanlon
AIDS presents a political opportunity to spark changes in society and talk about issues like human rights, homophobia and sex education according to UNAIDS Executive Director Michel Sidibé.
"You will never make a difference if you look at AIDS in isolation," Mr Sidibé said during his first meeting with the head of the World AIDS Campaign in Geneva.
Executive Director of The World AIDS Campaign Marcel van Soest said, “AIDS is a disaster beyond a health issue, it’s a human rights issue too.”
AIDS is a disaster beyond a health issue, it’s a human rights issue too.
Marcel van Soest, Executive Director of the World AIDS Campaign
International representatives from a wide range of communities including The Global Network of People Living with HIV/AIDS (GNP+) and The Global Unions AIDS Programme attended the meeting.
UNAIDS and the World AIDS Campaign reaffirmed their intention to put human rights and universal access to treatment, prevention, care and support at the centre of their campaigning agendas.
In addition to talks on how to help guarantee continuation of treatment, and to stop discrimination against people living with HIV participants looked at ways to invigorate campaigning at local and national levels.
The 2009 World AIDS Day Campaign will be unveiled in Nairobi, Kenya early in June.
Right Hand Content
Partners:



Feature Story
Official launch of the V Latin American and Caribbean Forum on HIV/AIDS and STDs
24 April 2009
24 April 2009 24 April 2009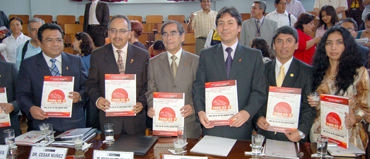 (L to R): Dr Jose Luis Sebastian Mesones, Technical Secretariat of the Horizontal Technical Cooperation Group and National AIDS Coordinator from Peru, UNAIDS Regional Director for Latin America, César Antonio Núñez, Minister of Health of Peru, Dr Oscar Raúl Ugarte Ubilluz, Minister of Labour, Jorge Elisban Villasante Aranibar, Director of Health Services of Peru, Dr Edward Cruz Sánchez and Mrs. Guiselly Flores Arroyo, representing the Latin American network of people living with HIV.
(L to R): Dr Jose Luis Sebastian Mesones, Technical Secretariat of the Horizontal Technical Cooperation Group and National AIDS Coordinator from Peru, UNAIDS Regional Director for Latin America, César Antonio Núñez, Minister of Health of Peru, Dr Oscar Raúl Ugarte Ubilluz, Minister of Labour, Jorge Elisban Villasante Aranibar, Director of Health Services of Peru, Dr Edward Cruz Sánchez and Mrs. Guiselly Flores Arroyo, representing the Latin American network of people living with HIV.Credit: Ministry of Health of Peru/J.E.Castro Varillas
The V Latin American and Caribbean Forum on HIV/AIDS and STD’s, FORO 2009 was officially announced on Thursday 16th April in Lima. The Forum will take place in Peru’s capital from 22nd to 26th June under the theme “Health is our right, universal access is our goal, no discrimination our challenge”.
FORO 2009 was officially launched by the Minister of Health of Peru, Dr Oscar Raúl Ugarte Ubilluz together with the Minister of Labour, Jorge Elisban Villasante Aranibar, Director of Health Services of Peru, Dr Edward Cruz Sánchez, UNAIDS Regional Director for Latin America, César Antonio Núñez, Mrs. Guiselly Flores Arroyo, representing the Latin American network of people living with HIV, and Dr Jose Luis Sebastian Mesones, Technical Secretariat of the Horizontal Technical Cooperation Group and National AIDS Coordinator from Peru.
Health Minister Ugarte invited all stakeholders working in Latin America and the Caribbean to come to Lima and engage in an open discussion about universal access to HIV prevention, treatment, care and support in the region and single out the gaps in the response. This was reinforced by Labour Minister Villasante, who also raised the importance of reducing stigma and discrimination in the workplace in particular.
During the launch, UNAIDS Regional Director for Latin America, César Antonio Núñez stressed that FORO 2009 “offers an opportunity to governments and civil society to review progress made in the region towards universal access to HIV prevention, treatment, care and support under a human rights perspective.”
Dr Núñez pointed out to the audience that there are close to 500 new HIV infections in the region every day and highlighted the urgency to prioritize HIV prevention efforts as well as the need to reject all forms of stigma and discrimination against people living with HIV and people most at risk of HIV infection.
The main objective of the forum is to promote coordinated national and regional efforts to achieve universal access to HIV prevention, treatment, care and support in the region. The meeting will also serve as a platform to share lessons learned to improve practices on HIV interventions, prevention, research and access to information.
Furthermore, the meeting will review the response to AIDS through analysis of progress made in the fulfilment of the International HIV commitments made by governments in the region. The forum will highlight recent successes, as well as outlining the challenges faced in the region and ways to overcome them. Finally, it will promote the greater participation of all the social actors in response to the epidemic.
Some 4,000 people are expected to attend this year’s Latin American and Caribbean Forum on HIV/AIDS and STD’s. Participants will include people living with HIV, civil society groups, non-governmental and governmental institutions, academia, the media, UN agency representatives and the private sector.
Official launch of the V Latin American and Carib
External links:
Related


Feature Story
New Country Response Information System to strengthen national M&E
24 April 2009
24 April 2009 24 April 2009
UNAIDS announces the launch of the Country Response Information System (CRIS) version 3, which is a tool for managing national HIV data. In support of Three Ones principles, and especially the principle of one national monitoring and evaluation system, CRIS3 enables national AIDS authorities to store, share and utilize the national HIV data in an effective manner with national and international counterparts.
The new released version brings improved features for monitoring national programmes and progress towards set national targets, such as those of universal access. Version 3 is more flexible and adaptable to meet the requirements of individual countries, using internationally agreed standards for HIV monitoring and evaluation.
Some of the main highlights of CRIS3 include:
- Ability to import indicators from the Indicator Registry, and flexibility in indicator data entry;
- Intuitive and clear user interface, reducing need for user training and time needed for use;
- Options of using CRIS3 either via web in countries with good internet access, or as a standalone application in settings with limited connectivity with data exchange between systems; and
- Improved technical and user support for national installations and configuration.
Supporting national HIV databases
As one of its mandates, UNAIDS provides guidance and develops tools for countries to better plan and manage their national monitoring and evaluation (M&E) system. Two of the most relevant tools recently developed by UNAIDS to facilitate the monitoring and evaluation of national HIV responses are the Indicator Registry (repository of standardized set of internationally agreed indicators) and CRIS3 (tool for monitoring national response to AIDS). Used together they complement each other as countries can use the indicator registry to select standardized indicators for their national monitoring purposes and use them in CRIS3 for data collection, storing, analysis and reporting.
CRIS3 has been developed with country needs in mind, emphasizing advanced programmatic features for national programme monitoring, including multiple monitoring plans that can accommodate the reporting needs of different donors, such as The Global Fund to fight AIDS, Tuberculosis and Malaria, the United States President’s Emergency Plan for AIDS Relief (PEPFAR) and others.
CRIS3 is at its best for use of national and district M&E officers as they have various backgrounds and skills to use different M&E tools. UNAIDS supports capacity building in M&E skills through different means, such as M&E trainings and CRIS specific trainings. Regional training events are organized during 2009 and the UNAIDS Country Monitoring systems team can be contacted for further details.
For more information on CRIS3 you may visit the support web-site: www.cris3.org or contact the Country Monitoring Systems team: cris@unaids.org
Mr. Taavi Erkkola (erkkolat@unaids.org).
Right Hand Content
Related



Feature Story
Consultation held on definition and measurement of concurrent sexual partnerships
24 April 2009
24 April 2009 24 April 2009It has long been suggested that concurrent sexual partnerships are one component responsible for creating sexual contact networks conducive to the rapid spread of HIV. Recently the idea has gained prominence and momentum, with national HIV programmes beginning to plan prevention campaigns targeted at reducing concurrent partnerships. However, in both the scientific and programmatic communities, research and discussion about concurrent partnerships and their role in the spread of HIV have been impeded by lack of clarity about the definition and appropriate indicators of concurrency.
On 20-21 April 2009, the UNAIDS Reference Group on Estimates, Modelling, and Projections convened a meeting to discuss the definition and measurement of concurrent sexual partnerships in Nairobi, Kenya. The meeting brought together a group of 35 experts, representing those working on large-scale cross-sectional surveys, longitudinal cohort studies, researchers using sexual behaviour and concurrent partnership data, and monitoring and evaluation specialists.
The main aim of the meeting was to reach consensus on what should be measured in large-scale surveys to best capture the amount of concurrency in a population and to monitor the impact of programmes. Topics covered included a history and overview of concurrent partnerships and HIV, comparisons of the definitions, methods, and questions used to measure concurrency, the reliability of sexual behaviour data, the measurement of concurrency in large cross sectional surveys and in longitudinal cohort studies.
Overlapping sexual partnerships where sexual intercourse with one partner occurs between two acts of intercourse with another partner.
Agreed definition of "concurrent partnerships"
At the close of the meeting, meeting participants reached consensus that the definition of concurrent partnerships should be “overlapping sexual partnerships where sexual intercourse with one partner occurs between two acts of intercourse with another partner”, and recommended that the point prevalence of concurrent partnerships in the adult population, that is the proportion of adults aged 15-49 reporting more than one ongoing sexual partnership at an instant in time, be used as the main indicator of concurrent partnerships in a population. This measure best distinguishes between concurrency and rapid serial monogamy.
Additionally, the Reference Group discussed other useful indicators of concurrent partnerships in a population (including the cumulative prevalence of concurrent partnerships in the adult population over a 1 year period), and made recommendations for further research into the methods of measuring concurrent partnerships and sexual behaviour, the relationship between concurrency and HIV transmission, and social norms around concurrent partnerships.
A set of specific recommendations on how to capture the proposed indicator will be provided to the UNAIDS Monitoring and Evaluation Reference Group and to the implementing organizations of large household surveys by end of April, 2009. A full meeting report will be available by end of May, 2009.
Right Hand Content
Feature stories:
Talking about OneLove in Southern Africa (06 February 2009)
Related


 An HIV vaccine: who needs it?
An HIV vaccine: who needs it?
21 July 2021
Feature Story
UNODC and Brazil promote action on AIDS in prison settings
22 April 2009
22 April 2009 22 April 2009A version of this story is also published at UNODC.org

The first national consultation on HIV in prison settings took place in Brasilia 31 March to 2 April 2009.
Credit: UNODC
Much more needs to be done to improve AIDS prevention, treatment and care services in Brazil’s prisons. This was the major conclusion emerging from the first national consultation on HIV in prison settings which took place in Brasilia between 31 March and 2 April.
Organized by Brazil's Ministry of Health and Ministry of Justice in partnership with the United Nations Office on Drugs and Crime (UNODC), the objective of the consultation was to discuss and propose an agenda with an action plan to provide prevention, treatment, care and support services aimed at addressing HIV, other sexually transmitted infections and co-infections such as tuberculosis and hepatitis in prisons.
"UNODC is committed to supporting the Government of Brazil in the provision of HIV prevention and care services to the prison population," said UNODC Representative for Brazil and the Southern Cone, Giovanni Quaglia.
The national consultation was attended by around 150 professionals. These included specialists from the key ministries, representatives from all 26 states of Brazil and the Federal District (where the capital is located), health professionals working in prison settings, members of the national harm reduction network, representatives of the Brazilian segment of the International Commission for Catholic Prison Pastoral Care and members of the National Network of People Living with HIV/AIDS.
UNODC is committed to supporting the Government of Brazil in the provision of HIV prevention and care services to the prison population.
Giovanni Quaglia, UNODC Representative for Brazil and the Southern Cone
As in most countries, Brazil has a higher HIV prevalence in the prison population than among the general population. According to the most recent research, a local study published in 2007, found rates of 5.7% among certain prisoners. In contrast, UNAIDS reports that by the end of 2007, general adult prevalence was 0.6%.
It is estimated that the country has approximately 420,000 prisoners living in often violent conditions where overcrowding, lack of access to medical services and unsanitary surroundings can lead to greater vulnerability to HIV and other infectious viruses such as tuberculosis and hepatitis. These conditions can also increase AIDS-related deaths and undermine attempts to implement an effective response to the epidemic in prisons.
Liliana Pittaluga, Technical Adviser at the Prevention Unit of the National STD and AIDS Programme, said that the consultation was a symbol of the solid partnership between the Government of Brazil and UNODC. "The cooperation between sectors is crucial to improve the health care and prevention services made available inside prison settings. We are confident that the results of this consultation will not only result in an exchange of experiences, but also in building a process of actions that will have a positive effect in the prison system at the country level."
The main outcome of the consultation was the commitment made by the Ministry of Health, the Ministry of Justice and UNODC to form a working group which will design a national operative plan with guidelines, targets and deadlines. In addition, civil society organizations, the Pan-American Health Organization (PAHO) and UNAIDS will be part of this group.
As well as UNODC, UNAIDS and PAHO/World Health Organization, also participating in the meeting were the United Nations Educational, Scientific and Cultural Organization (UNESCO) and the United Nations Population Fund (UNFPA). Health and justice experts from the Southern Cone region also attended as observers, at the invitation of UNODC.
Right Hand Content
Cosponsors:
Feature stories:
ICASA 2008: HIV in prison settings (06 December 2008)
Publications:
HIV and prisons in sub-Saharan Africa (pdf, 2.12 Mb)



Feature Story
AIDS responses in action in rural Ethiopia
22 April 2009
22 April 2009 22 April 2009
UNAIDS Executive Director Michel Sidibé joins a village “community conversation” in the Tigray Region of Ethiopia, 800kms from Addis Ababa, 22 April 2009. Credit: UNAIDS/Y.Gebremedhin
Across Ethiopia, community initiatives and local government are coming together to make a difference in the AIDS response. During his official travel to the country, UNAIDS Executive Director Michel Sidibé visited some of the programmes and projects putting into action the goals of universal access to HIV prevention, treatment, care and support services.
Adegude Health Center
At the heart of health service delivery in Ethiopia are the government-run local health centres which deliver primary health services such as family health, communicable disease prevention and control, including HIV, and health education.
Michel Sidibé was invited to visit the Adegude Health Center, one of five local health centres in Hintalowagrit District, which provides voluntary HIV counseling and testing services, as well as prevention of mother to child transmission and HIV treatment. Staff working at the centre gave an overview of the HIV services that they deliver in this rural area of Ethiopia to Mr Sidibé and shared their achievements as well as the challenges they face. District health office officials also shared experience of coordinating the multi-sectoral AIDS response, implementation of HIV programmes and service delivery.
Community conversations
Governments, people living with HIV, civil society leaders, and partners—we all need creative platforms to join in open discussion of the issues and identify ways to move forward together in the AIDS response.
Michel Sidibé, UNAIDS Executive Director
Mr Sidibé also had an opportunity to observe one of the “community conversations” in Hiwane Kebele where a cross-section of people—women and men, old and young, people living with HIV, representatives from women’s associations and youth groups join local religious and traditional leaders who have the ability to influence and bring change—regularly come together.
“Community conversations” are taking place across rural Ethiopia and studies show that they can be agents of change in the AIDS response. Once a week or fortnight in villages, or “Kebeles”, up to 70 people gather for a couple of hours with trained local facilitators to exchange their views on a range of social topics.
The village gatherings enable taboos to be aired and misunderstandings about sex and AIDS to be clarified. Traditional practices that may be factors in the spread of HIV are also discussed.
The “conversations” have changed opinion and even translated into action. For example, in some localities groups have condemned early marriage and committed to protecting school girls from discontinuing their education. Others decided to stop female genital cutting in their areas or some participants reached a consensus to avoid practices like widow inheritance. The importance of leveraging AIDS responses to deliver broader development results including gender equality and human rights is a point often emphasized by Mr Sidibé.
The local events also enable issues—such as stigma—to be explored collectively and can be a forum from which community actions are initiated such as HIV prevention, home based care, support for orphans, and increased take up of voluntary counselling and testing.
Facilitators explained how community conversations were first developed by UNDP and piloted from 2003 to 2004 in Ethiopia. The pilot was more successful than expected and federal authorities have since made community conversations a priority strategy for community mobilization across the country.
“The local community conversation I have witnessed is an inspiration. Governments, people living with HIV, civil society leaders, and partners—we all need creative platforms to join in open discussion of the issues and identify ways to move forward together in the AIDS response,” said Mr Sidibé.
People living with HIV in the region

(from left): Hailemariam Kiflay, Chairperson of “Save the Generation Association” gives a pin to Mr Sidibé during his visit with this umbrella network of people living with HIV in Tigray. Credit: UNAIDS/Y.Gebremedhin
The Executive Director also met with the Chairman and Board Members of the “Save the Generation Association Tigray” umbrella network of people living with HIV in Tigray National Regional State. The Network promotes the rights of its members, fight stigma and assists regional efforts to scale up HIV prevention, treatment, care and support services. According to the Federal Ministry of Health an estimated 62,000 people are living with HIV in the region and 63% of those in need of HIV treatment have access to it.
Care and support of vulnerable children
Around 650,000 children have been orphaned by AIDS in Ethiopia. Mr Sidibé visited a care and support project for orphans and vulnerable children and affected families in Mekelle. The project, run by Human Being Association of Brotherhood, began in 2001 to support orphans and vulnerable children and families under difficult circumstances and today provides basic and educational support to over 1000 families caring for orphans and vulnerable children. It also provides vocational training, equipment and seed money to street children and child sex workers to enable them to have their own income and continue their education. Other support services include reuniting street children with extended families and legal support for children to inherit property and pensions of their families who died of AIDS-related illnesses.
The Ethiopian Minister of Health Dr Tedros Adhanom accompanied Mr Sidibé on these site visits.
The government of Ethiopia has set ambitious targets to achieve universal access to HIV prevention, treatment, care and support and developed a multi-sectoral Plan of Action for 2007 to 2010. This was developed in consultation with a broad range of stakeholders, who shared lessons learned during implementation of the AIDS response. The plan includes detailed activities, targets, cost estimations and a financial gap analysis and represents a major step towards the realization of the ‘Three Ones’ principles.
Right Hand Content
Multimedia:
Feature stories:
UNAIDS Executive Director visits Ethiopia (20 April 2009)
ILO: Action against stigma brings hope to Ethiopia’s agricultural cooperatives (14 April 2009)
Translating intent into action in Ethiopia (25 November 2008)
Publications:


Feature Story
Joint action for results: UNAIDS outcome framework, 2009 – 2011
22 April 2009
22 April 2009 22 April 2009
The HIV organizational landscape has evolved and grown more complex over the past decade. UNAIDS, donors and civil society, including networks of people living with HIV, have rightly demanded greater clarity on the relationships between needs, financing, activities and outcomes. Also demanded is greater specificity about the role of UNAIDS and the Secretariat within the wider constellation of actors.
This Outcome Framework, which builds upon the UNAIDS Strategic Framework (2007–2011), will guide future investment and hold the Secretariat and the Cosponsors accountable for making the resources of the UN work for results in countries. It affirms the UNAIDS Secretariat and Cosponsors to leverage our respective organizational mandates and resources to work collectively to deliver results.
Joint action for results: UNAIDS outcome framework, 2009 – 2011 (pdf, 388 Kb)
Joint action for results: UNAIDS outcome framewor
Cosponsors:
Office of the United Nations High Commissioner for Refugees (UNHCR)
United Nations Children's Fund (UNICEF)
World Food Programme (WFP)
United Nations Development Programme (UNDP)
United Nations Population Fund (UNFPA)
United Nations Office on Drugs and Crime (UNODC)
International Labour Organization (ILO)
United Nations Educational, Scientific and Cultural Organization (UNESCO)
World Health Organization (WHO)
World Bank
Publications:
Joint action for results: UNAIDS outcome framework, 2009 – 2011 (pdf, 388 Kb)