
Feature Story
‘We Can’t Afford to Go Back’- UNAIDS Country Director on HIV funding cut in Eswatini
14 May 2025
14 May 2025 14 May 2025Eswatini, a country once described as the epicentre of the HIV epidemic with nearly 1 in 3 adults living with HIV in 2015 [adult HIV prevalence in 2015 was 31%]. But Eswatini managed to turn around its HIV epidemic, reducing new HIV infections from a peak of 21 000 per year in 2000 to 4 000 in 2023, a remarkable result, achieved with the support of US funding.
However, the sudden US funding cuts threaten to undo years of progress. We sat down with Nuha Ceesay, UNAIDS Country Director in Eswatini, to discuss the current situation, the impact on HIV services, and the way forward.
Q: How are US funding cuts impacting Eswatini’s HIV response?
Eswatini’s HIV response has been a success story, by transforming a crisis that once saw extremely high HIV prevalence rates, into a model of resilience and opportunity. But the recent US funding cuts, representing about half of the country’s HIV response budget, have left the people living with and affected by HIV in despair, the government was not notified and left unprepared, and the people working to end AIDS are in total shock. There is real concern that new HIV infections and AIDS-related deaths will rise, reversing years of hard-won progress. The cuts threaten not just HIV treatment and prevention, but also the broader health system improvements, data collection, jobs and empowerment of people living with HIV.
Q: What disruptions are being seen on the ground?
The effects are immediate and widespread. HIV testing services, the gateway to treatment, are now limited. With fewer people being tested, many may unknowingly be infected with HIV, missing the chance for early treatment and increasing the risk of further transmission. This could push annual new infections, which are currently around 4 000, even higher, and add pressure to already strained treatment resources. Stockouts of antiretroviral, lab test kits, and condoms are expected within months, and health worker layoffs are affecting service delivery and quality data collection. Primary prevention services, such as medicine to prevent HIV (PrEP), education campaigns, and voluntary medical male circumcision for HIV prevention (which is around 60% effective in preventing HIV) have also been scaled back or suspended.
We are also seeing a stop of the DREAMS programme which is a major setback for adolescent girls and young women, who are disproportionately affected by HIV in Eswatini. DREAMS provided prevention education, skills, and socio-economic support to young women. Its termination leaves them more vulnerable to infection and strips away resources that have been central to empowering this high-risk group. HIV prevalence among young women and girls aged between 15 and 24 years was 70% higher than among young men in Eswatini in 2023.
Read more about the impact on UNAIDS website
Q: How is UNAIDS responding to these challenges?
UNAIDS is working closely with the government and partners to continue the work of developing and implementing the HIV Sustainability Roadmap. This will help Eswatini’s HIV response to gradually shift from being reliant on international aid to increasing its domestic funding which will lead to the government taking full ownership of its HIV response. The first phase of this roadmap has already been launched, focusing on building resilience and long-term solutions.
UNAIDS has also worked closely with the Ministry of Health and partners to map the impact of the funding cuts, identify service gaps, and strategize on mitigating disruptions. Collaboration with the Ministry of Health, UN partners, and civil society remains central, but the transition to sustainability is a complex and gradual process.
Q: What’s your message to the international community?
The successes that we celebrate in the HIV response are built on mutual accountability and global solidarity. That’s what enabled countries like Eswatini to shift the narrative-from a crisis by leading a response that brought down new HIV infection to 4 000 compared to when new infections were as high as 21 000.
It is therefore devastating to see all the hard-won gains being reversed at this stage. This is the moment we need to come together in solidarity and in partnership to accelerate our collective efforts.
Ending the epidemic is like a marathon. We have run the race many miles, but the end is what matters. If we cannot reach that finish line, it means we have not completed, and we cannot afford that.
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads the global effort to end AIDS as a public health threat by 2030 as part of the Sustainable Development Goals.
Following the US stop work order in January, UNAIDS is working closely with governments and partners in affected countries to ensure that all people living with or affected by HIV continue to access life-saving services.
For the latest updates, please visit unaids.org
Related resources
Watch: "Access to prevention services no longer available", Nuha Ceesay, Eswatini UNAIDS Country Director
Watch: UNAIDS actively working on forward planning with governments, says Eswatini country director
Watch: "From crisis to opportunity," says UNAIDS citing Eswatini HIV response
Region/country
Related



Feature Story
Community-led HIV services under threat: global networks and UNAIDS track the impacts of the US funding cuts
13 May 2025
13 May 2025 13 May 2025Community-led organizations are the backbone of the HIV response in many countries, providing access to HIV services for key populations, advocating for human rights and monitoring the HIV response. However, data collected by community-led organizations shows mass shut-downs of life-saving, peer-led services, significant – or total – budget cuts, staff lay-offs and rising levels of stigma, discrimination and mortality rates.
Two new key population-led reports, one by Global Black Gay Men Connect (GBGMC) and another by the International Network of People Who Use Drugs (INPUD), document the consequences of the US President’s Executive Order in January 2025 which froze all US foreign assistance. These reports highlight how services led by and for key populations are facing deep uncertainty about their future due to the funding cuts and loss of staff.
In its Frozen Out report, GBGMC found that 36% of partners supported by the US President’s Emergency Plan for AIDS Relief (PEPFAR) shut down within one week of the Executive Order. Another 19% said they could not operate beyond one month without renewed support. Similarly, INPUD’s report The Human Cost of Policy Shifts describes significant disruptions across harm reduction programmes. Nearly half (45%) of the organizations surveyed reported major budget losses, and one in four lost between 75% and 100% of their harm reduction programming. Critical services including peer-led outreach, HIV and hepatitis C testing, opioid agonist therapy, and overdose prevention have been disrupted.
A cascading crisis
The GBGMC report states that nearly 93% of key population-serving partners in Kenya reported experiencing full or partial service shutdowns. In Nigeria, every PEPFAR implementing partner providing services to key populations was reportedly affected. Across Kenya, Uganda and Nigeria, an estimated 2.2 million people have lost access to key population-focused HIV prevention services.
The report also warns that even short-term interruptions can have life-threatening consequences. Each day, an estimated 200,000 people rely on receiving their HIV treatment through US government-funded sites. Interruptions risk treatment failure, HIV transmission and the emergence of resistance to HIV medicines. Prevention efforts are also at risk, with US government funding supporting nearly 90% of global pre-exposure prophylactic (PrEP) initiatives.
“The PEPFAR funding freeze has led to the closure of numerous organizations and the disruption of essential HIV prevention services, leaving millions at risk. Immediate action is imperative to restore funding and protect key populations from further harm,” says Micheal Ighodaro, Executive Director of GBGMC
Impacts on organizations led by people who use drugs
INPUD’s report, The Human Cost of Policy Shifts, provides a detailed picture of how harm reduction services have been devastated by the US funding cuts. Based on a global rapid assessment of 101 respondents, the report reveals that nearly half lost between 26% and 100% of their harm reduction budgets, and 23% lost more than three-quarters of their funding.
The most disrupted services included peer-led outreach (41%), legal and human rights support (36%), HIV testing (35%), services for women who use drugs (33%), and overdose prevention (25%). The consequences for individuals and communities have been severe. 47% of organizations reported that people are now going without harm reduction supplies such as sterile syringes and naloxone, and 46% said people are relying on underground or informal networks for access. 30% observed increases in overdose deaths. Additionally, 62% of organizations documented rising stigma and discrimination against people who use drugs.
The report also highlights a particularly stark impact on women who use drugs. Of the 54 organizations that previously offered tailored services for women, 68% halted outreach, and over a third had to reduce or close services altogether.
“While increasing overall funding is important, it is equally vital to ensure that organizations led by people who use drugs receive targeted support to run harm reduction services that effectively address their communities’ unique challenges and needs," says Anton Basenko, Executive Director of INPUD
Heightened stigma and structural risks
Even before the funding cuts, key populations faced legal and social barriers
including criminalization, discrimination, and denial of services. According to reports gathered through UNAIDS’ dialogues with global and regional networks, these challenges are now intensifying. Community organizations have documented a rise in harassment, hate speech and healthcare discrimination. In some countries, specialized clinics are being “mainstreamed” into general health systems without adequate training or protections ensuring safe access.
UNAIDS’ response and coordinated action
Since February 2025, UNAIDS has been convening biweekly virtual dialogues with global key population networks, civil society advocates and international partners to share updates, raise concerns, and coordinate efforts to protect HIV services. At the regional level, UNAIDS is also convening with networks and joining forces to document the impact of funding disruptions and shape collective responses. These engagements have informed UNAIDS’ advocacy and programming supporting the launch of tools like the Rapid Action Financing Tool, strengthening country-level tracking through the UNAIDS impact portal (launched in early 2025) and amplifying community voices at global forums such as the UN’s Commission on the Status of Women and the Human Rights Council. Through continued collaboration with country teams, regional networks, and civil society, UNAIDS remains committed to co-creating solutions and prioritizing community-led responses.
A call for urgent action
GBGMC and INPUD urge governments, donors, and development partners to take immediate steps to:
- Restore and increase funding for community-led and key population-focused services and establish dedicated funding streams for key population-led organizations
- Establish pooled emergency funding mechanisms to sustain prevention and harm reduction
- Ensure meaningful community engagement in funding, service design, and legal reform
- Protect peer-led HIV services, which are grounded in principles of dignity, safety, and equitable access
Related documents


Press Statement
UNAIDS launches bold transformation to sustain progress and end AIDS by 2030
10 May 2025 10 May 2025As the global HIV response faces rising risks, UNAIDS shifts to a leaner, sharper model focused on country impact
GENEVA, 10 May 2025—In the face of continued high numbers of new HIV infections and declining global funding, the Joint United Nations Programme on HIV/AIDS (UNAIDS) is launching a bold transformation to support countries in ending AIDS as a public health threat by 2030, and to ensure the HIV response remains strong and sustainable into the future. This shift will help governments and communities transition to a sustainable and domestically financed HIV response, grounded in data, equity, and human rights.
“UNAIDS’ transformation is a direct response to a fast-changing landscape, from a shifting geopolitical context to shrinking resources,” said Winnie Byanyima, Executive Director of UNAIDS. “We are reshaping how we work so that we can support inclusive, community led, multisectoral national HIV responses with greater precision and impact.”
UNAIDS restructuring and reform processes are closely aligned with wider UN processes through the UN80 initiative and promote enhanced efficiency, integration, consolidation and coordination.
The restructuring of the UNAIDS Secretariat is informed by the work of a High-Level Panel which has been working since October 2024. The Panel called for transforming the Joint Programme now and through to 2030 and recommended a smaller, sharper focused model for the Secretariat. It called on the Secretariat to focus on four core functions: leadership; convening and coordination; accountability; and community engagement.
Disruptions in the HIV response
UNAIDS modelling suggests that we are now seeing 2300 additional new HIV infections every day on top of the 3500 infections that were already occurring. These reversals are happening as a result of human rights push backs on women and girls and key populations coupled with disruptions in lifesaving services as international assistance from donor countries stopped. UNAIDS estimates that the funding cuts could lead to an additional 6.6 million new HIV infections and 4.2 million AIDS-related deaths by 2029. A tragedy for people living with and affected by HIV.
Reshaping to deliver in a changing context
UNAIDS is facing a big transition and is reforming to continue to support the response in the most efficient and cost-effective way. The Secretariat is consolidating its country footprint and will be moving global staff to be closer to the people we serve.
The physical in-country presence of the Secretariat will be reduced to approximately 35 countries while continuing to be able to support around 60 countries directly. The change is based on a typology of countries with high HIV burden, significant stigma and discrimination against key populations, and heavy reliance on international aid for the HIV response. The restructuring plan includes a 54% reduction in Secretariat staffing strength to ensure UNAIDS is fit for purpose and working within current core resource forecasts.
UNAIDS’ transformation is about supporting countries to protect the critical gains made in stopping new HIV infections and preventing AIDS-related deaths. UNAIDS will continue to support countries in monitoring their epidemics and making strategic investments for HIV prevention and treatment, as well as addressing human rights and policy barriers. It will convene partners, engage communities and stand with people living with and affected by HIV.
“This is a moment for global solidarity,” said Ms Byanyima. “With determination, and partnership, together we can still achieve the goal of ending AIDS as a public health threat by 2030 and ensure sustainable, inclusive, multisectoral national HIV responses into the future.”
In 2025, UNAIDS will shape and deliver a new Global AIDS Strategy to accelerate political, programmatic and financial commitment and sustainability and provide guidance to drive progress towards the goal of ending AIDS as a public health threat by 2030. The Strategy will be adopted by the UNAIDS Programme Coordinating Board in December 2025. It will provide the foundation for a new Political Declaration and 2030 HIV targets, to be adopted by a High-Level Meeting of the UN General Assembly in 2026.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.




Feature Story
HIV services and social reintegration programmes for prisoners and newly released detainees in Kyrgyzstan at risk of collapse
08 May 2025
08 May 2025 08 May 2025On the outskirts of Bishkek, the capital of Kyrgyzstan, a small house converted into a shelter welcomes people recently released from prison. The shelter is funded by the Global Fund/UNDP project “Effective Control of HIV Infection and Tuberculosis in the Kyrgyz Republic.”
Madina Toktogulova, head of the public foundation Istikhsan, which supports the shelter, is preparing to welcome her clients.
For 25 years, Madina has worked with people in prison, people who use drugs, and those living with HIV and tuberculosis. As a community representative, she was at the forefront of establishing the country’s first grassroots initiatives, self-help groups, and community-based organizations. She played a key role in developing social support and rehabilitation programmes for people in vulnerable situations.
Together with a group of like-minded colleagues, she established the country’s first peer support groups in correctional facilities. They persuaded prison administrations of the importance of providing HIV prevention services, including harm reduction, to people in prisons; they built relationships with prison health professionals, social workers, and psychologists; implemented HIV prevention projects; and helped people newly released from prison who had no place to stay, clothes, or money to return home.
Dr Gulsara Kukanova, a physician at the FSIN hospital-polyclinic in Kyrgyzstan, stressed how vital organizations like Istikhsan are the moment people are released from prison as some stop taking antiretroviral treatment or relapse into drug use. “We partner with organizations like Istikhsan and witness people rebuilding their lives — finding jobs, reuniting with family. Offering hope to someone who has lost it is invaluable.”
Madina knows that without food, shelter, or ID, HIV treatment is not a priority. That’s why she advocates for a comprehensive approach to reintegration.
“People need more than just medical care. They need psychological support, help finding a job, restoring their documents. Non-governmental organizations, with donor support, play this essential role — helping people rediscover themselves,” she explains.
Istikhsan’s work focuses on supporting incarcerated women. Madina says women are more emotionally vulnerable, more affected by violence – the harsh reality of prisons, trauma, stigma, and self-stigma. They are more likely to give up on therapy and lose hope.
“Society forgives men more easily. Women with a prison history are judged more harshly. Maybe because I’m a woman, I feel their pain more deeply,” she says.
The organization is currently providing support to all women living with HIV in a nearby prison. Thanks to their efforts, more than 20 women have been able to restore their identity documents, dozens are receiving psychological and medical support, starting HIV treatment, reconnecting with children, finding jobs, and reintegrating into society.
But all of this is now at risk. HIV prevention efforts built over years through partnerships with government, civil society, and international institutions face collapse due to shrinking funding from key donors, including PEPFAR and the Global Fund.
According to Madina, a systemic approach to reintegration is impossible without cooperation between government institutions and civil society.
“We have a very good probation law that provides a legal framework for supporting people on the path to resocialization. However, as with any system, there are times when resources and human capacity are not sufficient to reach everyone in need. That’s when civil society can step in — in partnership with the state and within the framework of the existing legislation,” she emphasizes.
While the Kyrgyz government fully covers HIV treatment, there’s a real risk that essential social and prevention services — post-release support, reintegration, temporary housing, documentation help, hygiene kits — will be lost without external aid.
“The loss of funding could dismantle the entire support system for women living with HIV in prison. These programmes are not charity; they’re investments in resilient health and social protection systems that can operate independently. Investing now means building a future where everyone’s right to health is protected,” says Meerim Sarybaeva, UNAIDS Country Director in Kyrgyzstan.
“For the first time, we’ve created a model where probation services, prisons, and NGOs collaborate daily, so no one falls through the cracks,” says Chinara Maatkerimova, Programme Officer at UNODC in Kyrgyzstan.
“If we disappear, who will hear them?” Madina asks. But she’s determined to continue — even if it means starting over — to advocate for sustainable funding and rebuild a system where every person, regardless of their past, has a right to health and a future.
As of April 1, 2025, Kyrgyzstan has reported 14,609 cases of HIV. Of these, 61.8% were transmitted sexually and 27.8% through injection drug use. HIV is increasingly being detected among people outside of traditional key populations — a sign of the epidemic’s broader spread in the country.
Region/country




Feature Story
The Breaking Point: A Story from Ethiopia
06 May 2025
06 May 2025 06 May 2025In April 2025, silence fell over Bahir Dar. Once a lifeline for people living with HIV, key populations, and young people—as the US funding pause began to bite. Funding cuts disrupted services. A few held on without salaries but eventually, even they stopped showing up. Confused and anxious clients arrived to find the gates closed. Some waited. Others turned away.
The crisis quickly spread from Bahir Dar, where key population programmes came to a halt. Outreach workers, who had built trust door by door, were laid off. Fear took hold. Clients asked for extra medication, unsure whether services would return. Peer support groups vanished, and with them, protection against stigma and transmission.
"I often find myself overwhelmed with stress,” said a woman from a women led association. “If the medicine and other services stop coming, where will I go? I simply don’t have the financial means to afford the treatment I need.”
The data collected by the women-led association of people living with HIV is stark. For two months, no new clients have been enrolled in PrEP, the prevention prophylaxis taken orally that protects from HIV infection.
“One of my biggest concerns is the fear of not having access to condoms,” said a case manager from the women led association. “Without them, we know HIV can spread much more easily.”
In the face of this collapse, the UNAIDS Ethiopia team visited Bahir Dar and surrounding towns to document the impact firsthand. They spoke with organizations, youth groups, and people living with HIV. They visited what remained of the services and listened to voices that too often go unheard—adolescents, mothers, peer educators—people still holding the line, even as systems crumbled around them.
“I worry deeply about the spread of HIV,” said a female member. “Will medicine still be available? Will we still have access to viral load testing? If condoms run short, we risk seeing the virus continue to spread, along with other infectious diseases.”
"Without a financial budget, our members are left without the basics they need to survive; no food, medical care, or even hope," said the association manager. "They have families, they have children, and they rely heavily on this support. It would make a huge difference if members could access free medical treatment and hospital services. Today, many can't even afford one meal a day. Their health is deteriorating; their children are suffering. What they need most is dignity, food, and a fighting chance."
“There’s a real fear that if funding ends, everything else will follow—medicines, condoms, even access to medical personnel,” said a member from the women led association. “Without these, proper care becomes almost impossible.”
And yet, even in collapse, communities are refusing to give up.
Young volunteers have stepped in. They have formed informal networks, checked in on peers, and created WhatsApp groups to stay connected. Mothers banded together to support their children’s treatment. Youth collectives used community radio and shared airtime to spread critical information. Where formal systems failed, communities built their own safety nets.
Bahir Dar was both a breaking point and a wake-up call. It laid bare the fragility of systems built around a single funding stream—when the money stopped, so did the services, the trust, and the hope.
This crisis makes clear that resilience must be built in, not left for later. Emergency preparedness must be a core part of national HIV responses. Community-led organizations must be recognized as essential. And youth-led innovation must be scaled up—because it is young people who keep the response alive when everything else falls apart.
"Resilient communities are the backbone of the HIV response," said Tina Boonto, UNAIDS Country Director for Ethiopia. "When systems collapse, it is communities that hold the line. Their leadership, courage, and innovation are not optional—they are essential. Building lasting responses means putting communities first, not as an afterthought but as the foundation of everything we do."
HIV must remain central to humanitarian, development, and recovery agendas. The intertwined challenges of conflict, displacement, gender-based violence, and HIV demand integrated, people-centered solutions. This won’t happen if HIV is treated as an afterthought or reduced to clinical care alone.
The story of Bahir Dar shows what happens when systems fail, and what people do in their absence. It is a testament that resilience is forged in crisis by those most often left behind who still find ways to move forward.
Related resources
Region/country


Feature Story
US foreign aid cuts puts the lives of people who use drugs at risk
05 May 2025
05 May 2025 05 May 2025Godfrey Swai is shaken. Since the end of January, the US aid funding cuts have meant that he can only afford for his staff to work a couple of hours twice a week compared to a full five days.
As the Executive Director of an organization called Methadone Family Against Drug Abuse based in Tanzania he has had to scramble. “Despite clinics being partly opened, our outreach in hotspots came to a halt,” he said. “The community is scared.”
In many countries, like Uganda, centres distributing opioid agonist maintenance therapy (OAMT), also known as medically assisted treatment, closed for a month. OAMT is often prescribed as oral medication to alleviate withdrawal symptoms and reduce injecting drug use, which in turn lowers the risk of acquiring HIV. In 2022, the risk of acquiring HIV was 14 times higher for people who inject drugs than for people in the overall adult population.
“We know that disruption to OAMT is a threat to life,” said Catherine Cook, Sustainable Financing Lead at Harm Reduction International (HRI).
Banza Omary Banza, Director of Community Peers for Health and Environment Organization in Tanzania, agrees. “Fearing a stock out of methadone–the OAMT medicine–we have witnessed people returning to heroin use and hitting the black market,” he said.
A setback that has a myriad of repercussions.
According to a recently published survey by International Network of People who Use Drugs (INPUD) there has been large-scale suspension of outreach and harm reduction programmes, including needle and syringe distribution, HIV and hepatitis C testing, overdose prevention and legal support services.
“The hardest hit has really been the peer-led outreach,” said Aditia Taslim, Advocacy lead at INPUD. “Three months later no alternative solutions have been put in place. It’s like we are being erased from the HIV response.”
For harm reduction advocates this crisis isn't just financial, it's profoundly human.
“Peers and peer outreach have been the backbone of the harm reduction response," said Juma Kwame, Director of Tanzania Network of People who Use Drugs (TANPUD). “Without people seeking out their peers you don’t have linkages to treatment to health services or to recovery.”
Team leader at a network of women who use drugs in Dar es Salaam, Grace Mbalawa, said that most people living with HIV who use drugs have little income or a stable home, so the loss of support programmes has upended their lives.
“They no longer have a safe space and many are stretching out their HIV treatment by skipping days in case they can no longer get their medicine,” she said. People living with HIV must take daily treatment to stay healthy and suppress the virus. In addition, when the viral loads of people living with HIV are suppressed, sexual transmission of HIV does not occur.
International donor funding comprised 67% of total harm reduction funding in 2022. Most of the money went towards HIV prevention programmes for people who inject drugs. The US President’s Emergency Plan for AIDS Relief (PEPFAR), a decades-long initiative, supported OAMT to 27 000 people in seven countries (India, Kenya, Kyrgyzstan, South Africa, Tajikistan, Tanzania and Uganda). In many cases these were and are the only services available. They also supported harm reduction programmes in Mozambique, Myanmar and Kazakhstan.
Many fear the loss of funding threatens to undermine human rights and marginalize communities already battling stigma and years of neglect with women bearing a big portion of the impact.
“One in three people who use drugs are women but women only account for one in five people accessing services due to the stigma of being a woman using drugs,” said Ms Cook from HRI. “They risk having to admit drug use and face stigma, arrest, losing custody of their children or even violence from the wider community.” Any services tailored to women like the one Ms Mbalawa works for are key as are all peer-led services.
Ms Cook is concerned that if funding for communities and civil society support dries out, the entire harm reduction response may collapse. INPUD also warns that without immediate and strategic intervention, the world could witness a resurgence of HIV, hepatitis C, and overdose epidemics.
UNAIDS, UNODC and partners have been working with governments to encourage increasing domestic funding and mapping out sustainability plans. Central to these include having organisations led by people from the community participating as well as moving funds away from punitive approaches like criminalising drug use to reduce stigma, and inequalities.
“As countries look at new models for how to integrate specific HIV services tailored to serve the needs of people living with HIV or at risk of HIV, including people who use drugs, into general health services, this must include the integration of harm reduction services ” said Suki Beavers, UNAIDS Director of Equality and Rights for All. “And peer-led outreach is part of that equation.”
Mr Kwame stressed, “We need our voice to be heard so that people who inject drugs are part of the health agenda, and our needs are met.”
Related resources
Related


Feature Story
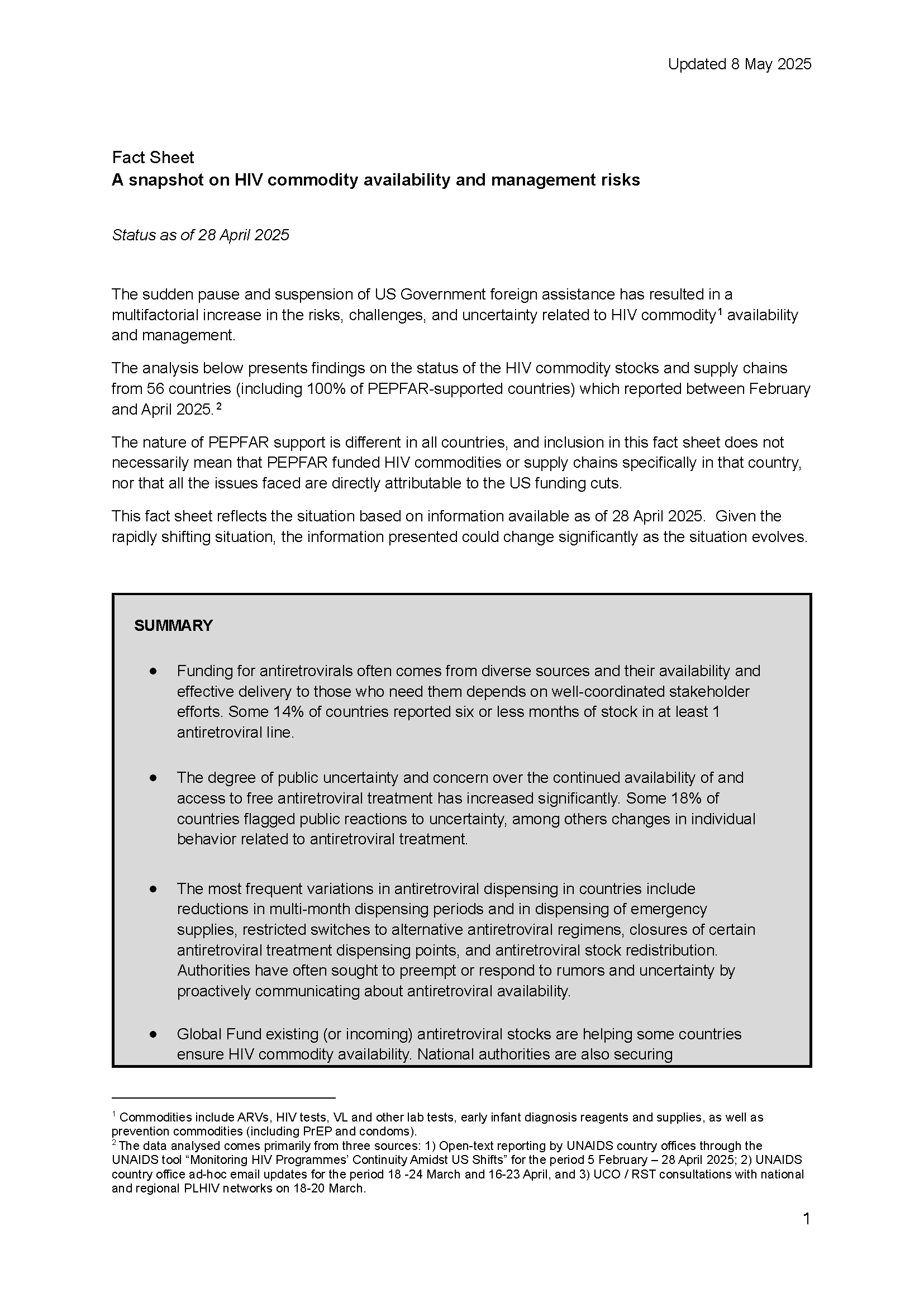
Impact of the US funding cuts: A snapshot on HIV commodity availability and management risks
01 May 2025
01 May 2025 01 May 2025The sudden pause and suspension of US Government foreign assistance has resulted in a multifactorial increase in the risks, challenges, and uncertainty related to HIV commodity[1] availability and management.
The analysis below presents findings from 56 countries (including 100% of PEPFAR-supported countries) which reported on the status of their HIV commodity stocks and supply chains between February and April 2025.[2]
The nature of PEPFAR support is different in all countries, and inclusion in this fact sheet does not necessarily mean that PEPFAR funded HIV commodities or supply chains specifically in that country, nor that all the issues faced are directly attributable to the US funding cuts.
This fact sheet reflects the situation based on information available as of 28 April 2025. Given the rapidly shifting situation, the information presented could change significantly as the situation evolves.
SUMMARY
- Funding for antiretrovirals often comes from diverse sources and their availability and effective delivery to those who need them depends on well-coordinated stakeholder efforts. Some 14% of countries reported six or less months of stock in at least 1 antiretroviral line.
- The degree of public uncertainty and concern over the continued availability of and access to free antiretroviral treatment has increased significantly. Some 18% of countries flagged public reactions to uncertainty, among others changes in individual behavior related to antiretroviral treatment.
- The most frequent variations in antiretroviral dispensation in countries include reductions in multi-month dispensing periods and in dispensing of emergency supplies, restricted switches to alternative antiretroviral regimens, closures of certain antiretroviral treatment dispensing points, and antiretroviral stock redistribution. Authorities have often sought to preempt or respond to rumors and uncertainty by proactively communicating about antiretroviral availability.
- Global Fund existing (or incoming) antiretroviral stocks are helping some countries ensure HIV commodity availability. National authorities are also securing supplementary domestic budget allocations to ensure HIV commodity availability and management.
- Despite the precarious situation faced by many community-led organizations because of the USG shift, they continue to play a central role in engaging and informing communities, addressing rumors, advocating for mitigation actions, and providing early warning on ARV availability, accessibility and cost.
- Significant disruptions affecting combination prevention commodities have been reported as a result of the USG shift. This is due to the dominant role played by PEPFAR in prevention commodity procurement, distribution or delivery in many countries. Some 23% of countries reported six or less months of condom or PrEP stocks.
- Around 21% of countries reported six or less months of stock in at least 1 HIV testing commodity. Careful monitoring of individualized country situations is necessary to mitigate any possible increase in stockout risks.
- Even when HIV commodities exist in-country, they may not always be reaching health facilities – creating patient-facing shortages that undermine trust in treatment continuity. Some 46% of countries reported supply chain management issues.
- The repercussions of the USG shift on the global HIV commodity markets should not be underestimated in the medium term. Sustained predictability in HIV commodity demand forecasts is essential to guarantee a stable supply, maintain prices, and ensure the availability of affordable generic medicines for national HIV responses.
[1] Commodities include ARVs, HIV tests, VL and other lab tests, early infant diagnosis reagents and supplies, as well as prevention commodities (including PrEP and condoms).
[2] The data analysed comes primarily from three sources: 1) Open-text reporting by UNAIDS country offices through the UNAIDS tool “Monitoring HIV Programmes’ Continuity Amidst US Shifts” for the period 5 February – 28 April 2025; 2) UNAIDS country office ad-hoc email updates for the period 18 -24 March and 16-23 April, and 3) UCO / RST consultations with national and regional PLHIV networks on 18-20 March.
Fact sheet
Related resources
Related
.")


Feature Story
From violence to funding cuts, Asia Pacific women living with HIV face old and new challenges
18 March 2025
18 March 2025 18 March 2025“In our country we are not the priority,” Daisy Cruz says plainly.
She is surrounded by other women living with HIV who agree. They share stories that are not often told about the epidemic in Asia and the Pacific. In a region where men living with the virus outnumber women roughly two to one, the issues of women and girls are often overlooked. They are all members of the International Community of Women Living with HIV Asia Pacific (ICWAP).
Eva Dewa was diagnosed in Yogyakarta, Indonesia in 2017.
“I came home seeking a safe space to share my sadness. At that time, I believed that my partner would support me. Instead, he blamed me,” she says.
Ms Dewa has survived intimate partner abuse. She knows she isn’t alone: “A lot of women either experience violence and get infected with HIV, or contract HIV and experience violence.”
She gave birth to twins two years before her diagnosis. During her pregnancy she was never screened. Unaware, she went on to breastfeed for a couple years. When she learned her status, it was she rather than healthcare staff who suggested the children be tested. One child was HIV negative. The other wasn’t.
UNAIDS estimates that under two-thirds (64%) of women living with HIV in Asia Pacific receive treatment to prevent transmission to their babies. This is far lower than the global average of 84%. Ms Dewa reflects that while HIV services for pregnant women are expanding, smaller cities and rural areas benefit more slowly.
Cathy Ketepa understands the challenge of reaching remote districts. Every day in her native Papua New Guinea, five infants are born with HIV. The epidemic there has doubled since 2010 with new infections among women increasing by a staggering 67%.
“Only around half of mothers living with HIV receive antiretroviral therapy,” says Ms Katepa . “We must bridge this gap to protect the health and future of our children.”
But while the women advocate for expanded services to reduce vertical transmission, they are adamant that their dignity, privacy and agency must be respected. The International Community of Women living with HIV (ICW) has conducted a global analysis of the reproductive coercion, mistreatment and abuse experienced by women living with HIV. The study found that across regions, during pregnancy and infant feeding women were most subjected to force.
“There is an issue with coercive practices,” said Sophie Bryon, ICW’s Director of Global Programmes. “We are talking about women being told not to have children, not to have another child, to terminate and being pressured to undergo sterilization. There is still denial of contraception and pressure to use certain kinds of contraception. There are issues ranging from verbal abuse to physical violence.”
There is also stigma. When Ms Cruz went to the hospital in Manila to give birth in 2001, a nurse on the ward loudly asked why she wasn’t breastfeeding.
“All the patients looked at me like there is something different,” she said.
There is a sense from these women that they’ve been ambushed by a threat they didn’t know existed. But having been hit, they will speak up for themselves, and for others.
Christina Montoya didn’t think it was possible for a woman like her to be infected. She was married and only had sex with her husband.
“We must be informed!” she declared. “And all our friends must be informed!”
11 years of ICWAP
ICWAP builds the capacity of women and girls living with HIV and women-led organizations in 18 Asia Pacific countries. It provides coaching and mentoring, ensuring women participate in Global Fund processes and are meaningfully engaged in community-led monitoring.
The organization was formed in 2014 to tackle the human rights violations and violence women living with HIV in the region experience, while removing barriers to treatment and care. Sita Shahi, its Regional Coordinator explains that the challenges can’t be tackled from a health angle alone.
“Women face a lot of stigma and discrimination. They also have an economic burden and are responsible for rearing children. There are so many intersecting issues,” she explained.
Now there are new challenges. ICWAP conducted an eleven-country survey on the impact of the United States development aid stop work order. It found that some country networks have either collapsed or scaled back, leaving women without crucial resources, including information about their rights and how to address gender-based violence or discrimination. There is also reduced access for many women who depended on community-based services for HIV or sexual and reproductive healthcare. While treatment is provided by government in most countries, many of the shuttered peer-led services were more accessible and friendly.
Some women who worked for US-supported programmes have lost their jobs, resulting in financial stress. ICWAP itself has been hard hit.
“We lost all funding. The core support we were receiving for managing staff and country interventions is gone. It is a devastating situation for us. There is now no funding to support our sisterhood at country level,” Ms Shahi explained.
UNAIDS has called for countries in Asia Pacific to support community-led HIV work including stigma and discrimination, adherence counselling, social support, monitoring and advocacy.
Feature Story
The impact of the US funding freeze and cuts on Namibia’s civil society: A struggle for survival
10 March 2025
10 March 2025 10 March 2025A long-standing partnership threatened
For years, Namibia’s HIV response has been supported by US funding, particularly through the United States President's Emergency Plan for AIDS Relief (PEPFAR). These programmes have provided lifesaving drugs for HIV treatment, prevention services, and essential socio-economic empowerment initiatives, especially for adolescent girls and young women and the most marginalized and at-risk groups.
However, given the recent decisions by the US to freeze and cut foreign assistance, Namibians are struggling to fill the funding gaps. An emergency humanitarian waiver issued by the US Government allowed for funding to flow to some projects and organisations (government and non-governmental) – but as the funds were not transferred into their accounts, they are faced with serious cash-flow challenges and were at risk of contravening the labour laws of the country.
The US funding freeze has had a particularly devastating impact on community groups supporting the most vulnerable populations. In Katutura, for example, adolescent mothers who were benefiting from HIV prevention and socio-economic empowerment programmes saw their support vanish overnight. “For the past year, these adolescent girls and young mothers have received psychosocial support, life-skills education and socioeconomic empowerment, but all these abruptly stopped, and their livelihoods are at risk,” said a representative of Lidar Community Foundation, a youth empowerment programme for orphaned and vulnerable girls in Katutra-Central, Windhoek. The loss of these critical services jeopardizes not only health outcomes but the livelihoods of some of Namibia’s most marginalized individuals.
A fragile civil society left to cope
Namibia’s civil society had long been reliant on external funding, with the US and the Global Fund being major contributors of the civil society-led HIV programmes. The US funding freeze has left civil society organizations working on HIV prevention, human rights and youth empowerment issues in a precarious position, unable to provide essential services and continue operations, forcing them to lay off their staff, scale back their operations, or even completely close their programmes.
This situation is overwhelmingly affecting the most vulnerable and marginalized groups in Namibian society. Key populations—such as transgender people, sex workers, and people living with HIV—were already facing discrimination in accessing essential services. With the end of the US support, these groups are now at an even greater disadvantage. “This is such an emotional time,” said Kholi Buthelezi of the Sisonke National Sex Workers Movement in South Africa. “It triggers memories from that pre-ART times in the HIV era, when all we had was hope but no concrete resources to act on the challenges."
Young women, particularly adolescent girls, are another demographic severely affected by the US funding freeze. Many had been participating in HIV prevention programmes or socio-economic initiatives aimed at empowering them. These cuts have halted progress, leaving them more vulnerable to HIV and other socio-economic challenges.
The need for collective action
A meeting co-hosted by UNAIDS on 7 February to review the implications and impact of the U.S. funding freeze, highlighted the need for collective action to help Namibia’s civil society weather this storm. Many civil society organizations were left unsure of how to engage at the national and international levels to advocate for their cause due to a lack of clear communication and support from the Namibian government. “We wonder if civil society organizations will be consulted on how the country is going to respond to this funding challenge, so that we also contribute to the solutions,” said one participant, highlighting the need for civil society to be closely involved in the response to this unprecedented challenge.
Exploring alternative funding sources, including from the private sector and other partners, was deemed essential. All partners called for a united front, with CSOs coming together not only to advocate for the reversal of the Executive Orders but also to explore ways to ensure continued support for Namibia’s most vulnerable populations.
As a way forward, CSOs were urged to complete a rapid assessment tool to better understand the immediate effects of the funding cuts, as data collection and monitoring are crucial in advocating for the continued support of affected communities and developing detailed action plans and strategies.
Strengthening partnerships, supporting mental health and psychosocial well-being, and engaging with the government are also key to ensuring that Namibia’s civil society could survive in these uncertain times.
Despite all, Namibia’s civil society remains determined. While the challenges are significant, the collective power of advocacy, solidarity, and collaboration offers a glimmer of hope for the future. It is through these unified efforts that Namibia’s most vulnerable communities may continue to receive the care, support, and recognition they deserve.
Region/country
Related

Feature Story
Three Years On: From crisis to prospective recovery
20 February 2025
20 February 2025 20 February 2025Ukraine has been reeling from three years of war since 24 February 2022. One out of two Ukrainians have been affected by the conflict and more than 12 million people need humanitarian assistance and protection while another 6 million have still not been able to return to their homes.
A war-driven economic crisis has severely impacted healthcare funding, putting access to HIV services at risk. With HIV services entirely dependent on external aid and humanitarian support that is becoming increasingly unstable, the uncertainty of the continuity of U.S. funding has further worsened an already dire situation in Ukraine. In January, the new U.S. Administration froze all foreign assistance for a 90-day period. A waiver to allow life-saving services was subsequently issued allowing support for some HIV services.
The U.S. President's Emergency Plan for AIDS Relief (PEPFAR) contributed US$15.6 million to the HIV response in Ukraine during 2023 and 2024. This includes $11 million for antiretroviral therapy and $2 million for various types of rapid test kits, while the rest was used for laboratory expenses.
UNAIDS and partners estimate that 92,840 Ukrainian people could see their HIV treatment disrupted if U.S. funding was to be entirely cut – that is 78% of all people living with HIV on treatment. In addition, stocks of life-saving treatment and HIV prevention drugs are low, with people only getting three versus six months of drug supply.
The threat of a potential financial void left by the U.S. is forcing Ukraine’s health system to search for alternative sources of funding. From Global Fund reprogramming to private sector donations to bulk medicine offers from pharmaceutical companies. Many options are being explored to patch together a lifeline. However, even collectively these efforts may not be enough to fill the PEPFAR gap should the U.S. permanently withdraw its support.
There are hopeful signs of recovery like HIV testing increased 23% last year compared to 2023 but obtaining comprehensive epidemiological and clinical data remains difficult.
This inevitably affects the accuracy of overall assessments due to the ongoing conflict, loss of administrative control in certain regions, missing persons, and mass displacement.
Despite ongoing challenges, Ukraine remains committed to the HIV response, supported by a strong coalition of government, civil society, international organizations, and donors. The UNAIDS Secretariat, Co-sponsors, UN agencies, and member states continue working together to ensure essential services for women, people living with HIV, and key populations, reinforcing the response's sustainability even in the face of adversity.
Related information
Special page
Region/country
Related
 Ukraine: Keeping people in care
Ukraine: Keeping people in care
23 February 2026
 Women, HIV, and war: a triple burden
Women, HIV, and war: a triple burden
12 September 2025
 Displacement and HIV: doubly vulnerable in Ukraine
Displacement and HIV: doubly vulnerable in Ukraine
11 August 2025