
Feature Story
OPINION: HIV and drugs: two epidemics - one combined strategy
20 April 2009
20 April 2009 20 April 2009By Michel Sidibé, Executive Director, Joint United Nations Programme on HIV/AIDS (UNAIDS) Geneva, Switzerland
(This article also appeared in the Bangkok Post on 20 April 2009)
At the Mitsamphan drug user harm reduction drop-in centre in Bangkok drug users are able to get clean needles, condoms and counselling. Access to these services allows them to stop HIV, look after their health and lead productive lives. The centre is run by community members, including ex-drug users, and has restored dignity and is giving hope to many. Thanks to many such centres worldwide, new HIV infections among drug users are being stopped. This is not a surprise for the delegates attending the 20th international conference on harm reduction in Bangkok this week. But for a majority of policy makers in national drug programmes, the term ‘harm reduction’ invokes silence and controversy. However nearly 16 million people inject drugs worldwide – 3 million of whom are estimated to be living with HIV – silence on harm reduction therefore is not an option.
National drug control and HIV programmes must work together. They must be informed by evidence and grounded in human rights. Drug issues are complex but they do not take away from the fact that people who inject drugs, just as everyone else, are entitled to the full spectrum of human rights. Evidence shows that harm reduction programmes save lives. Many countries are still not providing access to the harm reduction services. This is killing people as much as the drugs themselves.
Regrettably the 52nd session of the Commission on Narcotic Drugs in March of this year missed an occasion to make a bold political commitment to holistic harm reduction. Yet member states had committed to accelerating access to harm reduction efforts related to drug use in the Political Declaration on AIDS adopted at the UN High level meeting on AIDS in 2006.
But why are drug control authorities against harm reduction? Harm reduction programmes include access to sterile injecting equipment, opioid substitution therapies, and community-based outreach. These are the most cost effective means of reducing HIV-related risk behaviors. They not only prevent transmission of HIV but also of hepatitis C and other blood borne viruses. In Australia, the return on investment of a decade of needle and syringe programmes was estimated at one and half billion US dollars. And in Ukraine, for $0.10 cents per day one drug user can be protected against HIV through the provision of comprehensive harm reduction services.
Countries that have adopted a comprehensive approach to HIV and drug use have seen a decline in the spread of HIV among people who inject drugs. This includes Australia, United Kingdom, France, Italy, Spain, and Brazil, and in some cities in Bangladesh, the Russian Federation, and Ukraine.
We can protect drug users from becoming infected with HIV. China is doing its part. In 2004, there were only 50 needle and syringe programmes. Today there are more than a thousand such programmes in all priority provinces. By achieving universal access targets for 2010, nearly 10 million drug users will be able to access such life saving harm reduction programmes worldwide.
Harm reduction is not an obstacle in reaching the goal of a drug-free world. Drug control authorities need not fear a rise in drug use simply because people are taking steps to protect themselves from HIV and reduce their drug dependency.
There is no evidence that providing harm reduction services has led to more people becoming drug users. There is also no proof that current drug users increase their intake of drugs or choose to use them longer. In contrast to the overwhelmingly beneficial effects of harm reduction, law enforcement approaches alone do little to reduce drug use and drug-related crime and are often associated with serious human rights abuses and poor health outcomes for people who use drugs. They include arbitrary arrests, prolonged detention, compulsory drug registration and unwarranted use of force and harassment by law enforcement officers.
Many drug laws make possessing and distributing sterile needles and syringes an offence, and opioid substitutes such as methadone and buprenorphine are classified as illegal despite being on the WHO list of essential medicines.
When law enforcement and public health efforts come together, the outcomes are very successful – for example in Britain and Australia where drug action teams and police focus on crime fighting and successfully refer drug users to health and welfare services.
The Supreme Court in Indonesia rightly ruled that drug users should not be sent to prison; instead they should have access to treatment. It should not be a crime to access clean needles. It should not be a crime to access substitution therapy.
We need to get rid of drug laws that block the response to AIDS and drug use. HIV and injecting drug use are two epidemics but need a combined strategy. We cannot leave it to the next generation to reconcile the separate approaches to HIV and drug control.
Right Hand Content
Cosponsors:
Feature stories:
International Harm Reduction conference opens in Bangkok (20 April 2009)
OPINION: Silence on harm reduction not an option (11 March 2009)
51st session of the Commission on Narcotic Drugs (11 March 2008)
Reducing drug related harm (14 May 2007)
Injecting drug use: focused HIV prevention works (11 May 2007)
Harm reduction to be scaled up in Ukraine (11 April 2007)
Increased HIV services for drug users needed (14 November 2006)
External links:
Harm Reduction 2009: IHRA’s 20th International Conference
Statements:
Publications:
Best Practice Publication: High Coverage Sites—HIV Prevention among Injecting Drug Users IDU in Transitional and Developing Countries ( En | Fr | Es | Ru )



Feature Story
UNAIDS Executive Director visits Ethiopia
20 April 2009
20 April 2009 20 April 2009
Mr Michel Sidibé (left) met with HE Girma Woldegiorgis, President of the Federal Democratic Republic of Ethiopia.
Credit: UNAIDS/Y.Gebremedhin
The Executive Director of UNAIDS, Michel Sidibé is in Ethiopia to discuss ways of strengthening UN support to the AIDS response in the country.
High on the agenda will be the progress and challenges Ethiopia is facing in scaling up to universal access to HIV, prevention, treatment, care and support. These issues will be discussed in meetings with a range of stakeholders including the Ethiopian authorities, religious leaders, networks of people living with HIV, and senior officials from the African Union Commission.
Whilst in the country Mr Sidibé will also visit projects in Mekelle, a region some 800 km from the capital Addis Ababa. As well as visiting health facilities and care and support projects in the region, he will also meet with local communities to see first hand how universal access is working for people on the ground.
On the final day of the visit Mr Sidibé will meet with the press to present his vision for the future and highlight the urgent need to invigorate momentum and commitment towards achieving universal access and the need for increased investments for countries to reach their goals.
Right Hand Content
Feature stories:
ILO: Action against stigma brings hope to Ethiopia’s agricultural cooperatives (14 April 2009)
Translating intent into action in Ethiopia (25 November 2008)
Multimedia:
Related



Feature Story
International Harm Reduction conference opens in Bangkok
20 April 2009
20 April 2009 20 April 2009Delegates are gathering in Thailand’s capital this week for the 20th international conference on harm reduction running from 20 to 23 April. Organized by the International Harm Reduction Association (IHRA), the conference’s theme is human rights, underscoring the necessity of injecting drug users’ universal access to HIV prevention, treatment, care and support including comprehensive harm reduction programmes.
The four-day event will provide the harm reduction community with the opportunity to share ideas, research and best practices to further advocate for the inclusion of harm reduction in national drug – and AIDS – programmes.
The thematic link between harm reduction and human rights points to the growing understanding that drug users’ impeded access to the full harm reduction package, including clean needles and syringes, substitution therapy, condoms, HIV testing and counselling, infringes upon an individual’s right to highest attainable standard of physical and mental health, without discrimination of any kind.
Laws criminalizing the possession of injecting equipment or substitution therapy are major barriers in responding to HIV, as the fear of criminal measures and prosecution force many drug users underground.
“One of the most significant steps forward we can make to universal access to HIV prevention, treatment, care and support is to stop criminalizing use of needle exchange, methadone treatment and other substitution therapies,” said UNAIDS Executive Director, Michel Sidibé.
Lack of official support for harm reduction in many countries, laws that prohibit key components of harm reduction, and onerous regulatory schemes (e.g. strict import limits on opiate maintenance medications) often make it difficult to implement harm reduction initiatives at all, much less bring such programmes to scale.
Substitution therapy with methadone is available in only 52 countries, and with buprenorphine in only 32 countries. Substitution therapy is largely unavailable in Eastern Europe and Central Asia, where injecting drug use represents the most important mode of HIV transmission.
Important but uneven advances in access to harm reduction
Studies have consistently demonstrated that harm reduction services reduces HIV infections and risk behaviours without contributing to increased drug use or increasing other harms in the communities in which such programmes operate.
Experience in diverse regions has demonstrated the feasibility of bringing harm-reduction programmes to scale, even in the face of official resistance. Common features of high-coverage programmes for injecting drug users include involvement of community organizations, work with law enforcement agencies to minimize harassment, adequate and sustained funding, ease of access for clients, and involvement of injecting drug users in advisory bodies and other appropriate structures.
Recent years have seen important but uneven advances in access to harm reduction in various settings. China, for example, has expanded key components of harm reduction, reaching more than 88 000 individuals with methadone maintenance therapy, and by the end of 2008, establishing 1109 needle exchange programmes in 27 provinces. Viet Nam initiated its first pilot project of methadone substitution therapy in 2008, and harm reduction programmes in the country distributed 15 million condoms and 7.5 million needles and syringes in the first 10 months of 2007. In 2006, Bulgaria, Estonia, Finland, Latvia, and Lithuania created a regional network to expand and coordinate HIV prevention services for injecting drug users, with financing secured until 2009 from the European Commission. In Thailand, by contrast, a recent report by civil society informants found little expansion of harm reduction programmes, despite the national government’s widely publicized 2004 commitment to increase prevention access for drug users.
Aggressive drug control policies often inhibit use of harm-reduction programmes, underscoring the need for inter-ministerial collaboration between Ministries of Health, Interior and Justice and sensitization of law enforcement personnel, to avoid approaches that can deter participation in prevention programmes.
In most countries in Eastern Europe and Central Asia, for example, police sometimes make arrests for possession of extremely small amounts of narcotics, potentially discouraging drug users from participating in needle exchange projects. According to Georgia’s official report to UNAIDS on UNGASS indicators, the national anti-drug policy climate has inhibited efforts to offer even minimal access to detoxification and drug rehabilitation services. In Thailand in 2003, the alleged extrajudicial killings and associated violence, which resulted in the death of more than 2000 suspected drug dealers and users, continues to reverberate through society. Civil society informants report that injecting drug users are afraid to access harm reduction and other health services.
In contrast to the overwhelmingly beneficial effects of harm reduction, law enforcement approaches alone do little to reduce drug use and drug-related crime and are often associated with serious human rights abuses and poor health outcomes for people who use drugs.
When law enforcement and public health efforts come together, the outcomes are very successful. For example in Britain and Australia where drug action teams and police focus on crime fighting and successfully refer drug users to health and welfare services. In Australia, the return on investment of a decade of needle and syringe programmes was estimated at one and half billion US dollars. Furthermore, the Supreme Court in Indonesia ruled that drug users should not be sent to prison; instead they should have access to treatment.
The global drug problem is complex and cannot be solved in isolation. A coming together of organizations working on drug control and AIDS is urgently needed. HIV and injecting drug use are two epidemics but need a combined strategy.
Right Hand Content
Cosponsors:
Feature stories:
OPINION: HIV and drugs: two epidemics—one combined strategy (20 April 2009)
OPINION: Silence on harm reduction not an option (11 March 2009)
51st session of the Commission on Narcotic Drugs (11 March 2008)
Reducing drug related harm (14 May 2007)
Injecting drug use: focused HIV prevention works (11 May 2007)
Harm reduction to be scaled up in Ukraine (11 April 2007)
Increased HIV services for drug users needed (14 November 2006)
External links:
Harm Reduction 2009: IHRA’s 20th International Conference
Statements:
Publications:
Best Practice Publication: High Coverage Sites—HIV Prevention among Injecting Drug Users IDU in Transitional and Developing Countries ( En | Fr | Es | Ru )
Feature Story
UNICEF working to teach AIDS prevention to young people in Guinea
16 April 2009
16 April 2009 16 April 2009A version of this story was first published on UNICEF.org

Fatoumata in a salon in a poor Koloma neighbourhood of Conakry. She is 18, has two children, aged six and three, and has never heard of AIDS. Credit: UNICEF Guinea/2009/Baro
Nene Gallé Barry sells charcoal in a very poor area of the Koloma quarter in Conakry, Guinea’s capital. She is 18 now, but left her home village four years ago to earn a living in the city. She has a boyfriend and is sexually active and, until recently, she had never heard of AIDS and had never seen or used a condom.
This is the reality for many adolescents in Guinea. Adolescents often lack access to information that will protect them from sexually transmitted infections (STIs), including HIV. According to a recent UNAIDS/WHO/UNICEF report, in 2007 only 12% of females aged 15 to 24 had correct knowledge of, and rejected myths about, sexual transmission of the virus. In addition, just under a quarter of adolescents aged 15 to 17 used condoms during sexual intercourse, according to a 2005 study.
When Nene finally learned about the risks she had been taking by not using protection, she asked for condoms. She wanted to know how to use them and how to convince her partner to wear them and was very pleased when she’d learned what to do.
Improving youth access to information
In Guinea girls are particularly at risk of contracting STIs. According to the UNAIDS/WHO/UNICEF 2008 report, 31% of girls have had sexual intercourse before the age of 15. (For boys, the figure is 20%). The publication also confirms that girls and women in the 15 to 24 age group are twice more likely to be infected with HIV than their male counterparts.

A group of peer educators enter
a hair salon in Miniere, Conakry.
Credit: UNICEF
Guinea/2009/Baro
A high number of young women are involved in jobs that expose them to unsafe sexual practices; jobs such as selling fruit on the streets or working in hair and sewing salons. In these settings they often meet male adolescents or older men who offer money in exchange for sex.
UNICEF and its national partners have taken major steps to improve youth access to information and informed decision making concerning HIV. The first national prevention strategy for youth was produced in 2007, and a coordinating team has been set up in order to coordinate and scale up activities. For the past two years UNICEF has partnered with JCI (Junior Chamber International) to empower adolescents within poor communities and involve them in projects that reach other vulnerable adolescents, mostly girls.
'My job, my health'
From 2007 to 2008 the programme reached more than 20,000 adolescents ranging in age from 13 to 20, all from different backgrounds. Eight TV spots in four different languages were produced, as well as 20 interactive radio shows.
The newest project is called 'mon MÉtier, ma santé' ('my job, my health'), and aims to reach girls working in hair dressing and tailoring shops in two of the poorest neighbourhoods in Conakry. One hundred peer educators are planning to visit the selected sites and help educate young apprentices and clients about HIV prevention.
It is hoped that once the young girls have received the information about HIV prevention will then reach out to their family members and friends. A study will be conducted after two months of such sensitization activities to evaluate the impact of the project. UNICEF hopes to be able to reach at least 50 per cent of the most vulnerable girls by 2011.
Right Hand Content
Key populations:
Young people
Women and girls
Condoms
HIV prevention
Cosponsors:
Partners:
Junior Chamber International (JCI)
Feature stories:
Barber Shops and Beauty Salons promote HIV education in Guyana (26 March 2009)
Condoms and HIV prevention: Position statement by UNAIDS, UNFPA and WHO (19 March 2009)
Costa Rica: Peer HIV prevention programmes to be promoted for young people (03 March 2009)
Publications:
Best practice: Making condoms work for HIV prevention (pdf, 1.1 Mb)
UNAIDS action plan on intensifying HIV prevention (pdf, 1.71 Mb)



Feature Story
ILO: Action against stigma brings hope to Ethiopia’s agricultural cooperatives
14 April 2009
14 April 2009 14 April 2009
Ajama Kalacha gets ready to plough his field. His community’s support has made it easier for him to cope with HIV Credit: ILO
Ajama Kalacha works hard on his small agricultural plot in Ethiopia’s highlands to provide an income for the extended family he supports. Even though life is tough, Ajama is an optimist - his community treats him well and he believes his prospects for making a living from the land are good. But he was not always so confident.
Seven years ago, Ajama discovered that he had become infected with HIV. At the time stigma and discrimination were widespread in his community and the diagnosis led him to despair. Today Ajama is taking antiretroviral treatment and his health is stable. He has told everyone about his HIV status, and his children and extended family have not been excluded from school or community life as he had once feared.
“My message to others is that living positively with HIV helps you to work harder and leads to a new lifestyle,” he says. “The care and support that I have received has made it much easier for me to cope with my illness.”
This dramatic change in Ajama’s attitude and circumstances came about in 2004 when his agricultural cooperative society in West Oromia State became part of a wider programme to reduce the negative effects of HIV. Funded by the Italian government in cooperation with the International Labour Organization (ILO), the programme works through the Oromia region agricultural cooperative unions that have members in over 200 agricultural primary societies and 14 transport associations.
To ensure that interventions were at the right level, staff carried out an initial study of HIV knowledge and attitudes, which revealed many misunderstandings. For instance, 51 per cent of those interviewed thought HIV could be transmitted by mosquito bites, 17 per cent by sharing a toilet and 6 per cent by working with an HIV-positive person.
The programme has strong support from government and the national cooperative leadership. It works through a range of training approaches, firstly raising awareness of HIV among leaders and then, through specific workshops, training a network of master trainers and peer educators. They in turn roll out the programme at community level, helping to challenge discrimination, change behaviour which may risk exposure to HIV, and set up care and support services for members and their families.
Easily identified by their bags and T-shirts that both bear the slogan, ‘HIV does not discriminate, but people do,’ the peer educators work with the whole community visiting homes, speaking at local gatherings and involving key individuals such as religious leaders. They use an HIV manual and distribute popular information materials that have been translated into the local languages of Afaan Oromo and Amharic. They also help to provide care and support services including treatment.
In Ajama’s cooperative, misunderstandings about HIV, together with the stigma and discrimination directed against those affected, have gradually reduced as a result of this steady work. The positive environment and encouragement he has received gave Ajama the courage to speak out about his status and to have hope for the future.
“I set my mind to starting a new life,” he says. “The care and support for people living with HIV and AIDS has helped greatly to reduce its impact on our lives.”
Right Hand Content
Cosponsors:
Feature stories:
Faces against HIV stigma and discrimination (01 October 2008)
International labour standard would strengthen the HIV response in the workplace (21 July 2008)
ILO sees significant improvement in workplace attitudes to HIV (25 April 2008)
Making a difference: UNAIDS in Ethiopia (08 February 2008)
Publications:
Saving lives, protecting jobs. SHARE Report ( pdf, 3.7 Mb.) ( fr )
ILO Code of Practice on HIV in the workplace
Reducing HIV stigma and discrimination: a critical part of national AIDS programmes (pdf, 598 kb.)
AIDS is everybody's business: partnerships with the private sector (pdf, 1 Mb.)
Greater involvement of people living with HIV (GIPA) (pdf, 245 kb.)
Facts sheets on ILO work and partnerships in Africa:
Ethiopia
Benin ( Fr )
Botswana
Burkina Faso ( Fr )
Ghana
Lesotho
Malawi
Mozambique
South Africa
Swaziland
Togo ( Fr )
Zambia
Zimbabwe

Feature Story
Leadership in Senegal’s AIDS response
09 April 2009
09 April 2009 09 April 2009
Michel Sidibé UNAIDS Executive Director and representatives from national civil society organizations and regional networks of people living with HIV after their meeting at SIDA Service, 9 April 2009.
Credit: UNAIDS/C.Diop
UNAIDS estimates that one per cent of adults in Senegal are living with HIV. In 1992, at a time when the full impact of AIDS on society was only beginning to be recognised in the country, the Catholic church in Senegal founded “SIDA Service,” an organization to support and care for people living with or affected by HIV.
Since those early days, and continuing today, it actively seeks to change peoples’ attitudes of stigma towards, and discrimination against, people living with HIV.
SIDA Service has grown to 500 volunteers and employees with 23 branches across Senegal as well as a presence in neighbouring Guinea Bissau and Gambia. Its Dakar health centre was the first in the country to offer HIV testing that is free, voluntary and confidential. In addition to voluntary counselling and testing and support to people living with HIV, SIDA Service also cares for orphans and vulnerable children.
While in Senegal this week, UNAIDS Executive Director Michel Sidibé visited the SIDA Service’s health centre which is making a significant the contribution towards Senegal’s goal of universal access to HIV treatment, prevention, care and support. His visit took place on Wednesday 8 April where he had an opportunity to listen to those who use the services.
The medical team at the centre offer a range of services to the local community including HIV treatment, treatment of opportunistic infections, gynaecological health and pre-natal services. There is a laboratory for biomedical analysis and an on-site pharmacy. In addition to health care, food support is available and staff and volunteers offer time to listen as well as give counselling, psycho-social support and spiritual care to any in need.
SIDA Service has also led in promoting dialogue within faith communities on AIDS. It has co-organized a number of important conferences and gatherings of religious communities on AIDS in Africa and was a founding member of the National Alliance of Religious and Medical Experts against AIDS in 1999.
Mr Sidibé also met with civil society leaders in Senegal as well as from wider the West Africa region.
President Abdoulaye Wade

President Abdoulaye Wade of Senegal (front right) hosted a meeting with Michel Sidibé UNAIDS Executive Director. Also present were (from left) Dr Meskerem Grunitzky Bekele, Director, UNAIDS Regional Support Team for West and Central Africa; and United Nations Resident Coordinator Mr Bouri Jean Victor Sanhouidi.
Credit: UNAIDS/C.Diop
Later on Wednesday Mr Michel Sidibé met with Senegal’s President Abdoulaye Wade where they discussed Senegal’s progress in the national AIDS response. The country has made good progress in access to HIV treatment in recent years with 56 per cent of people in need of HIV treatment accessing it in 2007, up from 26 per cent in 2004.
Mr Sidibé also met with the Senegalese Minister of Health Dr Safiatou Thiam.
Regional Dialogue on Universal Access in West and Central Africa
On Thursday, Mr Sidibé opened a Regional Dialogue on Universal Access in West and Central Africa.
The Dialogue was chaired by Dr Thiam and brought together senior government and UN officials, civil society from across West and Central Africa including representatives from networks of people living with HIV, representatives from donor countries and the Global Fund.
Addressing the gathering Mr Sidibé urged participants to work together to achieve universal access which he said “is more than a motto but a way to bring about fundamental transformation.”
He called for AIDS to remain a political priority of governments in the region and emphasized the need for an expansion of HIV prevention efforts. Expanded partnerships including with the women’s movement, TB community, others working on development goals, are key to the strategy of universal access he proposed. Mr sidibé also called for respect for human rights: “I ask the UN system, governments and civil society to come together to build a response to HIV that does not drive people underground through fear of the criminal law”.
Dr Luis Gomes Sambo, Regional Director for Africa, WHO; Mr Jean-Christophe Deberre, Deputy Regional Director for West and Central Africa, UNDP; and Dr Meskerem Grunitzky Bekele, Director, UNAIDS Regional Support Team for West and Central Africa also spoke.
Mr Sidibé will conclude his visit later today by meeting with the First Lady of Senegal, Ms Viviane Wade who is a long term advocate on AIDS and health issues in her country and an active member of Organization of African First Ladies against HIV/AIDS.
Right hand copntent
Feature stories:
ICASA 2008 3-7 December 2008 (07 December 2008)
Understanding HIV transmission for an improved AIDS response in West Africa (03 December 2008)
Press centre:
UNAIDS and broad coalition working towards the release of nine men who have sex with men in Senegal who have been convicted and imprisoned (15 January 2009
Multimedia:
External links:
Organisation of African First Ladies against HIV/AIDS
Publications:
Senegal 2008 UNGASS Country Progress Report (French only)
The Alliance of religious and medical experts in the response to the AIDS epidemic in Senegal. The medical, coranic and biblical principles that every religious believer should read, know and apply (pdf, 365 Kb) (in French)



Feature Story
New policy brief on disability and HIV
08 April 2009
08 April 2009 08 April 2009
The new policy brief explores the links between HIV and disability and makes recommendations for policy change.
Credit: WHO/Asis Senyal
An estimated 650 million people, or 10% of the world’s population, have a disability. Although people with disabilities are found within the populations at higher risk of exposure to HIV, not much attention has been paid to the relationship between HIV and disability.
For this reason, the Joint United Nations Programme on HIV/AIDS (UNAIDS), the World Health Organization (WHO) and the United Nations Office of the High Commissioner for Human Rights (UNOHCHR) have collaborated on a policy brief that explores the links between HIV and disability and makes recommendations for policy change.
This policy brief discusses the actions needed to increase the participation of persons with disabilities in the HIV response and ensure they have access to HIV services which are both tailored to their diverse needs and equal to the services available to others in the community.
Evidence shows that people with disabilities are at the same or greater risk of HIV infection as non-disabled people. Due to insufficient access to appropriate HIV prevention and support services, persons with disabilities may engage in behaviours which place them at risk of HIV infection, such as unprotected heterosexual or male-to-male sex (including in the context of sex work) and injecting drug use.
The policy brief states that a large percentage of persons with disabilities experience sexual assault or abuse during their lifetime, with women and girls, persons with intellectual impairments and those in specialized institutions, schools or hospitals being at particularly high risk. There is also evidence that in some cultures, persons with disabilities are raped in the belief that this will “cure” an HIV-positive individual.
Persons with disabilities may not benefit fully from HIV and related sexual and reproductive health services because services offered at clinics, hospitals and in other locations may be physically inaccessible, lack sign language facilities or fail to provide information in alternative formats such as Braille, audio or plain language. Also, service providers may lack knowledge about disability issues, or have misinformed or stigmatizing attitudes towards persons with disabilities.
As stated in the 2006 Convention on the Rights of Persons with Disabilities, persons with disabilities have the right to participate in decisions which affect their lives, and should be fully involved in the design, implementation and evaluation of HIV policies and programmes. This is the best way of ensuring these policies and programmes are responsive to their needs.
The policy brief on Disability and HIV calls for HIV services to be inclusive of persons with disabilities. It makes recommendations to governments, civil society and international agencies to eliminate physical, information and communication, economic and attitudinal barriers not only to increases access to HIV programmes, but to assist people in accessing broader health and social services.
Right HAnd Content
Cosponsors:
Feature stories:
Disability and HIV in Jamaica (08 September 2008)
Publications:
Policy brief: Disability and HIV (pdf, 207 Kb)
Related

 Towards a life of dignity for people living with disabilities
Towards a life of dignity for people living with disabilities
15 February 2022

Feature Story
UNAIDS Committee of Cosponsoring Organizations meet
06 April 2009
06 April 2009 06 April 2009
(from left): Joy Phumaphi, Vice President and Head of the Human Development Network, World Bank; Arnauld Akodjenou, Director, Division of Operational Services, UNHCR; Josette Sheeran, Executive Director, WFP; Anarfi Asamoa-Baah, Deputy Director General, WHO; Assane Diop, Executive Director, Social Protection Sector, ILO; Koichiro Matsuura, Director General, UNESCO; Ad Melkert, Administrator ad-interim, UNDP; Ann M. Veneman, Executive Director, UNICEF; Michel Sidibé, Executive Director, UNAIDS; Thoraya Ahmed Obaid, Executive Director, UNFPA; Antonio Maria Costa, Executive Director, UNODC. Paris, 3 April 2009,
The Joint United Nations Programme on HIV/AIDS (UNAIDS) brings together the efforts and resources of ten UN system organizations in the AIDS response. The UNAIDS Committee of Cosponsoring Organizations (CCO) serves as the forum for these Cosponsors to meet on a regular basis to consider matters of major importance to UNAIDS, and to provide input from the Cosponsoring organizations into the policies and strategies of UNAIDS.
On 3 April 2009, the CCO held their first meeting since the appointment of UNAIDS Executive Director Michel Sidibé.
The CCO expressed their full support for “universal access” which Mr Sidibé has outlined as the top priority for UNAIDS as well as the other priority areas of focus which will be set out in the new UNAIDS outcome framework currently being finalized with Cosponsors.
The meeting provided an excellent opportunity to share ideas on supporting countries in achieving their universal access goals. The need for UNAIDS to advocate for an evidence informed AIDS response that is grounded in human rights was accepted by all. Equally important was the need for accountability and results.
The CCO also endorsed the general directions of the 2010-2011 Unified Budget and Workplan including the key priorities and the allocation of resources between the Cosponsors, the Secretariat and Interagency activities. The Secretariat will now work with the Global Coordinators of the Cosponsors to finalize the UBW for the June 2009 meeting of the Programme Coordinating Board.
UNAIDS Committee of Cosponsoring Organizations (CCO)
The CCO comprises representatives from the ten UNAIDS Cosponsors and the UNAIDS Secretariat. It meets twice a year and each Cosponsor rotates as chair of the committee annually, on 1 July.
Right Hand Side
Cosponsors:
Office of the United Nations High Commissioner for Refugees (UNHCR)
United Nations Children's Fund (UNICEF)
World Food Programme (WFP)
United Nations Development Programme (UNDP)
United Nations Population Fund (UNFPA)
United Nations Office on Drugs and Crime (UNODC)
International Labour Organization (ILO)
United Nations Educational, Scientific and Cultural Organization (UNESCO)
World Health Organization (WHO)
World Bank
Related
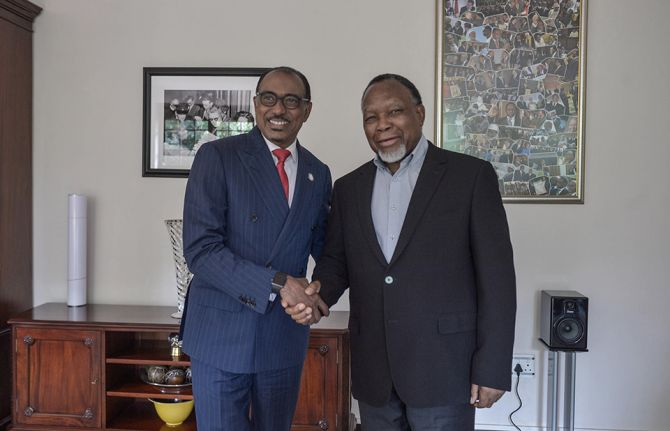 Keeping up the momentum in the global AIDS response
Keeping up the momentum in the global AIDS response
24 April 2019
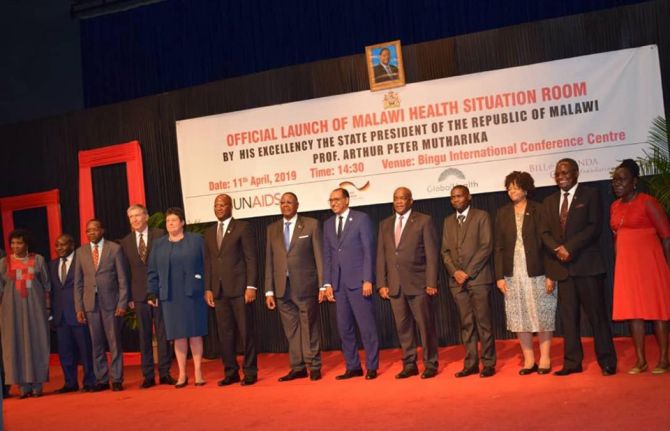 Malawi launches its health situation room
Malawi launches its health situation room
12 April 2019
 Learning lessons on evaluation
Learning lessons on evaluation
02 April 2019
Feature Story
‘Love and Relationships’: Film festival in Cambodia addresses HIV prevention
06 April 2009
06 April 2009 06 April 2009A version of this story was first published on UNESCO.org

‘The cinema road’ crosses Cambodian provinces. Credit: CCF
Last month audiences in selected Cambodian provinces had the chance to see the Khmer film Palace of Dreams as part of the ‘Love and Relationships’ film festival sponsored by UNESCO in cooperation with the French Cultural Centre (CCF). This drama, produced in 2008 by BBC World Service Trust, aims at reducing the risk of HIV infection transmission among young people.
Palace of Dreams is a powerful 90 minute feature about young people and their relationships. It aims to entertain and encourage the target audience to adopt behaviours that will reduce their risk of HIV infection and transmission. The drama was screened in 11 Cambodian provinces by the end of March.
Although HIV rates are on the decline in Cambodia, there is no room for complacency, especially for young people, as infection rates are highest among under 24-year-olds. Some specific groups are especially in need of HIV prevention information and are a particular focus within the film:
- out-of-school youth, including the 47% that work for a living, often far from home;
- young people in a relationship who say they trust their partner and do not use condoms;
- female entertainment workers;
- men who have sex with men, who have an HIV prevalence of 5.1%, which is more than five times higher than the national average.

Installation of the equipment for the evening screening. Credit: UNESCO
Since March 2008 ‘The Cinema Road’ project (La Route du Cinema), organized by the French Cultural Centre, has shown, free of charge, several movies in 15 different provinces of Cambodia and has reached more than 30,000 viewers.
In November 2008 UNESCO’s office in Phnom Penh joined CCF in the ‘Love and Relationships’ programme, which aims to reach the maximum number of people in Cambodia and highlights challenges that the young face in intimate relationships. It focuses particularly on HIV prevention, sexuality and discrimination based on gender and/or sexual orientation; topics that formal education has been reluctant to address explicitly.
For this joint project, CCF selects French films (mostly comedies) translated into Khmer while UNESCO chooses films related to the above-mentioned subjects. Each month one movie from CCF and one from UNESCO are screened in a selected province.

Entire families attend an open-air screening. Credit: UNESCO
The screenings follow a set pattern. The CCF projectionist arrives in the province at noon and tours the town, announcing the event and inviting people to attend the show in the evening. A local NGO, responsible for distribution, organizes a prior sensitisation of the public and technical arrangements are made with the help of local people.
Entire families and groups of friends attend the open-air screening, which takes place in a workshop environment, accompanied by a facilitated discussion. When the film is finished the projectionist takes his camera and interviews young people from the audience, asking them questions related to the drama.
The project has been very well received by the public. The two movies that have drawn the greatest positive reaction are Palace of Dreams, being screened currently, and In the Dark, shown in November 2008.
Right Side Content
Cosponsors:
Partners:
French Cultural Centre, Cambodia (Centre Culturel Francais, Cambodge)
BBC World Service Trust
Feature stories:
Love in a Time of HIV (19 December 2008)
Powerful film brings AIDS issues to communities in Democratic Republic of Congo (16 June 2008)
Multimedia:
Publications:
Art for AIDS (pdf, 2.12 Mb)
UNAIDS Expert Consultation on Behaviour Change (pdf, 1.29 Mb)
Related
Feature Story
Call for global action on the threat of drug-resistant tuberculosis
03 April 2009
03 April 2009 03 April 2009
Dr. Bernhard Schwartländer, UNAIDS Country Director for China, chaired a session on TB/HIV at the meeting.
Ministers from the 27 countries with the highest burden of multi-drug resistant and extensively drug-resistant tuberculosis (M/XDR-TB) have jointly endorsed a Call for Action on TB control and care to urgently address this alarming threat. The meeting in Beijing, China, on 1-3 April 2009, was organized by the World Health Organization (WHO), the Ministry of Health of the People's Republic of China and the Bill & Melinda Gates Foundation.
The two main aims of the meeting were to build consensus and political commitment globally and in countries with high levels of M/XDR-TB, and to act immediately to scale up the prevention and management of drug resistant tuberculosis. This will include developing five year national strategic plans, embedded within national TB and health sector plans.
The Call for Action, endorsed on the first day, recognizes the serious threat that this type of TB poses to people living with HIV and draws attention to the actions required to scale-up M/XDR-TB prevention, control and care. Countries are asked to identify the groups most vulnerable to, and at risk of, drug resistant TB and its impact, including people living with the virus, drug users, prisoners, migrant populations and other marginalized groups and to ensure that services to prevent and treat M/XDR-TB are targeted to meet their needs.
Among the recommendations was a call for governments and partners to strengthen efforts to mobilize more funding to finance care and control of the diseases and increase investments in the research and development of new TB diagnostics, medicines and vaccines effective in people living with HIV.
Drug resistant TB and HIV
The 33 million people living with HIV around the world are especially vulnerable to the impact of M/XDR-TB, a drug-resistant form of tuberculosis. They are at increased risk of contracting such types of TB and experiencing serious side effects and drug interactions when second-line drugs are taken with antiretroviral therapy. They are also at much higher risk of dying if affected by M/XDR-TB.
During a session chaired by UNAIDS Country Director for China, Dr Bernhard Schwartländer, the meeting discussed in detail how to strengthen TB/HIV collaboration. Participants agreed that the HIV community has to take greater responsibility for preventing, diagnosing and treating TB among people living with HIV. Michel Sidibe, Executive Director of UNAIDS, has recently stressed UNAIDS commitment and has made ‘stopping people living with HIV from dying of TB’ an organizational priority.
In line with this, Dr Brad Hersh of the WHO HIV/AIDS department stressed the need for TB and HIV programmes to work more closely together to gain efficiencies in these times of economic crisis. Better TB/HIV collaboration has the additional advantage of helping to overcome common health system barriers to successful programme implementation such as laboratory strengthening, quality assured drug supplies, and monitoring and evaluation.
Cindy Kelemi from the Botswana Network on Ethics, Law and HIV/AIDS (BONELA) urged participants to ensure that investment in HIV prevention, treatment and care was not cut as a result of the economic downturn as this would worsen the epidemic of drug resistant TB.
Affected communities are a highly valuable resource in the response and should be engaged in the planning, implementation and monitoring of activities to control and treat M/XDR-TB. Such a participatory approach is also critical in addressing the rising stigma and discrimination around TB, and to further protect the human rights of individuals affected by the disease. This need for community involvement and inclusion of people affected by TB was highlighted by South Africa’s Minister of Health, Ms Barbara Hogan.
More information about the meeting and the Call for Action can be accessed at http://www.who.int/tb_beijingmeeting/en/index.html
Note: Multi-drug resistant TB (MDR-TB) is tuberculosis that is resistant to at least Rifampicin and Isoniazid, the two most powerful anti-tuberculosis drugs. Extensively drug- resistant TB (XDR-TB) is MDR-TB that is also resistant to at least two out of the three classes of second line TB medicines.
Right Side Content
Cosponsors:
Partners:
Bill and Melinda Gates Foundation
Stop TB Partnership
Botswana Network on Ethics, Law and HIV/AIDS (BONELA)
Feature stories:
Call for fully funded Global Fund to fight AIDS, Tuberculosis and Malaria (31 March 2009)
UNAIDS Executive Director meets with TB Programme Managers, TB civil society (26 March 2009)
Need for scale up in integrated TB and HIV screening to address linked epidemics (24 March 2009)
ICASA 2008: Collaborative TB and HIV activities essential (03 December 2008)
World Lung Health experts discuss TB and HIV (15 October 2008)
TB deaths rise in people living with HIV (17 March 2008)
MDR-TB more common in people living with HIV (28 February 2008)