



Feature Story
Gervinho meets young people affected by HIV in Gabon ahead of CAN 2017
19 January 2017
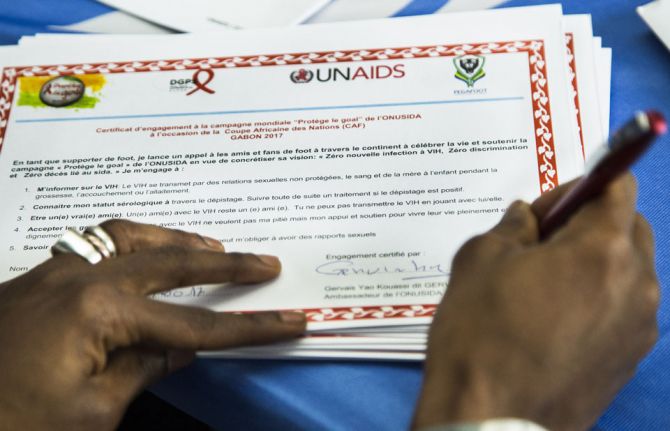
19 January 2017 19 January 2017Travelling to Gabon to attend the Africa Cup of Nations (CAN 2017), Gervais Yao Kouassi (Gervinho), UNAIDS Special Ambassador for Youth and China–Africa Collaboration, visited the UNAIDS office in Libreville, Gabon, to meet some 50 children and young people living with or affected by HIV.
Accompanied by young Gabonese ambassadors for HIV and by artist Charly Tchatch, the animator of the opening of CAN 2017 and an AIDS activist, the international football star talked to the children and young people and listened to their stories and concerns. The children and young people talked about problems with accepting their status and stigma and depression, but also about happiness, love and how they deal with their daily problems.
“I am very touched. It is the first time I hear such poignant testimonies”, said Gervinho. “As you know, I wanted to play with my team here, but I am injured. Your mental strength and joy of life encourages me to face life’s challenges.” Gervinho signed the Protect the Goal campaign ball to support UNAIDS’ vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths at CAN 2017.
Inge Tack, the UNAIDS Country Director, mentioned to Gervinho that despite AIDS budget cuts of 60% in Gabon since 2012, treatment rates have doubled and new HIV infections have been reduced by 30%, while paediatric treatment rates have tripled and coverage of prevention of mother-to-child transmission is at 78%. However, she also noted the need to improve the management of HIV treatment provision to achieve the 90–90–90 targets. “A radical shift in the organization and management of treatment delivery services is required to achieve the 90–90–90 targets in Gabon. Medicines need to be in the centre at all times and services reoriented to better serve patients’ needs,” said Ms Tack.
Gabon experiences persistent treatment stock-outs and poor care services result in no treatment adherence follow-up, no monitoring of drug resistance and no viral load measurement. Ms Tack stressed the need for a decentralized approach for the provision of antiretroviral therapy and an increase in community-led services.
Region/country
Related



Feature Story
Preventing mother-to-child transmission of HIV in coffee producing areas of Guatemala
08 December 2016
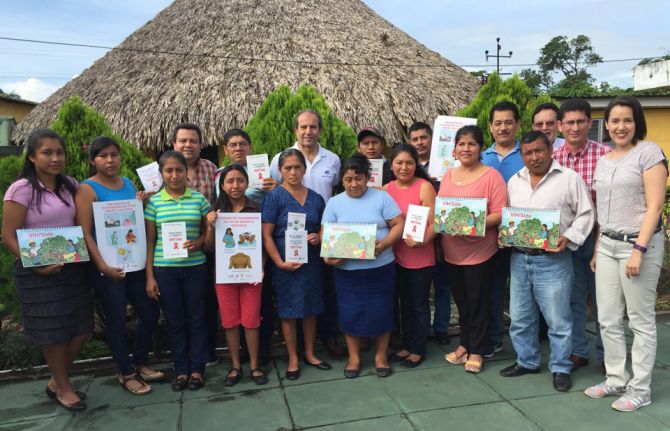
08 December 2016 08 December 2016Preventing mother-to-child transmission of HIV remains one of the major challenges of the AIDS response in Guatemala. In 2015, testing coverage for HIV among pregnant women was 42%. Now, the International Labour Organization (ILO) has teamed up with the Coffee Foundation for Rural Development (Funcafé), the national coffee association, the national AIDS programme and other United Nations agencies, such as UNAIDS and the United Nations Children’s Fund, to promote access to HIV testing, treatment and prevention programmes among women who take up work on plantations during the coffee cutting season.
Seasonal workers employed on coffee plantations often have limited information about HIV and other health issues and restricted access to HIV care and support services. There is also the additional challenge of high levels of mobility and migration among plantation workers. The new programme leverages the network of 16 community health centres established by Funcafé in coffee producing areas of the country’s highlands to provide information related to the prevention of mother-to-child transmission of HIV and to promote the uptake of HIV testing and treatment services for pregnant women.
The project aims to diagnose pregnant women living with HIV and refer them to the official health system for further tests to confirm their status and to start antiretroviral treatment. ILO and its partners provide technical support to train community health workers on providing prevention of mother-to-child transmission of HIV services, bringing HIV treatment and prevention services closer to the people who need them and increasing testing and treatment coverage among pregnant women.
“This is an innovative initiative aimed at strengthening women’s access to prevention of mother-to-child transmission of HIV services by linking the community health system and the national health system and by promoting a multisectoral partnership between the private sector, the Ministry of Health and international partners, with the active participation of communities,” says Ricardo Garcia, UNAIDS Country Director in Guatemala.
Among other aspects, the initiative seeks to train community midwives on HIV prevention and prevention of mother-to-child transmission of HIV on coffee plantations. Midwives play an important role in rural areas as an entry point for pregnant women into the health system. The joint project also aims to raise awareness about HIV prevention and gender equality among male coffee workers and men living in rural areas.
“Workplace settings are an opportunity to provide access to information about HIV prevention tools as well as to promote health, not only among our employees and their families, but in the communities in which we operate, benefiting the entire population,” explains Mynor Maldonado, the Executive Director of Funcafé.
The initiative is part of a wider programme that ILO and UNAIDS have been implementing since 2013. ILO and its partners are exploring similar initiatives with other agribusiness sectors.
Region/country








Feature Story
Czech science exhibition opens at UNAIDS
07 December 2016
07 December 2016 07 December 2016The Permanent Mission of the Czech Republic to the United Nations Office and other International Organizations at Geneva and UNAIDS have opened an exhibition celebrating the contribution that scientists have made to advancing medicine and the treatment of viral diseases such as AIDS. The exhibition, which opened on 6 December, is being held at UNAIDS headquarters in Geneva, Switzerland.
Created by Jáchym Šerých, the exhibition focuses on the work of Czech scientist Antonín Holý, who dedicated his life to developing medicines used to treat HIV, hepatitis B, herpes and other viral diseases. The core of the exhibition is a three-dimensional model of a football symbolizing a fullerene—a molecule of carbon. It captures moments in the private and professional life of Mr Holý.
Speaking at the opening, Vinay P. Saldanha, UNAIDS Regional Director for Eastern Europe and Central Asia, said, “The work of scientists like Antonín Holý transformed the view that being HIV-positive was a death sentence into the reality of a long life with dignity for people living with HIV.”
As of June 2016, 18.2 million people were on antiretroviral therapy in the world, a number that was unthinkable when the epidemic started, more than 30 years ago. No treatment was available at the beginning, but thanks to the tireless work of scientists to find innovative solutions together with communities, medicines were developed to save the lives of people living with HIV.
Jan Kára, Permanent Representative of the Czech Republic, said, “Antonín Holý was a man of vision and strong determination, who made alliances and was pragmatic. His inventions made a difference in fighting viral diseases like AIDS.”
Medicines evolved through time. From eight pills a day in 2001, treatment now involves taking one pill a day. Treatment has saved millions of lives, has improved the health of people living with HIV and has helped prevent the transmission of HIV.
Zdeněk Havlas, Honorary Chair of the Institute of Organic Chemistry and Biochemistry, worked with Mr Holý. He said, “The approval of one medicine is a relatively rare event. Antonín Holý started with antiretroviral medicines in the 1990s and kept on developing other medicines, for example to treat hepatitis B.” By doing so, Mr Havlas said his colleague contributed to “making the lives of millions and millions of people better and even possible.”
What does the future hold? Communities around the world count on scientists to carry on their research to make sure that AIDS is no longer a public health threat. There is hope that a cure and a vaccine for AIDS will be found soon.
Region/country
Related


 Government ensures continuity of treatment in Malawi
Government ensures continuity of treatment in Malawi
10 February 2025








Feature Story
Fruit, condoms and lots of creativity for Geneva World AIDS Day commemoration
05 December 2016
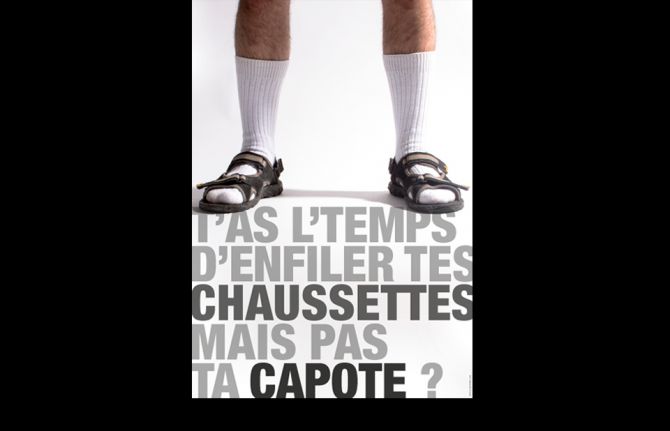
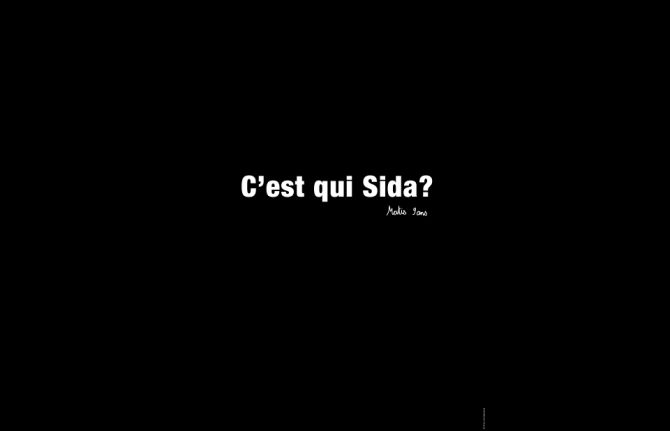
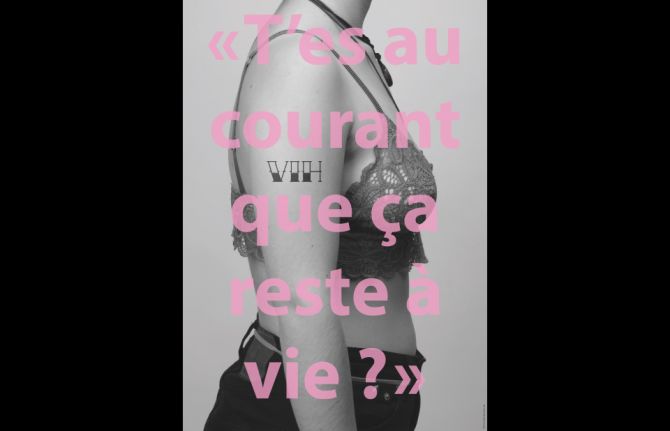
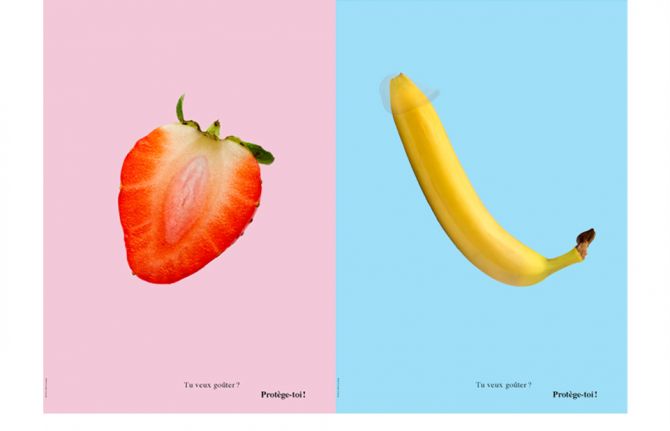
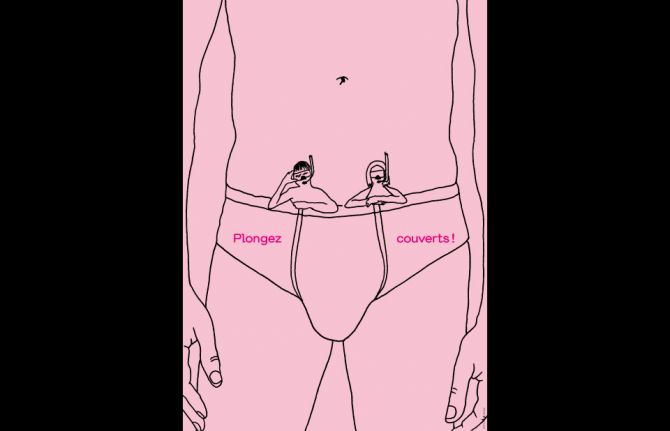
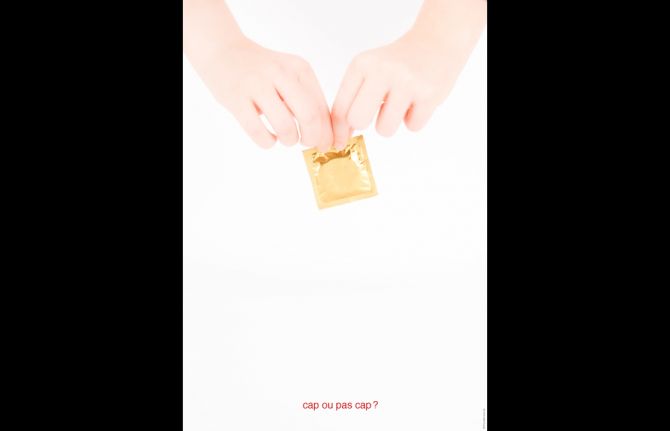
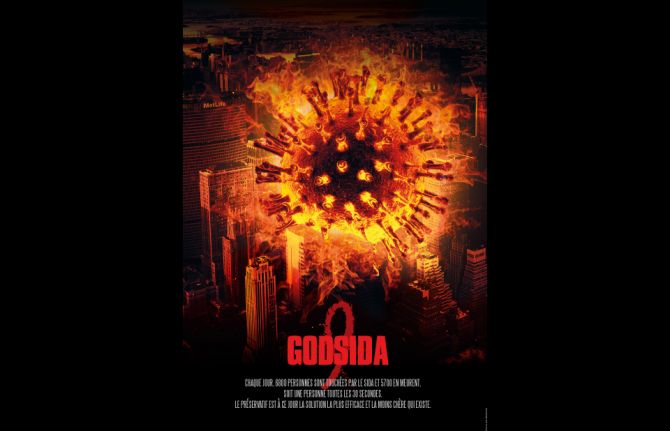
05 December 2016 05 December 2016A sliced strawberry set against a pink background asking, “Do you want to taste? Protect yourself,” a banana with a condom cover stating, “Better this way,” and a drawing of a miniature man and woman with scuba gear surfacing from a man’s underwear with the caption, “Dive covered.” These are some interpretations of what HIV prevention means to students at a Geneva-based professional arts high school.
In the lead-up to this year’s World AIDS Day, UNAIDS joined together with the Centre de Formation Professionnelle Arts (CFP Arts) school to create an art exhibition around the theme of HIV prevention.
Students from the graphic and interactive video departments of the school participated in the project by producing artistic expressions, in the form of posters and videos, around HIV prevention and what it means or how it affects them. This collaboration also helped the students to understand what HIV prevention is and sparked a conversation with a key age group.
The inauguration of the art exhibition took place in the UNAIDS headquarters in Geneva, Switzerland, as part of a World AIDS Day commemoration event. Mariangela Simao, Director of Rights, Gender, Prevention and Community Mobilization at UNAIDS, stressed how important it was to have so many young people present, emphasizing the need to reach out to the next generation.
“This is a day when we come together to remember the many lives lost. It is also a day to celebrate our successes and how far we have come,” she said. “HIV is preventable! We must break the cycle of infection, so we count on you,” added Ms Simao, looking at the students.
The school’s visual arts dean, Judith Behar, explained how CFP Arts enjoyed assigning students projects that serve a purpose beyond the school walls.
“Our students took on the HIV prevention theme with real passion and personal investment because, as they learned, AIDS does concern them.”
The posters and videos will be on display in the UNAIDS building until 18 January 2016.
Poster winners
1st prize to Magali Mühlig for thinking outside the box and sending such a positive message in Héropositive.
2nd prize to Joana Ruiz for encouraging behaviour change with a clear message—one always carries a mobile phone, why not a condom?
3rd prize to Capucine Fernez for the artistic beauty of her drawing, a protected woman or a woman who is well informed, depending on your interpretation.
Felicitations du jury honorary prizes
The uplifting and simplicity of the message by Laura Chappuis.
Sock wearing humour by Loraine Friedli.
The simple, but powerful, message, “Who is Sida?”, by Esaia Girardet.
The tattoo HIV messaging with the caption, “It lasts forever”, by Julie Bertschmann.
Video winners
1st prize to Derek Amez-Droz for his humorous video that is a throwback to the 1980s sexual education videos played in school.
2nd prize to Daniel Chavaz for a lovely drawn animation with a condom as a cape.
3rd prize to Immanuel Nour for the simple and museum-like video.
Felicitations du jury honorary prizes
Jamy Herrmann and Benaiah Finkel for their classical music romantic video encouraging condom use.
Hanaa Joowalay edited a beautiful video that is very artistic.
The fun-loving animation done by Melvyn Frash and Oliver Fehlmann.




Feature Story
Reaching young people in Namibia with sexual and reproductive health services
13 December 2016
13 December 2016 13 December 2016The Namibia Planned Parenthood Association clinic in Windhoek is decorated with colourful murals, its walls brightly painted with red ribbons. It has the feel of a welcoming classroom or youth club rather than a medical site. And that’s the idea, because this facility offers sexual and reproductive health services, including HIV testing and counselling, to adolescents and young people aged up to 25 years old.
The site is staffed by young peer-to-peer counsellors, such as 20-year-old Claudia Ndinundjene, who offers a friendly ear to the clinic’s users and advises them on what to expect from the testing process. She can also give them information on how to protect themselves from unintended pregnancy and HIV and other sexually transmitted infections.
“It’s important for young people to be advised by other young people,” says Ms Ndinunjene, “People need to be helped in a non-judgemental atmosphere that meets their needs—they shouldn’t be asked a lot of questions, but just get the help they need, and quickly.”
The clinic carries out about 200 rapid HIV tests a week. The results are back within 15 minutes. People who test negative are given condoms and advice on how to stay HIV-free. People who test positive are immediately referred to a neighbouring clinic to get access to antiretroviral medicine, which can keep them healthy.
One of the biggest challenges is to get young people to adhere to treatment, especially when long queues translate into long waits at other clinics, which may also be less oriented to the specific needs of young people. That’s why the Executive Director of the clinic, Bravo Linosi, would like to expand services.
“We would like to be able to offer treatment services to the young people who come here as well as HIV testing and counselling,” says Mr Linosi. “This would make a huge difference to young people’s lives, helping them remain healthy by staying on treatment and also helping Namibia to end the AIDS epidemic by 2030.”
The commodities used at the clinic are provided by the government, while funding and other support comes from a range of partners, including UNAIDS and the Global Fund to Fight AIDS, Tuberculosis and Malaria.
The clinic offers Wi-Fi, so that young people can carry on with their homework or simply stay in touch with their friends online while at the clinic. Mr Linosi has plans for pool nights or TV soccer nights to attract more young men to the clinic. In this way, he hopes that HIV testing can become a more routine part of young people’s lives, particularly young men, whose service uptake is currently poor.
The clinic still sees some older adults who have turned 25 but don’t want to go anywhere else, having been visiting the site for several years.
“People feel happy here and they keep coming back to the clinic because they feel safe—that’s why they don’t want to go anywhere else,” says Nelapewa Baumuller, a senior nurse at the clinic.
Region/country


Feature Story
Hands up for #HIVprevention mobilizes support worldwide
05 December 2016
05 December 2016 05 December 2016It started in October with a single message written on one person’s hand: “know your status”. Nine weeks on and thousands of people from all over the world have demonstrated their support for UNAIDS’ “Hands up for #HIVprevention” campaign by sharing photos and videos expressing what HIV prevention means to them. Through a range of content, the campaign highlighted different aspects of HIV prevention week by week and showed how they relate to different groups of people, including adolescent girls and young women, key populations and people living with HIV.
The campaign reached more than 2 million people on Facebook and 64 000 people have engaged through likes, shares and comments. On Twitter, the campaign reached almost 3 million people and UNAIDS campaign tweets were retweeted 12 000 times and liked 9500 times.
Messages that people wrote on their hands and held up for the world to see as part of the campaign include “Use condoms always”, “Provide support”, “End stigma”, “Invest”, “PrEP”, “No violence” and “Gender equality.”
Prominent contributors included the First Lady of Benin, Claudine Talon, the First Lady of China, Peng Liyuan, the First Lady of Guinea-Bissau, Hadja Djene Kaba Condé, the First Lady of Panama, Lorena Castillo de Varella, and Tobeka Madiba Zuma, First Lady of South Africa.
UNAIDS International Goodwill Ambassador Michael Ballack also supported the campaign, with a message in support of zero discrimination. He was joined by James Chau, UNAIDS Goodwill Ambassador for China, Vera Brezhneva, UNAIDS Goodwill Ambassador for Eastern Europe and Central Asia, and Alejandra Oraa, UNAIDS Regional Goodwill Ambassador for Latin America and the Caribbean. The young television star Jenna Ortega provided a powerful and personal message about why HIV prevention was important to her. Princess Tessy of Luxembourg, UNAIDS Global Advocate for Young Women and Adolescent Girls, joined the campaign in the week highlighting women’s empowerment.
UNAIDS partners such as the United Nations Educational, Scientific and Cultural Organization, the United Nations Office on Drugs and Crime, the Global Fund to Fight AIDS, Tuberculosis and Malaria, the President’s Emergency Fund for AIDS relief and mothers2mothers also joined in, offering powerful content and testimonies from people all over the world that showed how innovative programmes are reaching the people most in need of HIV prevention methods.
The campaign followed the launch of the UNAIDS Prevention gap report earlier this year, which showed that an estimated 1.9 million adults have become infected with HIV every year for the past five years and that the number of new HIV infections is rising in some regions. The report shows that HIV prevention efforts must be reinvigorated if the world is to stay on the Fast-Track to ending the AIDS epidemic by 2030.
The campaign culminated in a call for increased investment in HIV prevention strategies targeted at the people and places most in need of them. The commitment made in the 2016 Political Declaration on Ending AIDS is to ensure that financial resources for HIV prevention are adequate and constitute no less than a quarter of AIDS spending globally.
The World AIDS Day Facebook page remains open for new contributions. UNAIDS thanks everyone who has already participated.
Get the message out: AIDS is not over, but it can be.
Hands up for #HIVprevention — World AIDS Day campaign
Related


Feature Story
India announces reaching milestone of 1 million people on HIV treatment
02 December 2016
02 December 2016 02 December 2016Veena has been living with HIV for more than 15 years and works as a community educator in Bangalore, India. But she still remembers the day she learned of her HIV-positive status.
“I was so angry and I cried. I was so fearful and I was suffering,” said Veena, who prefers to be known by her first name. In the early days of her diagnosis she had a lot of health issues and lost weight. She also experienced discrimination from her family.
After starting HIV treatment in 2004, the situation changed for the better. “This medicine is very good and I’m very happy,” Veena said. “My weight increased.”
Now Veena has good relations with her family and is busy with her job and watching her teenage daughter grow into a healthy and engaging adult.
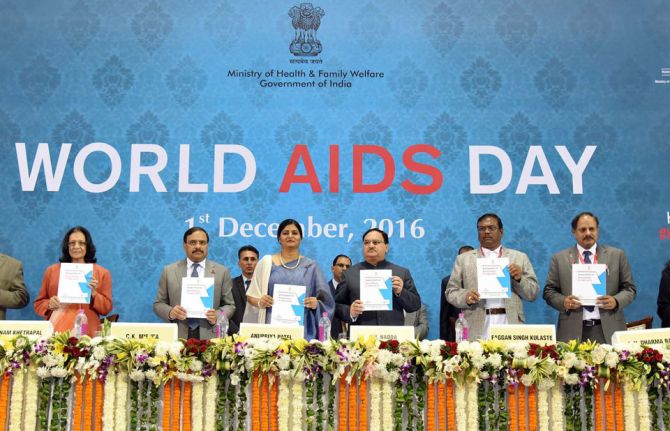
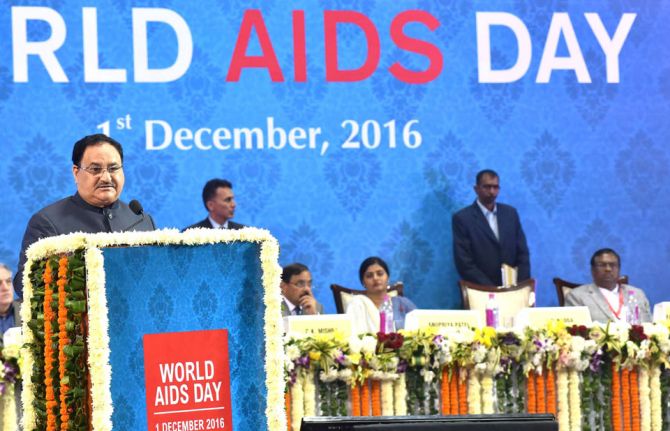
Veena is one of the 1 million people with access to life-saving treatment in India. The Minister of Health and Family Welfare, Jagat Prakash Nadda, made the announcement on treatment at a World AIDS Day event on 1 December in New Delhi. He said, “I am proud to announce the attainment of the milestone of initiation of treatment of the millionth person with free antiretroviral medicines.”
The scale-up in treatment is due to the country’s network of facilities providing HIV services and to greater inclusiveness in India’s policy regarding the eligibility of treatment, which has allowed more people to access antiretroviral medicine. Mr Nadda also announced that India is working towards free treatment for all the estimated 2.1 million people living with HIV in the country.
UNAIDS has congratulated India for this significant achievement. “The Government of India and the community of people living with HIV are to be acknowledged on reaching this important milestone,” said Oussama Tawil, UNAIDS Country Director for India. “The continued participation of communities in all aspects of the AIDS response is critical as India aims to further expand the provision of treatment”, he added.
India has the third largest epidemic in the world. According to the national AIDS programme, annual AIDS-related deaths declined by 54% and new HIV infections dropped by 32% between 2007 and 2015. While acknowledging the overall decline in new HIV infections, Mr Nadda cautioned about the emergence of HIV in new areas. He emphasized the need to re-strategize and to expand the scope of services.
Region/country



Feature Story
Closing the HIV prevention investment gap
28 November 2016
28 November 2016 28 November 2016Despite the progress made against HIV over the past 15 years and the availability of proven prevention and treatment methods, the annual number of new HIV infections among adults has remained static, at an estimated 1.9 million a year since 2010. Moreover, there has been resurgence of new HIV infections among key populations in some parts of the world.
Inadequate investments in prevention and unfocused investments that do not reach the most affected populations and locations are among the reasons for the prevention gap. An analysis of four countries in different regions and with different types of epidemic found that the funding of effective and focused primary HIV prevention programmes was low—6% of total HIV investments in Brazil, 4% in Cameroon, 15% in Myanmar and 10% in South Africa. Country allocations for HIV primary prevention (excluding mother-to-child transmission of HIV and voluntary HIV testing and counselling) by the United States President’s Emergency Plan for AIDS Relief and the Global Fund to Fight AIDS, Tuberculosis and Malaria have accounted for roughly 15% of total HIV expenditure.
With funding for prevention falling behind funding for treatment, fewer than one in five people at higher risk of HIV infection today have access to prevention programmes. UNAIDS modelling has shown that investing around a quarter of all the resources required for the AIDS response in HIV prevention services would be sufficient to make possible a range of prevention programmes, including condom programmes, pre-exposure prophylaxis, voluntary medical male circumcision, harm reduction, programmes to empower young women and girls, and mobilizing and providing essential service packages for and with key populations.
Investing more in prevention will also support treatment programmes to achieve their targets. Prevention programmes—including providing HIV information, condom distribution and outreach to young people and key populations—are often the first entry point for individuals to HIV testing and treatment. Community peer-led prevention programmes are also critical for reducing stigma and discrimination. Meanwhile, expanded access to treatment gives people at higher risk choices and encourages them to find out their HIV status; this, in turn, provides the opportunity to retain people who test negative in ongoing prevention programmes. Reducing the number of people who acquire HIV and will need treatment makes antiretroviral therapy programmes more sustainable.
In December 2015, the UNAIDS Executive Director, Michel Sidibé, called for investing a quarter for HIV prevention. In June 2016, United Nations Member States committed in the 2016 Political Declaration on Ending AIDS to ensuring that financial resources for prevention are adequate and constitute no less than a quarter of AIDS spending globally on average.
A number of countries have already taken action to increase their domestic funding for HIV prevention, including Namibia, which has committed to investing 30% of its HIV budget in preventing HIV among adults and children.
Hands up for #HIVprevention — World AIDS Day campaign
Publications

Feature Story
Youth and innovation shine on World AIDS Day in Algeria
01 December 2016
01 December 2016 01 December 2016A dynamic AIDS response characterized by partnership and passion across all sectors, and prioritizing youth and innovation, was celebrated in Algeria on World AIDS Day.
At a lively World AIDS Day commemoration filled with colour and song held in Algiers, key actors in Algeria’s AIDS response came together to reflect on the county’s successes, consider ongoing challenges and emphasize commitment towards ending AIDS by 2030.
Reacting rapidly to the challenges of HIV, Algeria’s response has consistently prioritized cross-sectoral action, community involvement and evidence and innovation within its strategies and policies. Significant results include a sustained low-level epidemic and free provision of antiretroviral therapy for 90% of people living with HIV.
“Algeria has been a pioneer on AIDS in the region, and the response remains highly dynamic. Continued innovation—particularly through harnessing the power of the young, vibrant population—is maximizing gains made and contributing to broader development and rights outcomes,” said UNAIDS Deputy Executive Director Jan Beagle, who welcomed Algeria as a new member of the UNAIDS governing body, the Programme Coordinating Board, from 2017.
To build on the gains made, Ms Beagle noted areas for increased focus, including: access to services for the prevention of mother-to-child transmission of HIV; greater investment in programmes for key populations; and prioritization of women, girls and young people. “Sustained leadership, integration, evidence and rights-based and people-centred approaches that are adaptable at all stages in the life cycle are needed. Let us build on the progress made and continue to be passionate partners in Algeria’s collective efforts,” she said.
Emphasizing commitment to mobilize an accelerated response towards an AIDS-free generation, Ministry of Health Secretary-General Ali Rezgui said, “Young people are this country’s greatest asset. We must treasure them, listen to them and equip them with education, knowledge and tools to prevent HIV and drive forward Algeria’s AIDS movement.”
“Today we celebrate determination, perseverance and progress driven by a highly multisectoral, inclusive response. This model of joint action is critical for the achievement of the interconnected Sustainable Development Goals,” said Eric Overvest, United Nations Resident Coordinator in Algeria.
Commitment to continued collaboration and dynamism was evident through the active participation of young people at the World AIDS Day celebration. “It’s our dream to protect the world against HIV. With solidarity, prevention and knowledge, together we can end AIDS,” a group of schoolchildren sang loudly and clearly.
Region/country

Feature Story
Viet Nam opens its first opioid substitution therapy service for prisoners
25 November 2016
25 November 2016 25 November 2016“In 2010, I participated in a study visit to learn about prison-based methadone programmes in Spain. Witnessing the positive impacts of the programme on prisoners as individuals and prisons as a whole, I reported the results and recommendations of the visit to the Ministry of Public Security,” said Nguyen Xuan Truong, Chief Prison Officer at Phu Son Prison. “It has been quite a wait since then, but I am happy that Phu Son is the first prison in Viet Nam to provide methadone services for prisoners.”
The launch of the pilot opioid substitution therapy service in Phu Son Prison marks a significant milestone in the efforts of the United Nations Office on Drugs and Crime (UNODC) and the Government of Viet Nam for HIV prevention, treatment and care in Viet Nam’s prisons.
“Since 2009, the United Nations Office on Drugs and Crime has worked with the Government of Viet Nam to provide opioid substitution therapy as part of a comprehensive HIV service package for people who are living and working in prisons,” said Christopher Batt, UNODC Officer-in-Charge.
Opioid substitution therapy is an evidence-informed service for opioid dependence. It reduces opioid use by eliminating withdrawal symptoms and drug craving, decreasing the risk of the transmission of HIV or other bloodborne infections and criminal behaviour. In addition, it integrates the patient into a continuum of care during and after his or her stay in prison.
“The opioid substitution therapy service unit is expected to enhance the quality of life of prisoners, reducing transmission of HIV and other diseases and decreasing the rate of relapse and overdose in prison settings,” Mr Batt added.
The Viet Nam Ministry of Public Security estimates that three out of 10 prisoners use drugs.
Prisoners are at higher risk of becoming infected with HIV or other bloodborne infections, including viral hepatitis B or C, relapse or overdose if their treatment needs are not met.
A second opioid substitution therapy service unit will soon be launched in Thanh Xuan Prison, and there are plans for the service to expand to other prisons.

