Feature Story
Need for scale up in integrated TB and HIV screening to address linked epidemics
24 March 2009
24 March 2009 24 March 2009Although it is mostly preventable and curable, tuberculosis (TB) is one of the leading causes of death among people living with HIV globally. Of the 33 million people who are living with HIV, only 20% of know their status, and only a tiny fraction, 2% in 2007, were screened for TB according to the World Health Organization’s annual report on global TB control launched today.
HIV is dramatically fuelling the TB epidemic in sub-Saharan Africa, where up to 80% of TB patients are co-infected with HIV according to the report. A respiratory infection that spreads like the common cold, TB exploits an immune system already weakened by HIV.
“We have to stop people living with HIV from dying of tuberculosis,” said Mr Michel Sidibe, Executive Director of UNAIDS. “Universal access to HIV prevention, treatment, care and support must include TB prevention, diagnosis and treatment. When HIV and TB services are combined, they save lives.”
"We have to stop people living with HIV from dying of tuberculosis. Universal access to HIV prevention, treatment, care and support must include TB prevention, diagnosis and treatment. When HIV and TB services are combined, they save lives."
Mr Michel Sidibe, Executive Director of UNAIDS
Global Tuberculosis Control 2009 provides an up-to-date assessment of the TB epidemic and progress in controlling the disease. It notes that globally only 16% of TB patients know their HIV status and so the majority of HIV-positive TB patients do not know that they are living with HIV and are not accessing HIV treatment.
However, there has been progress in this area with increased HIV testing among people being treated for TB, especially in Africa. In 2004, just 4% of TB patients in the region were tested for HIV; in 2007 that number rose to 37%, and in some countries (Kenya, Lesotho, Malawi, Rwanda and Swaziland) over 70% of all TB patients know their HIV status.
Because of increased testing for HIV among TB patients, more people are getting appropriate treatment though the numbers still remain a small fraction of those in need. In 2007, 200 000 HIV-positive TB patients were enrolled on co-trimoxazole treatment to prevent opportunistic infections and 100 000 were on antiretroviral therapy.
Need for integrated TB and HIV services
For many years efforts to tackle TB and HIV have been largely separate, despite the overlapping epidemiology. Improved collaboration between TB and HIV programmes will lead to more effective prevention and treatment of TB among people living with HIV and to significant public health gains.
The release of the report today coincides with World TB Day and a 1500-strong gathering at the 3rd Stop TB Partners’ Forum in Rio.

Click on the image to start video
Need for scale up in integrated TB and HIV screening to address linked epidemics
Cosponsors:
Partners:
Feature stories:
ICASA 2008: Collaborative TB and HIV activities essential (03 Dec 2008)
First HIV/TB Global Leaders Forum (09 Jun 2008)
Together against TB and HIV (23 Mar 2007)
UNAIDS interviews UN Special Envoy to Stop TB (21 Mar 2007)
Press centre:
HIV-related TB deaths higher than past estimates (24 March 2009)
External links:
3rd Stop TB Partner's Forum, Rio de Janeiro, Brazil, 23 - 25 March 2009
Publications:



Feature Story
TB/HIV, universal access, and human rights key items on UNAIDS Executive Director’s agenda in Brazil
23 March 2009
23 March 2009 23 March 2009
(from left) Executive Director, UNAIDS Michel Sidibé and Director, Stop TB Department WHO, Dr Mario Raviglione during the press conference launch of Global TB Control 2009, 24 March 2009.
Credit: UNAIDS/D. Ramalho
The Executive Director of UNAIDS, Mr Michel Sidibé, is in Brazil this week promoting greater awareness of the interlinked epidemics of HIV and tuberculosis, the need for universal access to HIV services for all people in need, and the necessity to address stigma and discrimination in Brazil’s response to HIV.
Earlier today in Rio de Janeiro, Mr Sidibé joined the international launch of the World Health Organization’s (WHO) annual report on global TB control.
Although it is mostly preventable and curable, tuberculosis (TB) is one of the leading causes of death among people living with HIV globally. Of the 33 million people who are living with HIV, only 20% of know their status, and only a tiny fraction, 2% in 2007, were screened for TB according to the Global TB Control 2009 report.
"Universal access to HIV prevention, treatment, care and support must include TB prevention, diagnosis and treatment. When HIV and TB services are combined, they save lives."
Michel Sidibé, Executive Director of UNAIDS
“We have to stop people living with HIV from dying of tuberculosis,” said Mr Sidibé. “Universal access to HIV prevention, treatment, care and support must include TB prevention, diagnosis and treatment. When HIV and TB services are combined, they save lives.”

(from left) Assistant Director-General, World Health Organization Dr Hiro Nakatani, Executive Secretary of the Stop TB Partnership, Dr Marcos Espinal; and Executive Director, Global Fund to Fight AIDS, TB and Malaria, Dr Michel Kazatchkine during the press conference launch of Global TB Control 2009, 24 March 2009.
Credit: UNAIDS/D. Ramalho
The UNAIDS Executive Director was joined at the launch by the Executive Director of the Global Fund to Fight AIDS, Tuberculosis and Malaria, Dr Michel Kazatchkine, the Assistant Director-General of the HIV/AIDS, TB, Malaria and Neglected Tropical Diseases Department at WHO, Mr Hiroki Nakatani, the Director of the Stop TB Department, Dr Mario Raviglione, and the Executive Secretary of the Stop TB Partnership, Dr Marcos Espinal.
The report launch is part of World TB Day events taking place during the 3rd Stop TB Partners Forum, which opened in Rio de Janeiro on 23 March. Mr Sidibé will deliver an address at the Forum’s closing on 25 March.
Later in the week, Mr Sidibé will travel to Brasília where he will meet with senior Government of Brazil officials including the National Congress Parliamentary group on HIV and the ministers for foreign affairs, women’s policies, health, and human rights, respectively.
To amplify UNAIDS’ messages of standing with people living with and affected by HIV and stopping laws that block the AIDS response, Mr Sidibé will meet with several key civil society actors active in promoting HIV awareness, protecting human rights, and ending stigma and discrimination, especially for those most vulnerable to HIV. One meeting will bring together national level representatives of groups representing people living with HIV, youth, women, and lesbians, gays, bisexuals and transgenders to discuss these issues within the national and local context.
In Rio de Janeiro, visits are planned to organizations providing vital services to children and young people. One such organization is Sociedade Viva Cazuza, a non-profit that supports children, young people and adults living with HIV through a broad range of services, from HIV counselling and testing to the administration of antiretroviral treatment under the auspices of Rio de Janeiro’s municipal health care system. Besides physical support, Sociedade Viva Cazuza also maintains a website where people can pose their HIV and other sexual health questions to experts.
In Latin America, Brazil has the region’s largest HIV epidemic, home to more than 40% (730,000) of people living with the virus, followed by Mexico with 200,000 HIV-positive people. But the country also benefits from a commitment to ensuring access to both HIV prevention and treatment services, which has helped keep its epidemic stable and halved AIDS mortality rates between 1996 and 2002.
On 30 March, Mr Sidibé will join the Brazilian Minister of Women’s Policies, Ms Nilcéa Freire, in inaugurating the first centre that focuses on rehabilitating men who abuse women. Located in Nova Iguaçu, a municipality in Rio de Janeiro, the centre will place emphasis on education programmes to put a stop to domestic violence. Ten other centres are planned for the country.
Mr Sidibe will conclude his official visit later that day by addressing delegates at the opening of the Global Symposium on Engaging Men and Boys in Gender Equality.
This is Mr Sidibé’s first official visit to Brazil since becoming executive director of UNAIDS.
TB/HIV, universal access, and human rights key items on UNAIDS Executive Directo
Cosponsors:
Partners:
Multimedia:
Feature stories:
Need for scale up in integrated TB and HIV screening to address linked epidemics (24 March 2009)
Press centre:
HIV-related TB deaths higher than past estimates (24 March 2009)
External links:
Feature Story
Swing and Sisters: HIV outreach to sex workers in Thailand
19 March 2009
19 March 2009 19 March 2009
Michel Sidibé, Executive Director of UNAIDS visited workers from two organizations to get first hand experience of how they carry out their outreach work among Pattaya’s sex work community.
Credit: UNAIDS/Vinai Dithajohn
Picking her way through the crowds Surang Janyan waves a friendly hello to her friend Gop. This is one of the many people she will meet tonight in Pattaya’s Walking Street – a long street running along the cost of one of Thailands red light areas.
Surang Janyam is the Founder and Director of Swing, a small organization which provides support for sex workers in Thailand. She regularly visits Gop around midnight to check whether she or her staff need anything. Gop is the owner of one of Pattaya’s most popular bars, the Wild West Boys, where men go to watch a show and pay to spend time with the male sex workers, in the bar or for sexual services in private.
Gop has around 70 sex workers working for her and Surang knows many of them well. “Swing workers come to talk to us and give us condoms,” said Gop. “And they show the boys how to use them properly.” Swing members and volunteers distribute several thousand condoms each month and provide information about HIV and how to protect themselves against the virus.
"HIV among sex workers and access to services are among the biggest challenges to the AIDS response in Thailand. It is extremely important that sex workers gain access to HIV prevention and treatment services without fear of discrimination."
Michel Sidibé, Executive Director of UNAIDS
“HIV among sex workers and access to services are among the biggest challenges to the AIDS response in Thailand,” said Michel Sidibé, Executive Director of UNAIDS. “It is extremely important that sex workers gain access to HIV prevention and treatment services without fear of discrimination.”
Swing works with a lot of bars and bar owners particularly. “Gaining the confidence of the bar owners is an important entry point for gaining access to the sex workers themselves,” said Patrick Brenny, UNAIDS Country Coordinator in Thailand. “Knowledge about HIV is worryingly low among sex workers in Thailand, at around 28% and it is important that they receive education about how to protect themselves and their clients.” Further down the Street Surang meets another of her friends Nueng who works for Sisters, the first counselling service in Thailand to cater exclusively for the transgender community. Pattaya is home to around 1000 transgenders in high season.
“We set up the centre in 2005 to get public support and greater acceptance of the transgender community in Pattaya,” said Nueng who is the Sisters Outreach Supervisor. “Before we started the transgender community had nowhere to go and no one to turn to for advice and support. There were services for male and female sex workers but nothing for transgender, we were on our own and people didn’t understand us.”
Pattaya, became the favourite ‘rest and recreation’ place of US troops during the Vietnam war and has since become a well trodden path on the sex tourism trail drawing in thousands of visitors a year.
Sisters, like Swing runs a drop-in centre in Pattaya where they provide medical services, counselling, skills development as well as club activities such as make-up, sports and cooking.
Nueng is transgender herself and so understands the stigma and discrimination faced by the transgender sex workers. “We have many problems because we are transgender,” she said. “If we try to access health services staff are often very unkind to us and treat us unfairly. So we try to offer our transgender sisters support and broaden awareness in the community so that people will accept us.”
Nueng wears a T-shirt the group printed for themselves so that they can be easily recognised when they carry out their outreach work. The T-shirts are bright pink and carry the words ‘Sisters, where our second home is.’
Michel Sidibé, Executive Director of UNAIDS visited workers from the two organizations this week to get first hand experience of how they carry out their outreach work among Pattaya’s sex work community. Working in partnership with sex workers to identify their needs and to advocate for policies and programmes that improve their health, safety and engagement in the AIDS response is a proven strategy and an essential feature of UNAIDS approach.
Swing and Sisters: HIV outreach to sex workers in Thailand
Multimedia:
Feature stories:
UNAIDS Executive Director visits Thailand (17 March 2009)
Asia Pacific Leadership Forum meets (19 March 2009)
Publications:
UNAIDS Guidance Note on HIV and Sex Work (pdf, 238 Kb)



Feature Story
Condoms and HIV prevention: Position statement by UNAIDS, UNFPA and WHO
19 March 2009
19 March 2009 19 March 2009[Originally published in 2004 updated in 2009]

Condom use is a critical element in a comprehensive, effective and sustainable approach to HIV prevention and treatment.
Credit: UNAIDS
Condom use is a critical element in a comprehensive, effective and sustainable approach to HIV prevention and treatment. Prevention is the mainstay of the response to AIDS. Condoms are an integral and essential part of comprehensive prevention and care programmes, and their promotion must be accelerated. In 2007, an estimated 2.7 million people became newly infected with HIV. About 45% of them were young people from 15 to 24 years old, with young girls at greater risk of infection than boys.
The male latex condom is the single, most efficient, available technology to reduce the sexual transmission of HIV and other sexually transmitted infections.
The search for new preventive technologies such as HIV vaccines and microbicides continues to make progress, but condoms will remain the key preventive tool for many, many years to come. Condoms are a key component of combination prevention strategies individuals can choose at different times in their lives to reduce their risks of sexual exposure to HIV. These include delay of sexual initiation, abstinence, being safer by being faithful to one’s partner when both partners are uninfected and consistently faithful, reducing the number of sexual partners, correct and consistent use of condoms(1), and male circumcision.
Conclusive evidence from extensive research among heterosexual couples in which one partner is infected with HIV shows that correct and consistent condom use significantly reduces the risk of HIV transmission from both men to women, and also from women to men(2). Laboratory studies show that male latex condoms are impermeable to infectious agents contained in genital secretions(3). To ensure safety and efficacy, condoms must be manufactured to the highest international standards. They must be procured according to the quality assurance procedures established by the WHO, UNFPA and UNAIDS and they should be stored away from direct heat sources. Prevention programmes need to ensure that high-quality condoms are accessible to those who need them, when they need them, and that people have the knowledge and skills to use them correctly.
Condoms must be readily available universally, either free or at low cost, and promoted in ways that help overcome social and personal obstacles to their use.
Condom use is more likely when people can access them at no cost or at greatly subsidized prices. Effective condom promotion targets not only the general population, but also people at higher risk of HIV exposure, especially women, young people, sex workers and their clients, injecting drug users and men who have sex with men. UNFPA estimates that the current supply of condoms in low- and middle-income countries falls well short of the number required (the condom ‘gap’)(4). Despite the gap, international funding for condom procurement has not increased in recent years. Collective actions at all levels are needed to support efforts of countries, especially those that depend on external assistance for condom procurement, promotion and distribution.
HIV prevention education and condom promotion must overcome the challenges of complex gender and cultural factors.
Young girls and women are regularly and repeatedly denied information about, and access to, condoms. Often they do not have the power to negotiate the use of condoms. In many social contexts, men are resistant to the use of condoms. This needs to be recognized in designing condom promotion programmes. Female condoms can provide women with more control in protecting themselves. However, women will remain highly vulnerable to HIV exposure, until men and women share equal decision-making powers in their interpersonal relationships.
Condoms have played a decisive role in HIV prevention efforts in many countries.
Condoms have helped to reduce HIV infection rates where AIDS has already taken hold, curtailing the broader spread of HIV in settings where the epidemic is still concentrated in specific populations.
Condoms have also encouraged safer sexual behaviour more generally. Recent analysis of the AIDS epidemic in Uganda has confirmed that increased condom use, in conjunction with delay in age of first sexual intercourse and reduction of sexual partners was an important factor in the decline of HIV prevalence in the 1990s(5). Thailand’s efforts to de-stigmatize condoms and its targeted condom promotion for sex workers and their clients dramatically reduced HIV infections in these populations and helped reduce the spread of the epidemic to the general population. A similar policy in Cambodia has helped stabilize national prevalence, while substantially decreasing prevalence among sex workers. In addition, Brazil’s early and vigorous condom promotion among the general population and vulnerable groups has successfully contributed to sustained control of the epidemic.
Increased access to antiretroviral treatment creates the need and the opportunity for accelerated condom promotion.
The success of antiretroviral therapy in industrialized countries in reducing illness and prolonging life can alter the perception of risk associated with HIV(6). A perception of low-risk and a sense of complacency can lead to unprotected sex through reduced or non-consistent condom use. Promotion of correct and consistent condom use within antiretroviral treatment programmes, and within reproductive health and family planning services, is essential to reduce further opportunities for HIV transmission. Rapid scale-up of HIV testing and counselling is needed to meet the prevention needs of all people, whether they are HIV-positive or negative.
1 UNAIDS. 2004 Report on the global AIDS epidemic, page.72.
2 Holmes K, Levine R, Weaver M. Effectiveness of condoms in preventing sexually transmitted infections. Bulletin of the World Health Organization. Geneva. June 2004.
3 WHO/UNAIDS. Information note on Effectiveness of Condoms in Preventing Sexually Transmitted Infections including HIV. Geneva. August 2001.
4 UNFPA. 2007 report on donor support for contraceptives and condoms for STI/HIV prevention 2007.
5 Singh S, Darroch J.E, Bankole A. A,B, and C in Uganda: The Roles of Abstinence, Mongamy and Condom Use in HIV Decline. The Alan Guttmacher Institute. Washington DC. 2003.
6 Gremy I, Beltzer N. HIV risk and condom use in the adult heterosexual population in France between 1992 and 2001: return to the starting point? AIDS 2004;18:805-9.
Condoms and HIV prevention: Position statement by UNAIDS, UNFPA and WHO
Cosponsors:
Press centre:
UNAIDS promotes combination HIV prevention towards universal access goals (18 March 2009)
Download printable version (pdf, 54 Kb)
Feature stories:
UNAIDS Executive Director visits Thailand (17 March 2009)
Asia Pacific Leadership Forum meets (19 March 2009)
Publications:
Best practice: Making condoms work for HIV prevention (pdf, 1.1 Mb)

Feature Story
Asia Pacific Leadership Forum meets
19 March 2009
19 March 2009 19 March 2009The 7th Steering Committee of the Asia Pacific Leadership Forum met today in the Thai capital Bangkok to discuss progress made and to design ways forward for work on HIV in the region.
The meeting was opened by the Executive Director of UNAIDS Mr Michel Sidibé who encouraged the leaders to focus on partnership building for a truly comprehensive response to the epidemic.
Lady Roslyn Morauta, the Australian Ambassador on HIV chaired the meeting and gave opening remarks about the actions taken on the recommendations made at the 6th APLF Steering Committee meeting.
The steering committee meets once a year to review progress and provide guidance on future strategies and activities for leadership mobilisation. The APLF works primarily at country level through the UNAIDS country offices which in turn work in partnership with government, civil society groups and the private sector to further the AIDS response in Asia Pacific.
At the invitation of the Thai Government, UNAIDS Executive Director Mr Michel Sidibé has spent the week in Thailand meeting government and civil society partners. During his stay Mr Sidibé also met with the Prime Minister of Thailand Abhisit Vejjajiva.
Asia Pacific Leadership Forum meets
Feature stories:
UNAIDS Executive Director visits Thailand (17 March 2009)
Swing and Sisters: HIV outreach to sex workers (19 March 2009)
Feature Story
UNAIDS Executive Director visits Thailand
16 March 2009
16 March 2009 16 March 2009
UNAIDS Executive Director Mr Michel Sidibé (left) with the Prime Minister of Thailand.
Credit: Gov. of Thailand
At the invitation of the Thai Government, UNAIDS Executive Director Mr Michel Sidibé is in Thailand this week to discuss progress in the response to AIDS and visit projects to get a better understanding of how HIV prevention and treatment efforts are making a difference to peoples lives.
Today in Bangkok Mr Sidibé hosted a meeting with civil society partners in the region. In his meeting with national and regional civil society partners, discussions took place on closer collaboration to further the AIDS response.
During his stay Mr Sidibé will meet with the Prime Minister as well as Ministers of Public Health, Interior and Foreign Affairs. Thailand is recognized as a visionary leader in the AIDS response, particularly in scaling up services to prevent the transmission of HIV from mothers to their children. The country also has expertise on HIV counselling and testing and on sexual and reproductive health services for young people which will be one of the topics that Mr Sidibé will be discussing in detail with the Minister of Public Health.

During his country visit to Thailand, UNAIDS Executive Director, Michel Sidibé met with representatives from the Thai and Regional Civil Society, Bangkok, 17 March 2009.
Credit: UNAIDS/P. de Noirmont/Asiaworks
Later in the week Mr Sidibé will visit the seaside resort of Pattaya where an HIV prevention outreach project is aiming to improve the health of the local men, women and transgendered who sell sex to tourists. Pattaya, once a quiet fishing village, is now a magnet for “sex tourism” drawing people from all over the world to buy sex.
Mr Sidibé will conclude his official visit by addressing Asian leaders at the opening of the Asia Pacific Leadership Forum.
This will be Michel Sidibé’s first official visit to Asia since becoming executive director of UNAIDS.
UNAIDS Executive Director visits Thailand
Multimedia:
Feature stories:
‘Positive partnerships’ break down AIDS-discrimination in Thailand (30 March 2006)
Swing and Sisters: HIV outreach to sex workers in Thailand (19 March 2009)
Asia Pacific Leadership Forum meets (19 March 2009)
Publications:
UNAIDS Guidance note on HIV and sex work (pdf, 239 Kb)
Feature Story
3% of US capital city living with HIV
16 March 2009
16 March 2009 16 March 2009
The District of Columbia HIV/AIDS Epidemiology Update 2008 report.
At least 3% of residents in Washington D.C. are living with HIV according to a report published today by US health officials at the District of Columbia's HIV/AIDS Administration.
The leading mode of transmission of HIV in the district is men having sex with men. Heterosexual transmission and injecting drug use closely follow, the report says.
"Today’s findings by US health officials show that there is no room for complacency in responding to HIV. We must continue to learn from each other and work together - both in developing and high-income countries – to ensure universal access to HIV prevention, treatment, care and support services for citizens."
Paul de Lay UNAIDS Deputy Executive Director, Programme, ad interim and Director of Evidence, Monitoring and Policy
“Today’s findings by US health officials show that there is no room for complacency in responding to HIV,” said Paul de Lay UNAIDS Deputy Executive Director, Programme, ad interim and Director of Evidence, Monitoring and Policy.
“We must continue to learn from each other and work together - both in developing and high-income countries – to ensure universal access to HIV prevention, treatment, care and support services for citizens.”
The District of Columbia HIV/AIDS Epidemiology Update 2008 reports that HIV is found in all demographics in Washington: more than 4% of African-Americans, almost 2% of Latinos and 1.4% of Caucasians are living with HIV. However African-American men are disproportionably affected, accounting for 76% of people living with HIV.
This follows the broader pattern across the United States where racial and ethnic minorities are disproportionately affected by the HIV epidemic. Although African Americans represent about 13% of the population (US Census Bureau, 2006), in 2005 they accounted for 48% of new HIV diagnoses.
The United States of America has one of the largest HIV epidemics in the world, with an estimated 1.2 million people living with HIV in 2007 (UNAIDS, 2008).
3% of US capital city living with HIV
Publications:
District of Columbia HIV/AIDS Epidemiology Update 2008 (pdf, 12.36 Mb)
Related



Feature Story
New HIV Indicator Registry improves access to high-quality indicators
13 March 2009
13 March 2009 13 March 2009UNAIDS announces the launch of a central repository of information on indicators used to track the response to the HIV epidemic. Through the Indicator Registry, professionals in monitoring and evaluation, for the first time ever have access to the complete definitions of all key indicators in one central database.
Coordinated monitoring and evaluation approaches are crucial to generating reliable and timely information on the AIDS epidemic and the response across countries and regions. The use of standardized definitions and indicators supports countries in measuring their way towards universal access to HIV prevention, treatment, care and support as well as in taking evidence-informed action and ensuring accountability.
The registry allows its users to select appropriate indicators to monitor a country’s epidemic and response and specifically highlights the harmonized indicators that have been endorsed by a wide range of multilateral agencies and international organizations.
A valuable resource for country monitoring
The Indicator Registry is a unique and highly versatile database. Key target audience of the Indicator Registry are national AIDS authorities in the process of defining or reviewing the monitoring and evaluation plan for their national response to HIV, as well as implementers monitoring their HIV programmes. By using the registry, countries are able to:
- access information on the full range of indicators available,
- select appropriate indicators for the country’s epidemic and the response,
- manage and share their country specific set of indicators,
- use standards tools for development of new indicators when needed,
- export indicator definitions to PDF, Word, Excel or SDMX for data collection by applications such as the Country Response Information System (CRIS).
The tool not only allows benchmarking of existing indicators, but can be applied to newly created indicators to ensure that the highest quality information is being collected. Integration of standards tool with the Indicator Registry is an unprecedented step to improve the quality and consistency of indicators used in HIV.
Additional features will be added in the coming year including independent rankings of the indicators, using a new Indicator Standards Tool developed by a technical working group of the UNAIDS Monitoring and Evaluation Reference Group (MERG), which includes representatives from various UN agencies, bilateral donors, country representatives and civil society.
The development of the indicator registry was a multi-agency effort with support from the World Health Organization, UNICEF, the Global Fund to Fight AIDS, Tuberculosis and Malaria, the U.S. President’s Emergency Plan for AIDS Relief, and the UNAIDS Secretariat and guided by the MERG that sets standards for indicators and their use.
For access to the Indicator Registry, go to: www.indicatorregistry.org
For more information, you may contact Mr. Taavi Erkkola (erkkolat@unaids.org).
New HIV Indicator Registry improves access to high-quality indicators
Cosponsor:
World Health Organization
UNICEF
Partners:
The Global Fund to Fight AIDS, Tuberculosis and Malaria
The U.S. President’s Emergency Plan for AIDS Relief
Contact:
By email to Mr Taavi Erkkola: erkkolat@unaids.org
External links:
UNAIDS Monitoring and Evaluation Reference Group (MERG)
Tools:
Related

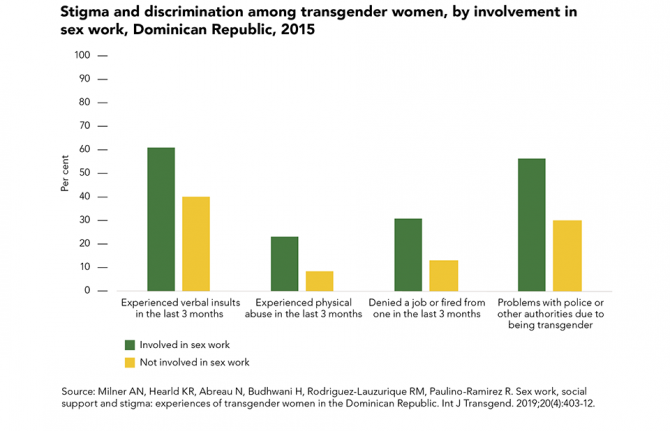 Transgender sex workers face frequent abuse
Transgender sex workers face frequent abuse
29 March 2022
 Many key populations avoid health services
Many key populations avoid health services
21 February 2022
Feature Story
Greater action needed to protect women’s inheritance and property rights in the face of HIV
13 March 2009
13 March 2009 13 March 2009
Elizabeth Mataka, UN Special Envoy for HIV/AIDS in Africa.
Credit: UNDP
If more women are to avoid HIV infection, laws on inheritance and property rights should be revisited, revised or better enforced. This was one of the key messages emerging from a high-profile side-event on women’s inheritance, land and housing rights in the context of HIV, which took place yesterday, 12 March, during the 53rd session of the Commission on the Status of Women held at UN Headquarters in New York.
The discussion brought together a range of speakers including Elizabeth Mataka, UN Special Envoy for HIV/AIDS in Africa and Rose Gawaya, Senior Gender Adviser of the UNDP HIV/AIDS Practice based in Johannesburg, South Africa. The event focused on reviewing innovative work that has been done to increase women’s access to, control over, and ownership of land and housing in a bid to mitigate the impact of AIDS. Realistic and workable strategies, from the grassroots to international level, were explored.
"Lack of equal rights for women to inheritance and property excludes women from accessing resources that would help reduce their vulnerability to HIV and improve their ability to cope with the consequences of the epidemic."
Elizabeth Mataka, UN Special Envoy for HIV/AIDS in Africa
Ms Mataka highlighted the increased vulnerability of women due to AIDS and called on governments to harmonise often conflicting laws and legislation. She said “Lack of equal rights for women to inheritance and property excludes women from accessing resources that would help reduce their vulnerability to HIV and improve their ability to cope with the consequences of the epidemic.”
The issue of such rights for women is of critical importance in addressing HIV. When a woman’s husband dies from AIDS, she might lose her home and land, inheritance and livelihood. This can leave her in a situation where she is forced to enter into relationships and behaviours that render her more vulnerable to the virus. The panellists contended that when women have enhanced access to ownership and control of land and property rights they have a greater range of choices, are far more able to exercise autonomy and, ultimately, are better able to protect themselves.
As well as the revision or implementation of existing laws on inheritance, the panellists recommended increased access to information and legal experts, enhanced partnerships among organizations working in the area and strengthened networks to raise awareness of the issues, with a focus on grassroots women as critical drivers of change. They also suggested greater use of the media and creative ways of sharing and packaging messages, while highlighting the need to increase the scope of research.
Other participants in the panel included: Jeanmarie Fenrich, Fordham Leitner Centre for International Law and Justice; Seodi White, Women and Law in Southern Africa (Malawi); Esther Mwaura, GROOTS Kenya, Huairou Commission; and Anne Gathumbi, Open Society Initiative for East Africa, Law and Health Initiative.
This event was organized by UNDP, the Huairou Commission and Soros/OSI with support from UNAIDS, GROOTS, ICRW, COHRE, Fordham Law Leitner Center and WLSA Malawi.
Greater action needed to protect women’s inheritance and property rights in the
Cosponsors:
Partners:
Fordham Leitner Centre for International Law and Justice
Women and Law in Southern Africa
Huairou Commission
Open Society Initiative for East Africa
The Global Coalition on Women and AIDS
Feature stories:
Commission on the Status of Women opens with call for action to achieve universal access and gender equality (02 March 2009)
UN Special Envoy for AIDS in Africa Elizabeth Mataka (15 September 2009)
External links:
Commission on the Status of Women 53rd Session
Official documentation
Publications:
An Analysis of the Gender Policies of the Three Major AIDS Financing Institutions: The Global Fund to Fight AIDS, Tuberculosis and Malaria, the World Bank and the President’s Emergency Plan for AIDS Relief (pdf, 166 Kb)
UNIFEM fact sheets on gender-related aspects of AIDS (pdf, 311 Kb)


.")
Feature Story
Injecting drug use and HIV: Interview with UNAIDS Team Leader, Prevention, Care and Support team
12 March 2009
12 March 2009 12 March 2009The Commission on Narcotic Drugs (CND) is meeting at the United Nations Office in Vienna for its 52 session, from 11-20 March 2009. At this session, governments will assess the progress achieved in meeting the goals defined in the 1998 UN General Assembly Special Session on Illicit Drugs.
In an interview, Mr Michael Bartos, UNAIDS Team Leader, Prevention, Care and Support team, shares his thoughts on the Commission’s progress in addressing the link between injecting drugs and HIV.
The 52nd session of the Commission on Narcotic Drugs is taking place 11 years after the landmark UN General Assembly Special Session on Illicit Drugs in 1998. Where are we today in addressing the links between HIV and drug use?
This year’s session of the Commission on Narcotic Drugs (CND) in Vienna marks ten years plus a year of reflection since the 1998 UN General Assembly Special Session on Illicit Drugs. The Commission and its high-level ministerial segment will be looking at progress made since 1998, the current situation and the next steps in the response to the global drug problem.
HIV is only one of the many aspects of the global drug problem. At the CND it is considered in the context of “demand reduction” where members will consider how to deal with both direct harms to drug users and the associated harms which include HIV.
"We are now very well aware of the central link between HIV and injecting drug use, and aware that the nexus has to be broken if we’re really to have any hope of getting HIV as an epidemic under control in many parts of the world."
Michael Bartos, UNAIDS Team Leader, Prevention, Care and Support team
Since 1998 we have become much more conscious of the intertwined nature of the epidemics of drug use and HIV. In 1998 we were already able to see the extent to which HIV had been transmitted among injecting drug users, and we were aware of the fact that injecting drug use was a very efficient way for HIV to spread across the countries. But at that stage the extent of the potential problem was not yet fully in view. For example the Russian HIV epidemic —which is largely driven by injecting drug use— had very few HIV cases before the beginning of the 90s. We now talk about Russia having one million HIV cases. The reality is that the decade of the 90s saw the explosive growth of HIV amongst injecting drug users in Russia and in a number of other countries.
So we are now very well aware of the central link between HIV and injecting drug use and aware that the nexus has to be broken if we’re really to have any hope of getting HIV as an epidemic under control in many parts of the world.
What are some of the key challenges in responding to the issues of HIV and drug use?
There are a series of challenges to properly addressing HIV amongst injecting drug users. The first is that in most countries injecting and other drug use are illegal. Therefore these behaviours and the ways they are controlled fall under the authority of the police.
This is an issue in relation to HIV as the most effective prevention strategies are those which include the people who are most affected. It has been very difficult for people who inject drugs to argue that they can, should, and indeed must, be part of the solution to AIDS and not viewed simply as part of the problem and thrown into prison or treatment camps.
Injecting drug users can find themselves marginalized in most social responses, including the responses to HIV. A considerable challenge is how to assist people who use drugs access HIV services and how to assist organizations who help provide services to people who use drugs, including HIV services.
Can law enforcement agencies and AIDS organizations work together?
Some real achievements have been made when law enforcement authorities and people who use drugs have found a common cause working together to deal with the harms associated with injecting drug use. That’s one of the things that we need to focus on: the ways in which positive policing can support AIDS response.
What will UNAIDS highlight at the Commission on Narcotic Drugs?
At the Commission on Narcotic Drugs UNAIDS wants to draw attention to the scale of the problem. There is virtually no country in the world where there aren’t at least some people who inject drugs. Recent estimates, constructed under the auspices of the reference group to the United Nations system on injecting drug use, show around 16 million drug users across the world, an estimated 3 million are living with HIV. That’s quite a considerable part of the global HIV epidemic. In fact 30% of the global HIV epidemic outside sub-Saharan Africa is among injecting drug users.
"Many IDUs are excluded from HIV treatment programmes because those running the programmes assume that people who use drugs would be unable to take their HIV treatment regularly."
Michael Bartos, UNAIDS Team Leader, Prevention, Care and Support team
But even more important than drawing attention to the scale of the problem is moving the focus to the scale of the response needed. A number of countries around the world are moving to full scale implementation of harm reduction services to deal with HIV amongst people who inject drugs.
These services include access to opioid substitution therapy such as methadone and buprenorphine services as a way drug users can be assisted to deal with their addiction. Other services include access to drug treatment and sexual health services, condoms and access to antiretroviral therapy for HIV for those drug users who need it.
Many IDUs are excluded from HIV treatment programmes because those running the programmes assume that people who use drugs would be unable to take their HIV treatment regularly.
Needle and syringe exchange services have proven to be effective in ensuring that drug injectors do not share contaminated equipment—which is a very efficient way of passing on the virus.
A number of countries are scaling up access to this full range of services. Impressive work has been done by countries such as Indonesia. Malaysia has made high level commitments to address these questions among its population. China has been very seriously addressing the way in which can fully scale up its package of services in relation to HIV and injecting drug use. The same has applied to many parts of India, and Bangladesh which have also made some impressive commitments. So particularly in east and south-east Asia there have been some strong developments. Also In eastern Europe and central Asia there have been signs that the most successful national responses to HIV amongst IDUs are looking to provide these services at full scale.
Do you anticipate the Commission on Narcotic Drugs at this session to make some headway on harm reduction? What needs to be done, politically speaking, to get harm reduction on Member States’ agenda?
"It has been very difficult for countries around the world to get the right balance—or to come to consensus on how to balance— the twin desires of getting people to not use drugs and also reducing the harms associated with drug use."
Michael Bartos, UNAIDS Team Leader, Prevention, Care and Support team
The Declaration of Commitment on HIV/AIDS adopted by the UN General Assembly Special Session on HIV/AIDS in 2001 makes a clear commitment to the range of harm reduction approaches. This was then repeated by the General Assembly in its 2006 Political Declaration on AIDS. However, the phrase “harm reduction” in the context of “drug control” which is reflected in the Commission on Narcotic Drugs, remains a contested term.
Apart from a question of terminology, harm reduction is also contested on a substantive level. It has been very difficult for countries around the world to get the right balance—or to come to consensus on how to balance— the twin desires of getting people to not use drugs and also reducing the harms associated with drug use.
I think that there is a strong sense across the world that a public health approach, a harm reduction approach, is the more prominent perspective in the global discourse. However it still hasn’t found its expression in the policies of a number of countries.
We have a situation where in some countries the national drugs authorities who consider questions of drug use and HIV may not even know what their counterparts in the national health and AIDS authorities are doing in relation to their response to HIV amongst IDUs.
One of the priorities for UNAIDS, alongside United Nations Office on Drugs and Crime (UNODC) which is our lead cosponsor on these issues, is to actually bring together drug authorities, AIDS authorities and prison authorities to talk jointly about the strategies which they are adopting to identify jointly what the barriers are to effective strategies for dealing with these intertwined problems in their settings such as prisons, or in relation to street policing, or in relation to HIV services and health services.
Back to topInjecting drug use and HIV: Interview with UNAIDS Team Leader, Prevention, Care
Cosponsors:
Press centre:
High Commissioner calls for focus on human rights and harm reduction in international drug policy (10 March 2009)
Feature stories:
OPINION: Silence on Harm reduction not an option (11 March 2009)
51st session of the Commission on Narcotic Drugs (11 March 2008)
Reducing drug related harm (14 May 2007)
Injecting drug use: focused HIV prevention works (11 May 2007)
Harm reduction to be scaled up in Ukraine (11 April 2007)
Increased HIV services for drug users needed (14 November 2006)
External links:
The Commission on Narcotic Drugs (CND)
Statements:
Publications:
Best Practice Publication: High Coverage Sites—HIV Prevention among Injecting Drug Users IDU in Transitional and Developing Countries ( En | Fr | Es | Ru )