

Feature Story
A powerful voice for the AIDS response
25 June 2019
25 June 2019 25 June 2019In September 2018, on the sidelines of the Forum on China-Africa Cooperation (FOCAC) summit in Beijing, China’s First Lady, Professor Peng Liyuan, and her fellow First Ladies from Africa lit up a Reb Ribbon at the centre of the meeting hall, officially launching the Joint Initiative of the China-Africa Thematic Meeting on HIV/AIDS Prevention and Control.
The 2018 FOCAC summit gathered together over 20 African Heads of State and First Ladies to discuss closer partnership between China and African countries, including on health-related matters. During the thematic meeting, Professor Peng announced a three-year HIV prevention campaign among adolescents to begin in 2019 as well as a community health promotion programme involving China, several African countries and international organizations, including UNAIDS.
For more than 10 years, Professsor Peng has had a particular interest in reducing the impact of HIV among children and adolescents, especially among children orphaned by AIDS. In 2016, she hosted the China-Africa Children Summer Camp that brought together children living with or affected by HIV from China, Ghana, South Africa and Zimbabwe. During the camp, the First Lady helped launch the Chinese version of the Bravest Boy I Know, a book which helps children understand the issues surrounding HIV and reduce the stigma and discrimination faced by children affected by the virus.
In 2015, Professor Peng attended a meeting of the Organization of African First Ladies against HIV/AIDS (OAFLA) in Johannesburg, South Africa, where she underlined the importance of four key issues critical to ending AIDS by 2030: universal access to HIV treatment; public information and education; educational opportunities for adolescents and economic development to eliminate poverty.
Together with national Red Ribbon Ambassadors, Professor Peng has for many years visited communities across China, including schools and universities, to raise awareness about HIV prevention and to reduce the stigma and discrimination associated with the virus.
An acclaimed soprano singer, Professor Peng has proven to be a powerful voice for those living with or affected by HIV.
She has been a World Health Organization Goodwill Ambassador for Tuberculosis and HIV/AIDS since 2011. In 2017, she was awarded a UNAIDS Award for Outstanding Achievement in recognition of her contribution to the response.
“A caring heart is our best weapon against AIDS,” she said in accepting the award. “We can save lives if we take action. We must succeed and we will succeed.”




Feature Story
Virtual communities power HIV services in China
21 June 2019
21 June 2019 21 June 2019According to national estimates, an estimated 1.25 million people are living with HIV in China, with almost 400 000 unaware of their status. China’s epidemic is concentrated among key populations at higher risk of HIV, including men who have sex with men. That’s why it’s crucial to meet these communities where they socialize, including in virtual spaces such as gay dating applications.
Danlan Public Welfare is a nongovernmental organization that advocates for lesbian, gay, bisexual and transgender rights. It is also behind the largest gay dating application in China, Blued, which today has more than 28 million users. It has incorporated community-driven HIV prevention messaging into the application and includes basic facts about the virus, as well as information on prevention, testing and treatment options and how and where to contact related services. Interactive quizzes test users’ knowledge about HIV.
As well as this powerful virtual tool, Danlan also operates free HIV rapid testing outreach projects in partnership with the Municipal Centres for Disease Control and Prevention. People can take a free HIV test and get their results in just 10 to 15 minutes.
As the Blued dating application becomes popular around the world, Danlan is extending its HIV prevention programme to Belt and Road Countries. Since March 2019, users in Indonesia have been able to access the “Blued Help Center". The service is provided in cooperation with a local civil society organization called "VictoryPlus”, which allows users to post their concerns regarding HIV-related issues and receive an immediate answer. Blued’s “We Care” programme also offers virtual information on HIV services close by.
In Thailand, Danlan worked together with a civil organization called "Impulse" to advocate for HIV prevention programmes and provided free rapid HIV testing services. Danlan has also cooperated with Mahidol University on HIV-related risk behaviour research.
In April 2019, the chief executive officer of Danlan, Geng Le, received an award for “Outstanding Innovative Model” by the Confederation of Trade Unions of Chaoyang, Beijing. It is estimated that community-based organizations like Danlan are responsible for finding 30% of all new HIV cases in the city.
“We are doing our best to use science and technology to improve the lives of lesbian, gay, bisexual and transgender communities, including their health,” says Geng Le. “Our vision is that all young people should be able to live with dignity, be free of stigma and discrimination and love who they want to no matter where they come from, what their sexual orientation is and what their HIV status is.”
Blued is more than just a dating application now. It is also a virtual healthcare resource centre that provides support to the wellbeing of the LGBT community.






Feature Story
HIV prevention for all at the 2nd European Games 2019 in Minsk
24 June 2019
24 June 2019 24 June 2019At the 2nd European Games 2019 taking place in Minsk, Belarus, athletes and spectators are receiving information about HIV, free access to condoms and the possibility of taking a free rapid HIV test.
Thanks to a partnership between UNAIDS, the directorate of the games, the ministry of health of Belarus, the parliament of Belarus, civil society organizations and the United Nations country team, Zero Discrimination zones offering HIV services have been established throughout the site hosting the games.
The main #zerodiscrimination pavilion was opened by the UNAIDS Ambassador for the European Games, Alexei Yagudin, the world champion figure skater and olympic gold medallist.
“The 2nd European Games are free from discrimination for everyone – regardless of your nationality, age, gender, sexual orientation or HIV status,” said Mr. Yagudin.
The UNAIDS Zero Discrimination zones are placed around the official fan zone, the main sports stadium and in the athletes’ village. The zones are staffed by more than 90 dedicated volunteers, mostly doctors and nurses, who provide HIV information, HIV counselling and rapid testing and access to free condoms. Ahead of the games, UNAIDS had also provided extensive training on HIV and sexual and reproductive health to hundreds of volunteers.
In addition, the national TV Channel ONT, in close collaboration with UNAIDS, produced two public service announcements on zero discrimination and equal opportunity for all. They have been broadcast in more than 20 public venues in Minsk, on all national TV channels and during live broadcasts of the games.
Carrying the official torch of the games, the “Flame of Peace”, UNAIDS regional director Vinay Saldanha said “I am proud to carry this Flame of Peace on behalf of UNAIDS and on behalf of people who deserve to live free from discrimination, including people living with HIV that are competing in and visiting these games in Minsk.”
The 2nd European Games opened officially on 21 June and will continue until 30 June. More than 4000 athletes from 50 countries are participating in the Games, competing in 15 sports across 23 disciplines, 8 of which will also serve as qualifying events for the Olympics Games 2020 in Tokyo.
Region/country




Feature Story
Botswana enters new phase of AIDS response
20 June 2019
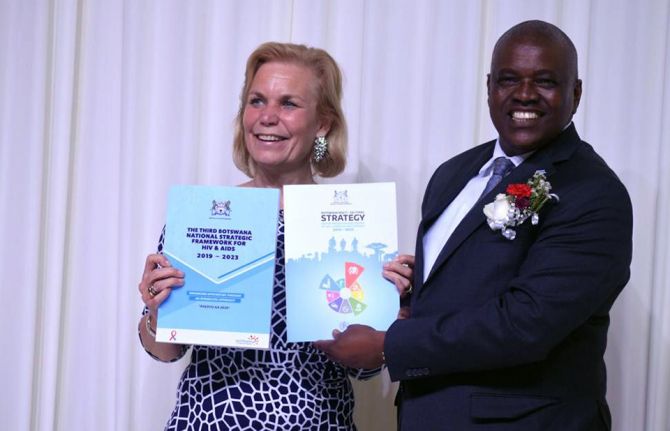
20 June 2019 20 June 2019Botswana has reaffirmed its commitment to end the AIDS epidemic as a public health threat by 2030 with the recent launch of two new five-year strategies.
The third National Strategic Framework for HIV/AIDS and the Multi-sectoral Strategy for the Prevention of Non-communicable Diseases will until 2023 guide the government’s strategic response to improve health outcomes for the country’s population.
Botswana has made significant progress in its response to the HIV epidemic in recent years. Of the estimated 380 000 people living with HIV in 2017, 320 000 have access to treatment to keep them well.
Botswana was the first country in eastern and southern Africa to provide free and universal treatment to people living with HIV. It has adopted the Option B+ strategy which offers women living with HIV lifelong treatment and the “test and treat” strategy which provides immediate treatment to people who test positive for the virus.
During a two-day visit to the country from 13 to 14 June, UNAIDS Executive Director a.i., Gunilla Carlsson, attended the presidential launch of the new health strategies.
“As a country, we need to renew our focus and re-prioritize our agenda on the HIV response to attain the 2020 targets and the vision for ending AIDS as a public health threat by 2030. Furthermore, non-communicable diseases have become a new epidemic that threatens our health as a nation as well as our national development agenda,” said President Mokgweetsi Masisi during the launch.
During her visit, Ms Carlsson also named the First Lady of Botswana, Ms Neo Masisi, as Special Ambassador for the Empowerment and Engagement of Young People in Botswana. In this role, Ms Masisi will focus on advocating for young people’s needs, the promotion and protection of their rights, and their leadership roles of agents as change, with an emphasis on young women and girls.
“I’d like to thank UNAIDS for the confidence placed in me by conferring upon me this role. It will help me to leverage my role as First Lady to end the AIDS epidemic among young people and add value to the work I am already doing,” said Ms Masisi.
In a meeting between Ms Carlsson and members of civil society in Botswana, participants raised their concerns about complacency, especially among younger people, adherence to treatment and HIV prevention.
On the back of the landmark decision of the High Court of Botswana to decriminalize same-sex relations, members of the LGBT community expressed hope, but also warned that more work needed to be done to address stigma and discrimination, especially in communities and in health care settings.
“The main challenge that Botswana is facing in its AIDS response is complacency. If the country can overcome this challenge, then it will show the whole world that it can be done,” said Gunilla Carlsson, UNAIDS Executive Director, a.i.
During her visit, Ms Carlsson also visited Ramotswa, a village outside of Gaborone, to witness how communities are coming together to accelerate the AIDS response. She also visited Tebelopele clinic in Gaborone, which provides integrated HIV and health services to a wide range of people, including female sex workers, men who have sex with men and adolescent girls and young women.
Region/country




Feature Story
UNAIDS continues to support the response to the HIV outbreak in Pakistan
18 June 2019
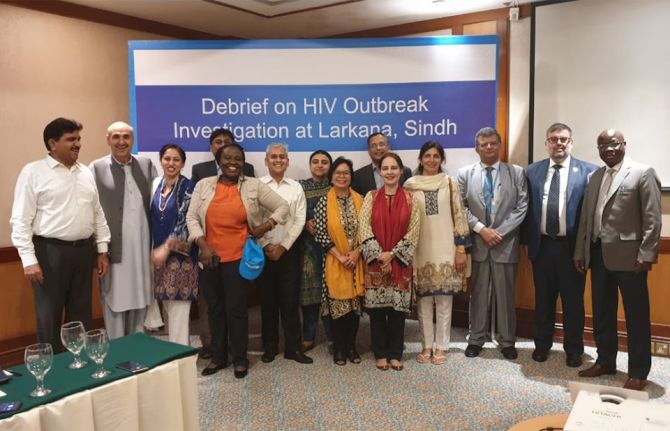
18 June 2019 18 June 2019UNAIDS is continuing its support to Pakistan in responding to the outbreak of HIV in Larkana, during which more than 800 people have been newly diagnosed with the virus. More than 80% of the new cases are among children aged under 15, with most among children aged under 5. By 17 June, 396 people had been referred to treatment.
At a press conference on June 14 the authorities presented the findings of a preliminary investigation into the outbreak. It concluded that poor infection control practices, including a lack of sterilization and the re-use of syringes and intravenous drips, are the most significant factors behind the rise in new infections.
“There is a huge amount of work that needs to be done to improve infection control and support the affected children and their families,” said UNAIDS regional director, Eamonn Murphy, during the press conference held in Karachi, Pakistan. “UNAIDS will continue to facilitate and coordinate within the United Nations system and with other partners to ensure that the required support is provided effectively and efficiently,” added Mr Murphy.
As well as improving infection control procedures, the preliminary investigation found that strengthening community education is critical to raise awareness about HIV prevention and to tackle stigma and discrimination. The conclusions of a rapid assessment on HIV-related knowledge presented at the press conference found that information about HIV is very limited among the affected communities. Many parents and caregivers learnt about HIV only on the day their children were diagnosed or because of media reports about the increase in cases. A lack of accurate information created panic and some families with children diagnosed with HIV have been shunned and isolated.
In response, UNAIDS in partnership with UNICEF, UNFPA, the World Health Organization and the JSI Research and Training Institute have been supporting national partners to develop a community response plan to promote health education and reduce stigma and discrimination. The Sindh AIDS Control Programme, together with UNAIDS and UNICEF, has started to train health workers on paediatric case management and health education sessions are being organized with the involvement of community led organizations and religious leaders. Training sessions for local media on responsible HIV reporting are also being carried out.
UNAIDS has been working closely with the federal and provincial governments to provide on-site technical support to help respond to the crisis and mitigate its impact. Sindh’s Ministry of Health has increased its efforts to prevent unlicensed and informal medical practices from operating and, as a result, 900 health clinics and unlicensed blood banks have been closed.
The preliminary investigation was led by the World Health Organization, in partnership with organizations including the Sindh AIDS Control Programme, Aga Khan University, the Field Epidemiology and Laboratory Training Programme, the Dow Medical University in Karachi, the Microbiology Society of Infectious Disease and UN agencies, including UNAIDS, UNICEF and UNFPA.
With 20 000 new HIV infections in 2017, Pakistan has the second fastest growing AIDS epidemic in the Asia Pacific region, with the virus disproportionately affecting the most vulnerable and marginalized, especially key populations. UNAIDS continues to work with the government and partners in Pakistan to strengthen the response in the country.
Region/country

Feature Story
China marks International AIDS Candlelight Memorial Day
19 June 2019
19 June 2019 19 June 2019The International AIDS Candlelight Memorial, coordinated by the Global Network of People Living with HIV, is one of the world’s oldest and largest grassroots mobilization campaigns for HIV awareness in the world. In May, the UNAIDS country office in China invited members of community-based organizations to lead a commemorative event to mark the 36th International AIDS Candlelight Memorial at the United Nations headquarters in Beijing.
Organized by the Man Wellness Center and Beijing Love Without Border Foundation under the theme of "Ignite Hope, Blessing for Love,” the event brought together community members, activists, young people, healthcare providers, private sector representatives and other people working in the response. They remembered those lost to AIDS-related illnesses and re-committed their efforts to end the AIDS epidemic as a public health threat by 2030.
During the ceremony, the director of UNESCO’s Beijing office, Ms. Marielza Oliveira, welcomed the significant advances made in the response to AIDS, emphasizing the medical and scientific advances that could now be used to reduce the impact of the epidemic. She called on people to join together to reduce the stigma and discrimination associated with the virus to ensure that everybody could share in the progress being made.
Participants at the event received the latest material about HIV treatment and prevention options.
Civil society activists in China are working hard to get the message across that as long as people living with HIV take treatment regularly and are virally suppressed, they are not infectious: Undetectable = Untransmittable.
Young people were prominent at the event. Volunteers from the Core Group for AIDS Prevention and the Red Cross Society of China’s Beijing branch attended and committed themselves to creating a discrimination-free environment for people living with and affected by HIV.
As dusk fell, people lit candles in memory of those that have been lost to AIDS-related illnesses.
At the end of the ceremony, people came together to place their candles on a commemorative red ribbon.
The event once again demonstrated the central role played by communities in the response to the AIDS epidemic.

Feature Story
Positive health, education and gender equality outcomes for Myanmar youth
14 June 2019
14 June 2019 14 June 2019This story was first published by UNESCO
Young people in Myanmar make up more than half of the national population, with 5-14-year-olds making up the largest group. This youthful population brings incredible potential for sustaining Myanmar’s recent development momentum, but only if investments are made to address the challenges that prevent them from making informed decisions about their health and well-being.
Research shows that young people in Myanmar have a limited understanding of sexual and reproductive health, with 38 per cent of adolescents admitting they did not know a woman could become pregnant if she has sex only once, and only 16.67 per cent of young people aged 15 - 24 having accurate HIV prevention knowledge.
To address these issues, UNESCO Yangon, in collaboration with the Ministry of Education, held a policy seminar on 22 March, 2019. More than 50 representatives from Government and non-Government organizations came together to share good practices and identity opportunities for strengthening sexuality education policy, curriculum and teaching in Myanmar.
The event featured the launch of the Myanmar-language version of the 2018 revised International Technical Guidance on Sexuality Education (ITGSE), developed by UNESCO, in partnership with the World Health Organization, UNICEF, UNFPA, UNAIDS, and UN Women. The Technical Guidance assists education, health and other relevant authorities in the development and implementation of sexuality education programmes and materials.
UNESCO regional advisor for health and education, Kabir Singh, said the UN Technical Guidance covers a wide range of topics; going beyond sexual and reproductive health to include broader life skills such as negotiating consent and staying safe.
“While young people in Myanmar face challenges in accessing sexual and reproductive health (SRH) information and services, the situation is further exacerbated by social and gender norms that prevent children and young people, particularly girls and other vulnerable groups, from achieving good health and well-being,” he said.
“This is why it is critical that CSE programmes begin at the ages of 5 – 8, as outlined in the UN Technical Guidance. We need to help children at the earliest ages understand gender equality, healthy relationships, and respect for themselves and one another.”
Sexuality education in Myanmar
The National Life Skills Education curriculum in Myanmar, developed by the Ministry of Education (MoE) in collaboration with UNICEF, has been part of the core curriculum in primary schools since 2006, and in middle schools as a compulsory co-curricular subject since 2008. The lower secondary curriculum (grades 5-8) covers seven themes, including reproductive health, HIV and STIs, substance use, and disease prevention and nutrition.
A 2012 assessment of Life Skills Education in middle school found that knowledge around reproductive health was low, with the authors suggesting that cultural sensitivity and lack of teacher training may be contributing factors. A recent UNICEF U-Report, a free SMS social monitoring tool for youth participation in Myanmar, also found that most survey respondents learned about sexuality education through social media, a source that is often not scientifically accurate or age-appropriate.
At the 2019 UNESCO-led policy seminar, Myanmar government representatives agreed to review Life Skills Education in the context of the UN Technical Guidance, ensuring the sexuality education being delivered is comprehensive and age-appropriate. Representatives also indicated that comprehensive sexuality education should be strengthened as part of current education reforms to the basic education curriculum and pre-service teacher education curriculum.
Min Jeong Kim, Head of UNESCO Myanmar Project Office, welcomed the close working relationship between UNESCO and the Ministry of Education in introducing comprehensive sexuality education into the education system.
“The Ministry of Education has shown strong leadership in their efforts to address the challenges faced by children and young people, such as gender inequalities, and sexual and reproductive health. UNESCO shares this commitment to positively impact young people’s lives and look forward to continuing to work in partnership the curriculum core team and the Teacher Education Colleges to integrate CSE into the new curriculum for teacher education,” Min Jeong Kim said.
Delegates at the policy seminar discussed ways in which to introduce comprehensive sexuality knowledge and related life skills to current and future generations of children and young people in Myanmar. The seminar provided a platform that bridged key stakeholders such as public service providers, development partners and non-Government organizations, with a view to starting a dialogue on comprehensive sexuality education, understanding the gaps and identifying the best way forward for full implementation.
The revised technical guidance on sexuality education
The original international technical Guidance published in 2009 positioned sexuality education primarily as part of the HIV response. However, while HIV prevention remains important, evidence and practice demonstrate that sexuality education has a much broader relevance to other issues, not only for young people’s sexual and reproductive health but also for their overall wellbeing and personal development.
The revised Guidance presents sexuality with a positive approach, recognizing that CSE goes beyond educating about reproduction, risks and disease. It reaffirms the position of sexuality education within a framework of human rights and gender equality. It reflects the contribution of sexuality education to the realization of several internationally agreed commitments in relation to sexual and reproductive health, as well as the achievement of the goals in the 2030 Agenda in relation to health and well-being, quality and inclusive education, gender equality and women and girls empowerment.
Based on a review of the sexuality education around the world and drawing on best practices in the various regions, the Guidance demonstrates that sexuality education:
- helps young people become more responsible in their attitude and behaviour regarding sexual and reproductive health
- is essential to combat the school dropout of girls due to early or forced marriage, teenage pregnancy and sexual and reproductive health issues
- is necessary because in some parts of the world, two out of three girls reported having no idea of what was happening to them when they began menstruating and pregnancy and childbirth complications are the second cause of death among 15 to 19-year olds
- does not increase sexual activity, sexual risk-taking behaviour, or STI/HIV infection rates. It also presents evidence showing that abstinence-only programmes fail to prevent early sexual initiation, or reduce the frequency of sex and number of partners among the young.
Region/country
Related



Feature Story
Ukraine: government to fund publicly procured HIV services
18 June 2019
18 June 2019 18 June 2019Ukraine has announced that it is to allocate $16 million to the country’s AIDS response for 2019-20, which will sustain and expand HIV prevention and support services for key populations as well as care and support services for people living with HIV.
The procurement of HIV services for key populations and people living with HIV from suppliers, including non-governmental organizations, will be managed by the Ministry of Health’s Centre for Public Health, using public procurement procedures. The new process will begin in July.
The move is an important part of Ukraine’s transition from donor funding to a nationally funded AIDS response.
"Ukraine has taken an important step towards moving from international funding to a nationally coordinated policy and ownership,” said Vladimir Kurpita, director of the Centre for Public Health at the Ministry of Health.
The list of services covered by the new policy includes targeted HIV information services and consultations, harm reduction programmes, including needle exchange and distribution, the distribution of condoms and lubricants, HIV testing and screening for tuberculosis. Key populations prioritized include gay men and other men who have sex with men, sex workers, and people who inject drugs. HIV care and support services include strengthening treatment adherence and retention under medical supervision and the involvement of partners of people living with HIV in health care services.
Mr Kurpita promised a smooth transition and said that the government would procure quality-assured services from local non-governmental organizations with the relevant experience and capacity to deliver.
“Nobody who was reached through prevention, support and care services that were funded by external donors should ever be cut off from the transition to government support,” he said.
The head of the All Ukrainian Network of People Living with HIV, 100% Life, Dima Sherembey, encouraged everyone to engage in the process.
"If you are an NGO service provider, engage in bidding; if you are a representative of the donor community in Ukraine, motivate your partners and subcontractors on the ground; and if you have resources and knowledge, provide technical support and assistance to bidders so that they can be successful recipients and implementers of this important wave of government funding,” he said.
UNAIDS country director Roman Gailevich welcomed Ukraine’s commitment to increase domestic funding for the AIDS response.
“We are entering a new era of the national response to HIV in Ukraine,” he said. “We hope Ukraine will not only show that this new model of procurement of HIV services is viable, but that it will also serve as an example to other countries in the region.”
Region/country



Feature Story
Stepping up for China’s AIDS response
13 June 2019
13 June 2019 13 June 2019Zhou Kai has worked in the UNAIDS China office for almost 13 years and has been involved in the AIDS response for more than 16 years. Before this, she was a university lecturer and researcher in paediatric and adolescent health for ten years.
Ms. Zhou’s experience demonstrates how China’s AIDS response has evolved over time. She first worked as a clinical researcher at the China Integrated Programme on AIDS before joining UNAIDS in 2006 to manage the coordination of the nine co-sponsor agencies that are behind UNAIDS in China.
“The AIDS response strategy in China was very weak at the time,” says Ms. Zhou.
Ms. Zhou began working on HIV prevention among key populations. As a doctor she provided strong technical support on HIV testing and prevention to national counterparts and strengthened community participation in prevention programmes.
In the following years, the AIDS response in China gradually improved. The Chinese government hoped to share its experience and began working on development projects, including in the health sector, to strengthen China-Africa collaboration.
One of the agendas for China-Africa cooperation is sharing best practice between China and African countries. In 2018, with the support of the UNAIDS Regional Support Team for Eastern and Southern Africa and the United Nations Office on Drugs and Crime, Ms. Zhou helped facilitate a visit for officials from Uganda, Kenya, and Tanzania to Beijing and to Yuxi in Yunnan province in the south-west of the country.
During the visit, the delegates visited a rehabilitation clinic for people who use drugs and learned about the needle and syringe exchange programmes and opioid substitution therapy projects which have significantly reduced HIV infections among people who inject drugs.
Another of Ms. Zhou’s responsibilities is to advocate for the local production of medicines and health commodities in Africa. “I believe the local production of pharmaceuticals is essential if Africa wants to achieve further progress in the AIDS response and public health. It’s not purely a health issue, but closely linked with a country’s industrial development.” She started to work on the file in 2014 and transferred to her current position of policy and strategy adviser in 2018.
Through her efforts, several two-way visits have been arranged. These have resulted in the agreement of several partnerships between Chinese pharmaceutical companies and African counterparts.
On the country level, China-Africa cooperation has also been bolstered. The Roundtable of China-Africa Cooperation upgraded to the Forum on China-Africa Cooperation (FOCAC), elevating the academic dialogue to a multiple-themed forum at the country level.
As the Belt and Road Initiative attracts more countries, Ms. Zhou sees more opportunities for South-South cooperation. She also expects to expand public health cooperation to more Asian countries to share knowledge and experience between them.
UNAIDS has signed strategic partnership agreement with China that strengthens cooperation around the Belt and Road Initiative and the 2030 Agenda for Sustainable Development, including the scale up of the local production of medicines and health commodities.
“There is a huge potential for China to engage in South-South cooperation and make progress in the AIDS response and public health," said Ms. Zhou "The partnership will also benefit from the Belt and Road Initiative."

Feature Story
Leadership as a process of influence
11 June 2019
11 June 2019 11 June 2019Accelerating progress towards gender equality and the empowerment of women is fundamental to ending the AIDS epidemic. And it starts within UNAIDS.
In 2018, UNAIDS released its Gender Action Plan 2018-2023 aimed at improving the effectiveness of UNAIDS by promoting women’s leadership across the organization and ensuring that all staff, women and men, are aware of the issues that increase women’s risk of HIV infection.
The first annual progress report of the Gender Action Plan 2018-2023 shows progress in reaching its targets although much remains to be done. “The Gender Action Plan is a tool for change,” according to Gunilla Carlsson, UNAIDS Executive Director, a.i. “Building on the impressive progress made over just the first year of its implementation, it is key to keep up the momentum and sustain achievements over time.”
Of the 30 actions identified to achieve the four targets set out in the five-year Gender Action Plan, UNAIDS successfully advanced in 20 of them over the first 12 months. “The Gender Action Plan matters because it is about equality, balance, justice and fairness”, said Helene Badini, Regional Community Advisor in UNAIDS’ regional support team in Dakar, Senegal.
The Plan includes training and mentorship opportunities, mandatory gender-related work objectives, and organization-wide support. “All the staff in my office have a learning objective on gender and I advocate against all gender-based violence,” reflected Francoise Ndayishimiye, UNAIDS Country Director in Gabon. “Also, as a member of UN Plus, I like to be connected with other HIV-positive women working at UNAIDS to unite our strengths and act together,” she added.
In the West and Central Africa region, the majority of UNAIDS staff are men and half of the UNAIDS country directors are women, leading small teams in countries belonging to a region struggling with one of the fastest growing AIDS epidemics globally and severe challenges relating to security, humanitarian and natural disasters. Marie Engel, UNAIDS Regional Programme Advisor in Dakar believes that “having a network of women colleagues is a powerful and unique tool to advance women’s leadership, and this is why in my current role I am facilitating collaboration between the West and Central Africa alumnae of the Women’s Leadership Programme”.
The Gender Action Plan recalls that gender equality is a human right and critical to the performance and effectiveness of UNAIDS. The importance of advancing gender equality, including through the achievement of gender parity, is now recognized to an increased extent.
The plan, which is primarily for staff, rapidly translates into programmatic action. In the Democratic Republic of Congo, for example, UNAIDS helps women involved in civil society networks of people living with HIV to develop their skills and to reduce self-discrimination and self-stigma. Network members travelled to New York in 2018 to participate in the Commission on the Status of Women to share their experiences. The woman behind this work is Natalie Marini Nyamungu, a human rights and gender equality advisor in the UNAIDS’ country office.
“I developed skills that allowed me to create a positive work environment with equality and respect for diversity at its core, and without discrimination or prejudice,” said Ms Nyamungu. “I have also helped our civil society partners develop the new skills, resources and self-confidence that they needed to boost their own leadership.”
Supporting women’s leadership is central to the Gender Action Plan. The experience of female staff at UNAIDS has convinced many that leadership is a process of influence, not just a position in the organizational hierarchy.
Aminata Ouattara, Executive Officer in the UNAIDS regional support team in Dakar sums it up.
“UNAIDS Gender Action Plan has had the same effect as when you hop on public transport. Instead of taking your own car, the bus will fight the traffic for you and get you where you want to be much faster.”.


