



Feature Story
Pace of decline in new adult HIV infections remains short of ambition
14 November 2019
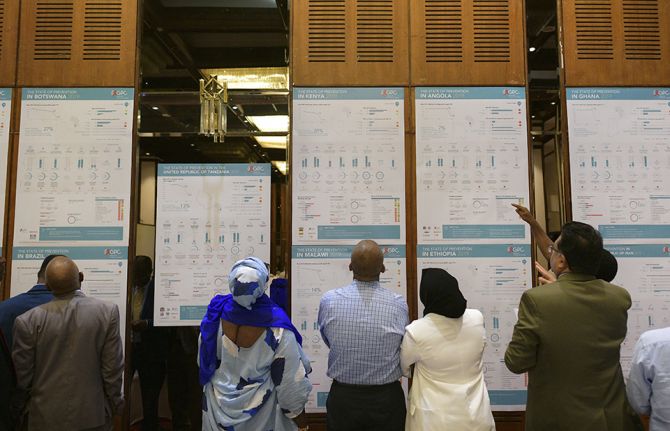
14 November 2019 14 November 2019The co-conveners of the Global HIV Prevention Coalition, UNAIDS and the United Nations Population Fund, have launched a new report on progress made in reducing new HIV infections across 28 countries that have been particularly affected by HIV. The report was launched at the High-Level Meeting of the Global HIV Prevention Coalition, held on 12 November on the sidelines of the Nairobi Summit on ICPD25.
Together, the 28 countries account for 75% of all new HIV infections globally—1.2 million of the 1.7 million new HIV infections among adults in 2018. The report, Implementation of the HIV prevention 2020 road map, shows that among the coalition countries new HIV infections among adults declined on average by 17% since 2010, slightly higher than the global decline of 13%, but far short of the 60% decline needed in 2018 to meet global HIV prevention targets.
“We are nearly 40 years into the HIV epidemic and it is unacceptable that governments and leadership are still shying away from sensitive issues,” said Winnie Byanyima, Executive Director of UNAIDS. “Investments in HIV prevention do not match the needs of our people; in some countries, even the basic commodities like condoms are not available, accessible or affordable in rural areas, for young people or key populations.”
The report shows that some countries have made significant progress, with 12 countries reducing new adult HIV infections by 26% or more since 2010. They include countries with major epidemics, such as South Africa, with a 39% decline, the Democratic Republic of the Congo, with a 37% decline, Uganda, with a 36% decline, and Zimbabwe, with a 28% decline.
Some coalition countries, however, experienced concerning increases in new adult HIV infections, including Nigeria, where new adult HIV infections increased by 8%, and Pakistan, which is experiencing a rapidly growing HIV epidemic among key populations, where new adult HIV infections rose by a staggering 56%. On average, new HIV infections in non-coalition countries remained relatively stable between 2010 and 2018.
The report shows that while there has been some progress in developing programmes for adolescent girls and young women, the Global HIV Prevention Coalition estimates that in 2018 only 34% of the areas with high HIV prevalence had dedicated comprehensive HIV prevention programmes for women and girls—far short of the global target of reaching 90% of adolescent girls and women with these services by 2020. During the meeting, Nyasha Sithole, from the Athena Network, made a strong call for investment and engagement of adolescent girls and young women in HIV prevention and sexual and reproductive health programming.
The Global HIV Prevention Coalition was established in 2017 to galvanize greater commitment and investment in HIV prevention in order to achieve the 2020 prevention target of reducing new HIV infections among adults by 75% by 2020 (against the 2010 baseline). Its added value is clearly visible in a number of focus countries and beyond. Countries confirm that it has promoted a more systematic and structured approach to HIV prevention programming and built momentum in most of the 28 countries; however, much more needs to be done to meet global commitments.
“The coalition has been working as an important platform for countries to share their progress and experiences in HIV prevention, providing a very good opportunity for us to take joint actions to reduce new infections and curb the spread of the disease. This is the key to realize the Sustainable Development Goal target on ending AIDS by 2030,” said Yu Xuejun, Vice-Minister of Health of China and current Chair of the UNAIDS Programme Coordinating Board.
To accelerate progress in stopping new HIV infections, momentum urgently needs to be stepped up by increasing investment, addressing HIV-related stigma and discrimination, addressing the legal, policy and structural barriers to HIV prevention, especially for adolescent girls and young women, key populations and their sexual partners, and taking measures to expand community-based responses.
“I am convinced that community action is the key not only to HIV prevention, but prevention of all ill health. It is for this reason that we have made primary health care the focus of universal health coverage in Kenya,” said Sicily Kariuki, Cabinet Secretary of the Ministry of Health, Kenya.
By taking these critical steps and increasing efforts to address persistent gaps in programme coverage and ensuring that services and community programmes are available to everyone in need, significant progress can be made towards ending AIDS.
During the meeting, which was chaired by the Cabinet Secretary of the Ministry of Health of Kenya and the Minister of Health of Zambia, representatives of the coalition countries made bold commitments and pledges to scale up HIV prevention in their respective countries.
The Nairobi Summit on ICPD25




Feature Story
UNAIDS Executive Director holds first face-to-face meeting with key donors
13 November 2019
13 November 2019 13 November 2019Ahead of the opening of the Nairobi Summit on ICPD25, the Executive Director of UNAIDS, Winnie Byanyima, and Peter Eriksson, the Minister for International Development Cooperation of Sweden, co-hosted a ministerial breakfast meeting with key donors and partners to highlight the need for a strong UNAIDS to lead the global response to HIV.
It was Ms Byanyima’s first face-to-face meeting with some of UNAIDS’ key donors and partners in her capacity as the Executive Director of UNAIDS, during which she pledged to take a feminist approach in taking the organization forward.
“UNAIDS is at a critical juncture as it emerges from the challenges of the past two to three years, and the staff will be my first priority; we need healing, trust-building and closure. I want to bring back the joy in the great work of UNAIDS,” said Ms Byanyima.
Katherine Zappone, the Minister for Children and Youth Affairs of Ireland, Christopher MacLennan, Canada’s Assistant Deputy Minister of Global Issues and Development, and other heads of delegations applauded UNAIDS’ intention to make meaningful culture change happen at UNAIDS.
“UNAIDS has been at the frontline of the AIDS response for years. Canada has been a strong supporter and we are so pleased that Winnie has joined,” said Mr MacLennan.
Ministers and representatives of Australia, Belgium, Canada, Finland, Germany, Ireland, Luxemburg, the Netherlands, Norway, Sweden and Switzerland encouraged UNAIDS to continue its leading role in promoting community-led solutions and responses. They also highlighted the need to leverage the unique capacity of UNAIDS and build on its human rights expertise to address the social and political barriers that are hindering progress on HIV.
“We must integrate sexual and reproductive health and rights better into the HIV response in order to reach our targets,” said Mr Eriksson. “The Joint Programme has a very important role in driving sexual and reproductive health.”
The meeting was also attended by representatives of several UNAIDS Cosponsors―the United Nations Population Fund and the United Nations Development Programme (UNDP). “UNDP is committed to working with UNAIDS in supporting governments to establish enabling legal, policy and regulatory environs for effective and rights-based HIV responses,” said Achim Steiner, the Administrator of UNDP.
UNAIDS, donors and partners agreed on the need to forge partnerships with the Global Fund to Fight AIDS, Tuberculosis and Malaria to ensure a sustainable response to HIV.
The meeting was the first in a series of events planned as part of UNAIDS’ enhanced collective engagement and strengthened collaboration as it embarks on the process of developing a new strategic plan on HIV.
The Nairobi Summit on ICPD25





 together with members of the organisation. Credit:UNICEF")
Feature Story
Confronting the link between HIV and gender-based violence in Jamaica
07 November 2019
07 November 2019 07 November 2019Monique McDonald is an HIV peer educator who tells the story of her childhood with unflinching courage. “I was sexually abused by my uncle at the age of 12 and contracted HIV.”
Ms McDonald has written about her experiences in a book called I am now free. It uses her old diary entries to describe the abuse she suffered as a child and her journey to recovery. Today, she supports young women living with HIV, helping them to come to terms with their status and advising them on adhering to treatment. She has also founded the Ashley Fund to help other sexual abuse survivors to continue their education.
She admits that it’s been a long road.
“I was so depressed, I didn’t know who to trust,” she remembers. “How could this happen, and everybody turned their eyes?”
Rushell Gray reflects on her past with a similar mix of sorrow and disbelief.
“As a young girl everybody turned a blind eye and blamed me. I was the AIDS girl walking around in the community. Nobody said, “this man needs to go to jail.” At one point I almost gave up because the stress was too high,” she said.
Ms Gray now works as a Mentor Mom. The Mentor Mom programme enlists young mothers living with HIV to share their experiences and help other young women coping with similar situations. Mentor Moms answer questions and offer reassurance, accompany young women and girls on their health visits and reinforce clinical guidance on the importance of taking medicines regularly.
Both Ms McDonald and Ms Gray are employees and past clients of Eve for Life, a Jamaican nongovernmental organization that helps to prevent new HIV infections and improve the quality of life of women and children living with or affected by HIV. Clients benefit from peer support groups, psychological care and empowerment programmes.
Joy Crawford and Patricia Watson founded Eve for Life 11 years ago. While supporting young women and girls affected by HIV, they quickly learned that there was a clear link between HIV infection, adolescent pregnancy and child sexual abuse. According to Situation analysis of Jamaican children, a 2018 report by the United Nations Children’s Fund (UNICEF), more than one in five (21%) adolescent girls in Jamaica said that they had survived sexual violence.
As a long-standing provider of technical support and capacity-building around sustainability for Eve for Life, UNICEF is keen not only on supporting girls, but addressing the cultural norms that make them vulnerable.
“There is this pervasive idea that adult men should have some level of access to a girl’s body if they are in their life, supporting the family or something like that,” explains Novia Condell, UNICEF Jamaica’s Adolescent Health and Empowerment Specialist. “Of course, the girl has no power to negotiate any protection in a situation where she has been abused or exploited.”
High on UNICEF’s agenda is supporting the community engagement necessary to shift attitudes around child sexual abuse. Eve for Life has spearheaded the “Nuh guh deh” (don’t go there) campaign, which aims to stop sexual abuse. They use complementary strategies—everything from community meetings to music videos—to get the message out.
The UNAIDS country office in Jamaica also provides technical support to Eve for Life and has helped the organization build partnerships for resource mobilization. The UNAIDS Caribbean subregional office is also working with Eve for Life to create safe spaces for young survivors and leaders to raise awareness about the link between gender-based violence and HIV.
There is also a focus on meeting young women’s basic needs, including food, clothes and health care. But beyond these services, work continues to provide teenage girls and young women living with HIV with a deeper level of emotional support and mentorship.
“Jamaica’s Ministry of Health has found a strong partner in Eve for Life—one that is able to focus on resilience and life skills-building. They get the girls’ lives on track so they can improve their lot and the lot of their children,” says Ms Condell.
Related

.")


Feature Story
The power of transgender visibility in Jamaica
12 November 2019
12 November 2019 12 November 2019“Is it safe to do their work?” Renaè Green and Donique Givans go silent for several seconds. “I am still scared,” says Ms Green, the Associate Director for Policy and Advocacy at TransWave Jamaica. “I don’t like to go to certain spaces. If anyone wants to participate in one of our campaigns, we explain the risks. You don’t know what kind of backlash you might experience.”
Ms Givans, who is the organization’s community liaison officer, knows this all too well. She wasn’t up front about her gender identity with her father when she began becoming more visible in her advocacy work.
“He doesn’t want anything to do with me now,” she says, her voice shaking a little. “He told me to go and not to come back to his house. So, we do let people know they might have difficulties.”
TransWave was formed in 2015 following a lesbian, gay, bisexual and transgender health and gender-based violence training, conducted by WE-Change and supported by the Jamaica Forum for Lesbians, All-Sexuals and Gays and Jamaica AIDS Support for Life.
TransWave’s Executive Director, Neish McLean, is the only transgender man at the helm of a Caribbean transgender organization. Recently Mr McLean discussed his personal journey publicly, exploring issues ranging from the distinction between gender identity and sexuality to top surgery. This is largely unchartered territory in a Caribbean nation famed for its social conservatism.
“For a long time, people actually said that transgender people didn’t exist in Jamaica because people could not put a face to them or identify anyone who was transgender. Now we have so many people who identify. It has helped in terms of explaining who transgender people are,” explains Ms Green.
In addition to increasing transgender visibility, TransWave advocates on a wide range of subjects that affect the community—the lack of access to transgender-oriented housing, education and employment, for example, as well as initiatives to reduce poverty and violence. HIV is a huge challenge. A 2018 Integrated Biological and Behavioral Surveillance Survey conducted by the University of San Francisco found that 51% of Jamaican transwomen tested were living with HIV.
TransWave advocates strongly for all members of the community to access health care.
“Many are aware that they are HIV-positive but don’t seek treatment. They are just waiting to die. People cannot stomach not being able to live their lives as their real selves and won’t put themselves through the distress of going to a clinic,” says Ms Green. “It becomes difficult because all eyes are on you and you are putting yourself at risk for people to attack or hurt you,” explains Ms Green.
In July, UNAIDS Jamaica supported TransWave’s Transgender Health and Wellness Conference. The event helped launch a toolkit on how health-care providers can provide holistic, non-discriminatory services, along with dialogue around the rights and inclusion of transgender people. The organization has also met some employers to gauge the degree of acceptance for the inclusion of transgender workers.
Ms Givens paints a mixed picture of what life is like for transgender people in Jamaica.
“It is very difficult, but people try to align themselves with society’s gender norms. They might do a little makeup to feel comfortable, but they don’t go heavy. Some workplaces allow people to be themselves, but you don’t have transwomen wearing skirts,” she said.
Public transportation is often challenging. When TransWave books a taxi, for example, they are never sure if the driver will be tolerant. Renting an apartment can be a landmine. Lower-priced housing often means living in a less safe area. Landlords and neighbours can be judgemental.
At the extreme, homelessness remains a major problem, with some young transgender people being thrown out of their homes before they even become teenagers. This is often the starting point for a frightening array of vulnerabilities, including a lack of schooling, poor job prospects and bad health, with some turning to sex work.
Asked about their hopes for the future, Ms Givans and Ms Green list adequate funding for TransWave and being able to further their education. Ms Green adds that she would like to emigrate.
“But not everybody wants to leave Jamaica and not everybody should leave,” she says pointedly. “That’s why we are working so hard. So that we can get to a point where everybody is accepted.”







Feature Story
Former Welsh Rugby Captain Gareth Thomas speaks passionately about confronting HIV-related stigma
11 November 2019
11 November 2019 11 November 2019Welsh rugby ace Gareth Thomas has spoken out about the urgent need to confront HIV-related stigma head on. Speaking at a special event during the 17th European AIDS Conference, which was held in Basel, Switzerland, from 6 to 9 November, Mr Thomas said that he wants to help create an environment that breaks stigma and where people can make educated decisions based on facts and be free to talk openly about HIV.
It was the first time that the former Welsh rugby captain had spoken in front of an audience about his decision to publicly disclose his HIV status. He talked of the overwhelming reaction and public support following his disclosure and the airing of the BBC documentary he made about living with HIV, which included footage of him completing the International Iron Man triathlon in Wales.
He spoke of his determination to show people that living with HIV can also mean living a long, fit and healthy life and that medical advances now mean that with access to effective treatment, people living with HIV cannot transmit the virus, advances that he said not enough people know about.
“I wanted to challenge stigma head on,” said Mr Thomas. “I wanted people to see that I was capable of swimming two and a half miles in the sea, cycling 112 miles and running a marathon with HIV. If I can do that, we can do anything. Since that day, I have received nothing but support and love.”
The event was moderated by the Director of the UNAIDS Eastern Europe and Central Asia Regional Support Team, Vinay Saldanha, and shone a spotlight on the power of partnerships to advance progress towards ending AIDS. The participants included a panel of international experts working in the field of community-led organizations, funding, international partnerships and activists living with HIV.
Advocate Bruce Richman, Founder and Executive Director of the Undetectable = Untransmittable (U = U) campaign, spoke about the importance of U = U to overcome the stigma experienced by people living with and affected by HIV and how the campaign has become a public movement to break down fear and misunderstanding around HIV.
“U = U sets people living with HIV free from the fear of transmission,” said Mr Richman. “We have been living with and dying from HIV stigma for over 35 years. U = U builds our partnership to end that stigma.”
Head of the sexual health charity the NAZ Project in London, United Kingdom, Marion Wadibia spoke of how partnerships can offer culturally specific sexual health services to people being left behind. “We need to integrate race into all our work,” she said.
She was joined by other panellists who talked about the importance of using bolder business unusual approaches to end AIDS in all communities and populations. Rageshri Dhairyawan, of Barts Health NHS Trust, London, cited Soul Sisters as an example of a partnership that provides support for women who are experiencing domestic abuse for sexual health services and HIV prevention. “Violence against women and girls is a leading driver of HIV transmission,” said Mr Dhairyawan.
The event, entitled Together We Can, was organized by Gilead Sciences. The conference joined together leading HIV experts, scientists, researchers, activists and communities of people living with HIV to discuss the latest progress towards ending AIDS in Europe.
The conference gave special attention to the growing HIV epidemics in eastern Europe and central Asia, examined progress towards the 90–90–90 targets, looked at cities and municipalities that have joined the Fast Track cities partnership, discussed models of care for people living with HIV as they get older and tacked eliminating HIV-related stigma and discrimination.
Webcasts, presentations and ePosters of the 17th European AIDS Conference are available on the European AIDS Clinical Society Resource Library for a period of three months.
Related





")
Feature Story
Promoting gender equality in Brazil step by step
30 October 2019
30 October 2019 30 October 2019Daniela de Barros, a Finance Assistant in the UNAIDS Country Office in Brazil, is also a UNAIDS Gender Focal Point for Latin America and the Caribbean.
She traces her interest and motivation to helping others and promoting equality back to a good deed in her childhood. “It was one of those dream-come-true situations. When my sister and I were younger, my parents couldn’t afford to pay for ballet classes. But their best friend’s sister ran a ballet studio and, one day, she invited us to start taking classes free of charge. From that point on, I never stopped dancing.” Ms de Barros says that dance has taught her to be disciplined, organized, focused and connected “body and soul” to her life and work.
“Besides all these important skills that I use all the time as a professional and as a mother of adolescent twins, I have also taken another important lesson from my ballet classes: I have learned how to connect with myself and meet my potential and my inner power,” she said. “Isn’t this what we want from such an important initiative like the UNAIDS Gender Action Plan? Empowerment and transformation for all women inside and outside this organization?”
From her role overseeing financial, administrative and operational aspects of the UNAIDS Country Office, Ms de Barros has seen that change management is crucial for maintaining staff motivation. “Although change generates some insecurity, in the end it can be a breath of fresh air. I have learned to recognize that change is important for organizations.”
Ms de Barros believes it is time that women were encouraged to be confident about achieving their goals. “The Gender Action Plan we have inside UNAIDS not only reinforces our self-confidence and courage, it also inspires men to support the women they work with,” she said.
Ms de Barros is sure that “UNAIDS chose her,” rather than the other way around. “I studied international relations and always wanted to work for the United Nations, but I confess I had never heard of UNAIDS until a friend of mine told me I should apply for the position,” she said. “I have grown a lot and learned so much from UNAIDS.”
She says that turning 40 years old has come with some significant changes for her and she now wants to engage in projects that can transform lives. For more than six months she’s been teaching ballet to other women and is just about to start what she describes as “a recently-born old wish”: teaching dance to young kids and adolescents from poor communities in Brasília, where she lives.
“I like to think of ballet as the realization of a Buddhist thought that says we see our external world from within, and that by working on our internal perspective, we can change the world outside. It is the power of dance and where it can take us. And this is what I want to teach children and women through the project.”


Feature Story
Desperately seeking an HIV cure: Belgian research centre studies viral rebound
17 October 2019
17 October 2019 17 October 2019Growing up, Linos Vandekerckhove loved biology, so it seemed an obvious choice to go to medical school. After two years of practising internal medicine, in 2001 he had a chance to spend a year in South Africa.
“Here I was, in the eye of the storm, where most days one person would come to the clinic and die within 48 hours from an AIDS-related illness,” he said.
He returned to his native Belgium shaken. “It was really shocking to me, because in Europe treatment was readily available, so suddenly I felt like some people pay a very high price.”
IS THERE A CURE FOR HIV? There is no cure for HIV. However, there is effective treatment, which, if started promptly and taken regularly, results in a quality and length of life for someone living with HIV that is similar to that expected in the absence of infection.
FREQUENTLY ASKED QUESTIONS ABOUT HIV AND AIDS
Not wanting to plunge back into a hospital setting, he opted to work for a few days a week in an HIV virology laboratory. After getting his PhD, he wanted to continue researching HIV, so he joined the Ghent University Hospital in Belgium. After a few years of working with patients, he finally had more time to spend on research. In 2009, he started his own laboratory, the HIV Cure Research Center Ghent, and a year later he spent five months in San Francisco, United States of America, to familiarize himself with research on a cure.
“The sabbatical helped me gain momentum,” he explained. His research laboratory now employs 20 people.
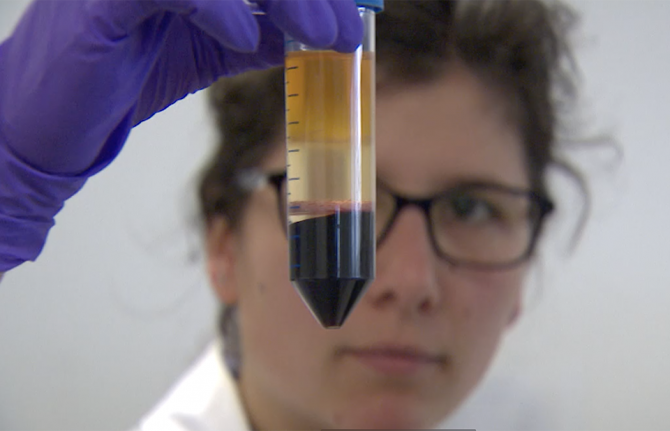
Recently, his team completed a study with 11 people living with HIV. It involved pausing antiretroviral therapy so that scientists could observe viral rebound.
“An ethics committee had to validate the study and, of course, we held a patient forum to analyse the stress factors associated with taking people off treatment and the subsequent tests on them,” Mr Vandekerckhove said. His team made sure that the eight to nine procedures would be minimally invasive and carried out in a day, so that the volunteers could return to work after two days. To minimize any further disruption, technical assistants went to each person’s home to regularly gather blood samples.
“We wanted to involve the volunteers as much as possible and show our support from A to Z,” he said.
Two patterns surfaced from the study. Viral rebound, which took 15–36 days, occurs randomly. The team found more than 200 independent rebound events, from the gut to the lymph nodes to “just about everywhere where immune cells are present.”
Mr Vandekerckhove’s team also found that, depending on where the virus rebounded in a part of the body, the virus had evolved with its own individual make-up, like a barcode or a fingerprint. The researchers found different viruses, showing that they are not all the same single virus that has emerged from a reservoir, but rather multiple re-emergent events.
“We analysed 30 barcodes per cell type and about 400 barcodes per person,” he said.
That’s when they asked for help from virologists and statisticians.
“Our study revealed that having a medicine that would only target the lymph nodes is wrong. What this shows is that you need to focus on many organs, not just one,” Mr Vandekerckhove said.
UNAIDS Science Adviser Peter Godfrey-Faussett congratulated the HIV Cure Research Center Ghent. “Such detailed work advances our understanding of reservoirs where HIV “hides” while treatment suppresses the virus in the blood,” he said.
In his opinion, the research highlights the many challenges of the virus, since HIV can rebound from a wide range of reservoirs. “This is why a clear understanding of the nature of the reservoirs is so important to find a cure.”
Mr Vandekerckhove remains very positive, pointing to how gene therapy used to be science fiction but is now a reality.
“We need to bring the world of research to the world of patients,” he said. In his mind, a cure is one of the many facets of HIV that we cannot overlook.
Fellow Belgian Jonathan Bossaer couldn’t agree more. Ten years ago, he became very ill in South Africa and soon found out he had contracted HIV. After many years of feeling lost, a friend’s death made him realize he had to change.
“I was able to free myself of the frustration and shame that I had been living with for almost eight years and let go,” Mr Bossaer said. He founded a charity to raise awareness about HIV stigma. “Positively Alive has three main objectives: educate people about HIV, normalize HIV and help end HIV by raising funds,” he explained.
Half the funds go to a South African orphanage and the other half to Mr Vandekerckhove’s research centre. “Ending the HIV and AIDS epidemic is an enormous challenge and research for a cure and a vaccine needs our full support,” he said.
Pausing a bit, Mr Bossaer said, “The fight is far from over, but we are on the right path.”
Related





Feature Story
Putting HIV prevention back at the centre of Brazil’s LGBTI pride
17 October 2019
17 October 2019 17 October 2019In June 2019, more than 3 million people took to the streets of São Paulo, Brazil, to celebrate lesbian, gay, bisexual, transgender and intersex (LGBTI) pride and to mark the 50th anniversary of the Stonewall riots, a turning point in the struggle for LGBTI rights. For gay entrepreneur Almir Nascimento, 2019 marked a return to involvement in the event’s organization after a 20-year break.
What prompted Mr Nascimiento’s pride comeback was a rising unease about the increasing number of new HIV infections in Brazil among young people, especially among young gay men and transgender women. For many years, he thought that the mobilization of the 1990s and the arrival of antiretroviral therapy would be enough to end the HIV epidemic.
“The epidemic was at its height when I first joined pride as one of the organizers in 1999 and 2000. Back then, it seemed to me that we had made significant achievements, and I thought it would be enough to stop HIV”, recalls Mr Nascimento. “But four to five years ago, I began to notice that a lot of young gay, bisexual and transgender people were getting infected with HIV again, and even worse they were dying of AIDS-related illnesses at a really young age. This situation motivated me to come back and support the parade organizers in promoting an open discussion about HIV and AIDS inside our community.”
In 2018, there were around 900 000 people living with HIV in Brazil, with new HIV infections up by more than 20% since 2010. While HIV prevalence in Brazil among the adult population is estimated to be 0.5%, among transgender people it stands at around 30% and among gay men and other men who have sex with men at round 18.3%.
Mr Nascimento is the owner of a gay sauna in São Paulo and says he has always made efforts to ensure that his customers have the knowledge and tools to prevent HIV and other sexually transmitted infections. He partners with the São Paulo health authorities to distribute free condoms, for example. More recently, health researchers have been welcomed to the sauna to recruit people interested in participating in pilot programmes for PrEP (pre-exposure prophylaxis), a pill that can prevent people becoming infected with HIV.
“There is no denying that gay men and transgender people are the most affected populations here in Brazil. And I realized that the lesbian, gay, bisexual and transgender parades, including the São Paulo one, no longer had effective HIV initiatives within their associations,” he says. “Because of that, we decided to call a meeting with the 27 parades representing each of Brazil’s state capitals and a dozen others from the most important cities in São Paulo State. Altogether, we estimate they reach over 18 million people every year.”
Because the numbers are so huge, Mr Nascimento believes there is not only an opportunity but also a responsibility to convey HIV prevention and zero discrimination messages to the LGBTI community.
“There is still resistance among some parade organizers to link the festivities with AIDS-related discussions because of the fear of stigma and discrimination. But everyone is together during these events and we must take advantage of that to generate candid discussions to educate people about HIV prevention, which can save lives.”
With the support of the UNAIDS office in Brazil and other key partners, Mr Nascimento and the São Paulo LGBT Pride Parade Association are now preparing for the third LGBTI Youth Health and Prevention Meeting, to be held in November.
“After our first meeting in 2017 focusing on HIV prevention among young lesbian, gay, bisexual and transgender people, over a fifth of the participating parade associations have now started the same discussions in their cities. That’s what we want: that every pride president learns how to conduct them and that they hold their own meetings during pride week and indeed throughout the year.”



Feature Story
Empowering young Brazilians to talk to their peers about HIV
11 October 2019
11 October 2019 11 October 2019New HIV infections in Brazil increased by more than 20% between 2010 and 2018, so it’s crucial that young Brazilians start talking about HIV and learn how to protect themselves. That’s the aim of a project led by the United Nations Children’s Fund (UNICEF).
Swiping through one of his social media accounts, Jonas da Silva checks out the latest parties and public events in Salvador. He is also chatting online with other young people. They talk about sex, how and if they use condoms with their partners, what they know about HIV prevention and if they have been tested for HIV.
“What’s cool about the project is that we have young people talking to young people. We use our language and slang to address HIV,” he says. “This connection is vital. We can see they trust us, and this is when we know we have touched them with the information they need.”
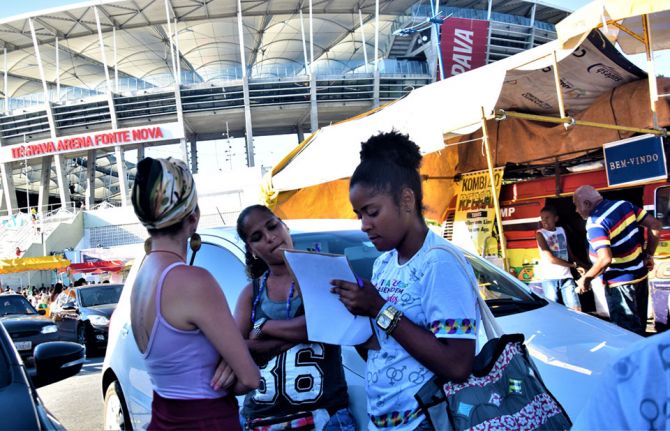
He and another 30 young people have been trained to work as volunteers in the Viva Melhor Sabendo Jovem (VMSJ) Salvador project. Their goal is to raise awareness among other young people about the importance of HIV testing and prevention. For that, they need to be where their peers are—online and on the street.
The project follows the calendar of traditional street parties and festivals, especially those that attract a large concentration of young people. It also responds to specific demands from key populations by mapping public gatherings where young lesbian, gay, bisexual, transgender and intersex people hang out. With a colourful small truck—the Test Truck—Mr da Silva and his co-volunteers can provide privacy for people who want HIV counselling and testing.
Since the project launched in August 2018, more than 1000 young people aged between 16 and 29 years have been tested for HIV in around 30 outings for the truck. As part of a strategy to promote testing among adolescents and young people, the volunteers also facilitate workshops on HIV and other sexually transmitted infections and host talks about sexuality and sexual health in schools. These events reached more than 400 students in the first six months of the project.
“The VMSJ Salvador peer education methodology makes it possible to engage more young people in these activities. It also helps them to become aware of the importance of HIV prevention and care,” said Cristina Albuquerque, Chief of Health and HIV/AIDS for UNICEF in Brazil. “Young people who get tested during our activities congratulate the initiative and complain that they have very few of these opportunities around town.”
In 2018, according to Ministry of Health estimates, young people aged between 15 and 24 years represented almost 15% of all new HIV diagnoses in Salvador.
“For us, too, the volunteers, this experience is important because we also start to take better care of ourselves, to apply these prevention methods to our lives and to pass the message on to those around us, to our friends and family,” said Mr da Silva.
The project is implemented in partnership with GAPA Bahia―one of the oldest nongovernmental organizations dealing with HIV issues in the country―and counts on the support of the UNAIDS office in Brazil. The young volunteers all went through a rigorous selection process before undergoing a training programme that included topics such as human rights, counselling and information on HIV and other sexually transmitted infections. They were also trained on community-based programmes, the functioning of the public health system and HIV services available in Salvador. The initiative includes a continuous training strategy on related topics.
“One of the most important things I have learned is that we have to respect each other’s choices and that we are here only to assist with information and inputs that we consider most appropriate to that person’s history and behaviour”, said Islan Barbosa, another of the volunteers.
“The project represents an important response to HIV testing demands in the city, especially among key populations, who very often avoid using public health facilities for that purpose. We are taking HIV testing to where these people are,” said Ms Albuquerque.


Feature Story
Two decades of engagement in the response to HIV in Brazil
14 October 2019
14 October 2019 14 October 2019Seven years after finding out that he was living with HIV, Jair Brandão was waiting for a medical appointment in a clinic in Recife, north-east Brazil, when a fellow patient informed him he could access psychosocial support at a nearby nongovernmental organization. Although it had taken him many years to accept his HIV status, he needed just three sessions of counselling to realize that he was meant to become an HIV activist.
“I was thrilled and scared at the same time, because I didn’t understand much about political spaces, nor about AIDS and health policies. I didn't know how to engage in political discussion,” recalls Mr Brandão, who two decades later is one of Brazil’s most influential HIV activists. “First, I had to accept myself as a person living with HIV, and this was one of the challenges. And then learn about the virus, take care of myself. Only after that did I start to learn about social and political issues.”
Mr Brandão says he believes that being an activist is natural for him. “Some people are born for that,” he says. “Being an activist is about being restless and not accepting injustices and violations of rights. I think I was born with this gift because I always led processes, even without knowing it was activism, and I was always concerned about helping and empowering others.”
After participating in three of the four United Nations high-level meetings on AIDS and in the 2018 high-level meeting on tuberculosis, Mr Brandão knows how difficult it is to engage in dialogues with other civil society peers and country representatives. His mother tongue is Portuguese, which is not an official United Nations language. “Speaking a foreign language is a major issue for us in Brazil, so we have to know at least Spanish. Very few activists know English fluently enough to be able to make interventions in these spaces.”
In July 2019, Mr Brandão was among the nongovernmental organization delegates at the High-Level Political Forum on Sustainable Development in New York, United States of America, representing RNP+ (the Network of People Living with HIV and AIDS) and his own nongovernmental organization, Gestos: Soropositividade, Comunicação e Gênero.
“It is essential for civil society to participate in the national implementation and monitoring processes of the 2030 Agenda for Sustainable Development effectively. We cannot achieve the Sustainable Development Goals without the full participation of civil society,” he says. “Defending the AIDS agenda also requires discussing other equally important and cross-cutting issues.”
Through his role as Project Adviser at Gestos and as a member of RNP+, Mr Brandão also leads the People Living with HIV Stigma Index 2.0 project in Brazil. With his peers at Gestos and other national networks of people living with HIV, and with the support of the United Nations Development Programme and UNAIDS, he helped train 30 people on interviewing techniques in seven Brazilian cities. In two months, they gathered information about HIV-related stigma and discrimination by conducting around 1800 interviews. The initial results will be released before the end of November.
“This process strengthened the activists who conducted the interviews because they could listen to and experience the stories that many people have been through and could not until now share with anyone,” he recalls. “We are in the fourth decade of the AIDS epidemic and still there is a lot of stigma and discrimination. The Stigma Index 2.0 is an instrument which gives us evidence of that in Brazil. We will be able to advocate for stigma-free, zero discrimination HIV policies and services.”
Mr Brandão says he believes in the power of collaboration and partnership to achieve social progress.
“The solidarity and spirit of community that helped create the AIDS movement must come back in our actions and hearts,” he says. “Rethinking strategies and creating new ways to bring about change is fundamental. Empowering new activists, especially young people, is critical. Young people need to be welcomed and open to receive information from experienced AIDS activists. It’s time to join forces, not to be divided.”