



Feature Story
Learning lessons on evaluation
02 April 2019
02 April 2019 02 April 2019“The fact that something is hard to evaluate doesn’t make it impossible,” said Anna Downie, who leads on strategic information at Frontline AIDS. Reflecting on the challenge of evaluating advocacy, coalition-building, generating new partnerships and increasing the capacity of communities, she added, “To be successful, it is essential to allow space for innovation, to hear from communities about what is important to them and involve them from the outset so that you are looking for the same results and the evaluation is truly useful.”
Ms Downie was one of a number of experts who gathered in UNAIDS headquarters on 29 March in Geneva, Switzerland, for UNAIDS’ first consultation on evaluation. With the aim of informing the new UNAIDS evaluation policy, to be presented to the UNAIDS Programme Coordinating Board (PCB) meeting in June, the participants shared lessons they have learned while working on evaluation.
“Generating evaluations that are independent, credible and useful is the foundation of our work” said Susanne Frueh, the Chair of the United Nations Evaluation Group and Chair of the consultation.
The central role of countries in supporting a strong and independent evaluation function at UNAIDS was highlighted. The need for dedicated funding for evaluation, for the evaluation function to be independent and for transparency in the appointment of the head of the evaluation function were highlighted. The credibility and expertise of the staff of the office of evaluation, the establishment of an independent advisory committee and the need to protect the office from becoming politicized were also noted.
Michel Sidibé, UNAIDS Executive Director, highlighted the importance of the evaluation function. “We will not be able to transform or sustain our gains in the AIDS response if we don’t have clear learning from what we are doing. We will not be able to quicken the pace of action and help countries to scale up if we are not able to share our work and lessons learned,” he said.
The participants agreed that it is essential not only to ensure a strong gender and equity element in evaluations but also to measure what works and identify results in the areas of gender and human rights, which are cornerstones of the AIDS response. Triangulating data on human rights with civil society is a good way of ensuring that the evaluation provides a full picture. The importance of assessing the support provided by UNAIDS when major donors transition from countries was also highlighted.
In the medium to long term, the participants highlighted the need to build the capacity of young evaluators and to consider working with the growing number of evaluation companies from the global South.
The UNAIDS policy on evaluation is to receive a final round of comments from stakeholders soon. It will then undergo a peer review by the United Nations Evaluation Group before being presented to the UNAIDS PCB for endorsement.
Related






Feature Story
The road to NAIIS: UNAIDS’ role in better understanding Nigeria’s HIV epidemic
22 March 2019
22 March 2019 22 March 2019After six months of data collection and three months of data analysis, the President of Nigeria, Muhammadu Buhari, announced the results of the Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS) in March 2019. Costing approximately US$ 100 million and covering more than 200 000 people, 185 survey teams collected data for the NAIIS, the largest HIV-specific survey in the history of the global response to the epidemic.
In Nigeria, three types of survey have been conducted by the Federal Ministry of Health HIV/AIDS Division to determine HIV prevalence and to monitor the trends of the HIV epidemic in the country:
- The HIV Sentinel Survey (HSS), which is conducted typically every two to three years among women attending antenatal clinics, which determines HIV prevalence among pregnant women.
- The National Reproductive Health Survey (NARHS), which is conducted every five years among the general population.
- The Integrated Biological and Behavioural Surveillance Survey (IBBSS), which is mostly used to monitor prevalence and behavioural trends among key populations.
The last HSS and IBBSS took place in 2014, while the last NARHS took place in 2012. These data sources have served as the main survey data sources for the AIDS response in the country.
Between 2012 and 2014, significant progress was made in the AIDS response in Nigeria. The number of antiretroviral therapy sites doubled, prevention of mother-to-child transmission sites increased eightfold and HIV counselling and testing sites increased fourfold. According to government data, 6.7 million adults were counselled and tested for HIV in 2014, a 65% increase from the previous year. HIV testing among pregnant women also doubled in 2014 compared to 2013. Similarly, the number of people living with HIV on antiretroviral therapy increased significantly.
However, despite this progress, there was no commensurate improvement in the statistics on the coverage of antiretroviral therapy among people living with HIV. National achievements in the AIDS response were poor compared to the targets, and programme implementers reported difficulties in identifying people living with HIV in need of services. It was therefore suggested that the HIV burden was not as high as was estimated using the available HIV prevalence data.
Former UNAIDS Country Director Dr Bilali Camara was a longstanding advocate for an expansion of the surveillance of the country’s epidemic.
“Working as UNAIDS Country Director in Nigeria, I realized early on that we did not have the full picture of the country’s AIDS epidemic,” said Dr Camara. “I was pushing for surveillance to be expanded for a long time―I am very happy that with this new survey we now have a better understanding of the AIDS epidemic in Nigeria and that it will allow us to better respond to the areas and people in most need.”
Dr Camara’s persistence indeed paid off.
In July 2015, the National Agency for the Control of AIDS (NACA), under the leadership of its then Director-General, Professor John Idoko, decided that it was imperative to better understand Nigeria’s HIV epidemic. The NACA set up a National Stakeholder Committee, comprising the head of the National AIDS and STI Control Programme, the UNAIDS Country Director, the World Health Organization (WHO) representative, the United States President’s Emergency Plan for AIDS Relief (PEPFAR) Coordinator, civil society and others, which decided to conduct a triangulation of data from various sources.
“The need for the survey was first initiated under my leadership, but we had overwhelming support from Dr Camara. UNAIDS headquarters was even willing to send its Strategic Information Director to Nigeria at the time,” said Professor Idoko.
Many countries have shifted to a location–population approach, which helps to ensure that HIV services reach the people and geographic areas with the greatest need. Location–population approaches require granular-level data, which were not typically available in Nigeria. In 2016, the UNAIDS Nigeria Strategic Information Team, led by Dr Gatien Ekanmian, was tasked to develop an evidence-informed methodology to estimate the HIV burden at the local level. During this process, a closer analysis of the results from the various surveys highlighted a series of issues with the HSS surveys:
- The sentinel sites were too limited in number to ensure nationally representative geographic coverage based on the demographics of the country.
- Urban sites were oversampled.
- Rural sites were usually under-sampled.
- There were often more urban sites than rural sites in many states, thus the HSS results reflect more the urban HIV epidemic than the rural epidemic among pregnant women.
The conclusion of the UNAIDS Nigeria epidemiological analysis was that the HSS and NARHS were no longer giving sufficiently precise epidemiological information. It was recommended that a comprehensive review of the HIV surveys being conducted in Nigeria be carried out in order to address the shortcomings in the existing survey approaches and methodology.
Thereafter, the UNAIDS country office met with various stakeholders, including the Development Partners’ Group on HIV, and presented these observations and recommendations, effectively utilizing the Development Partners’ Group on HIV to galvanize support from PEPFAR and the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) in particular.
In June 2016, the Director-General of the NACA raised an objection to the latest estimate of 3.5 million Nigerians living with HIV, believing that the figure was an overestimation. He had the opportunity to discuss his concerns with UNAIDS country directors, Dr Erasmus Morah and Dr Alti Zwandor at the International AIDS Conference in Durban, South Africa, in 2016. In July 2016, after advocacy from the UNAIDS country office, the new Minister for Health, Professor Isaac Adewole, and the new Director-General of the NACA, Dr Sani Aliyu, agreed on the need for an epidemiologically robust population-based HIV survey in Nigeria. They approved the recommendations for a population-based survey and committed to mobilize resources for it.
“When I resumed as Director-General of the National Agency for the Control of AIDS, a recurring issue that came up at every introductory meeting with partners was the difficulty in finding new cases. It was obvious that there was a problem with case-finding. Was this because we were looking in the wrong places? I had doubts on the quality data we had … and we can’t achieve epidemic control if we don’t even know where we are. Hence, the number one priority of my administration was born―establishing the true prevalence of HIV in Nigeria by employing the best scientific and technical survey tools available in the shortest possible time,” said Dr Aliyu.
In November 2016, a review and triangulation of HIV data in Nigeria was commissioned by the NACA, in collaboration with UNAIDS, the findings of which gave further support for a national survey to develop more precise estimates of HIV prevalence. Firm support for the survey came from the Government of the United States of America (the Centers for Disease Control and Prevention, PEPFAR, USAID and the Department of Defense) and the Global Fund, which committed funding to the NAISS.
“It was easy to see that getting the data situation in Nigeria right was not only the right thing to do but also the dream of so many people. Fortunately, Nigeria had great partners to help turn this dream into reality. Programming and accounting for HIV results in the country will never be the same,” said Dr Morah, the current UNAIDS Country Director for Nigeria.
The United Nations system’s contributions in the NAIIS Technical Committee were anchored by UNAIDS, WHO and the United Nations Children’s Fund. Before the results of the survey were announced, Peter Ghys, UNAIDS Director of the Strategic Information Department, led a multi-group technical mission to Nigeria. The team gave advice on the use of the survey results, on the trends and the geographic locations of the epidemic, at the national and subnational levels. They also gave technical guidance to national partners on data management and governance, including on a strategy for country ownership and leadership of the survey results and support on how to communicate the changes in the epidemiological profile of HIV in the country.
“The road to NAIIS is a wonderful and brilliant story to tell, because it actually tells the story of the HIV response in Nigeria,” said Professor Adewole.
This feature is adapted from an article written by Erasmus U. Morah, Gatien K. Ekanmian and Doris, A.Ogbang
Region/country



Feature Story
"The community is not on the girls’ side"
15 March 2019
15 March 2019 15 March 2019Rise clubs are helping adolescent girls and young women start conversations about HIV and sexual and reproductive health and rights.
Khayelitsha is one of South Africa’s largest townships, situated in the Cape Flats in Cape Town, South Africa.
As is the case in many other communities in South Africa, women and girls in the semi-informal settlement deal with gender inequality on a daily basis, which puts them at higher risk of HIV infection.
Gender inequality is a barrier for adolescent girls and young women to access HIV and sexual and reproductive health services and comprehensive sexuality education. It also places girls at higher risk of gender-based violence.
“There is a lot of crime. The community is not on the girls’ side. The community believes that women must submit to men. Sometimes it is hard for us to speak out,” said a young woman who is a member of the Rise club in Khayelitsha.
“We belittle ourselves to fit in the box that the community puts us in. Girls get raped, kidnapped … there is a lot of violence. “You can do this, you can’t do that”, you are told what to do,” she says.
For most girls, it is difficult to talk to parents, teachers or family members about sex, sexuality and sexual and reproductive health and rights. Young women and adolescent girls face stigma and discrimination, such as being shamed for being sexually active, from nurses in health-care settings when they seek sexual and reproductive health services. While many countries in eastern and southern Africa have signed the Ministerial Commitment on Comprehensive Sexuality Education and Sexual and Reproductive Health Services for Adolescents and Young People in Eastern and Southern Africa and have some sort of policy on comprehensive sexuality education, implementation is still uneven.
Young women are at higher risk of HIV and other sexually transmitted infections than their male peers or older women.
In eastern and southern Africa, a quarter of the 800 000 new HIV infections in 2017 were among adolescent girls and young women between the ages of 15 and 24 years. Of the 2.17 million adolescents and young people aged 15–24 years in eastern and southern Africa living with HIV, 1.5 million are adolescent girls and young women.
Of the 277 000 new HIV infections in South Africa in 2017, 77 000 were among adolescent girls and young women between the ages of 15 and 24 years, more than double that of their male counterparts (32 000).
Knowledge of HIV prevention ranges from a high of 64.5% in Rwanda to low of 20.37% in Comoros, with South Africa mid-range at 45.8%.
In some countries in the region, adolescent girls and young women are permitted by law to marry at a young age. Early marriages are associated with loss of bodily autonomy, lack of education owing to school drop-out, lack of economic independence and gender-based violence.
Transactional sex contributes to the gender disparity in HIV infection among young people in sub-Sahara Africa.
Evidence shows that transactional sex among adolescent girls and young women is associated with a number of sources of HIV risk, including abuse and violence, alcohol use, having multiple partners, lack of condom use and age-disparate sex.
Rise clubs
Rise is a club for adolescent girls and young women that seeks to build social cohesion, self-efficacy and resilience through allowing adolescent girls and young women (aged 15‒24 years) a space to support each other and undertake projects in the community that help prevent HIV, mitigate its impact and enable safer choices.
Rise helps meet the needs of adolescent girls and young women in terms of building self-confidence and encouraging them to speak out against social ills and helps them to make decisions about their lives.
The clubs were started in 2014 for young people in 15 high-burden districts in South Africa by the Soul City Institute for Social Justice.
“African parents do not talk to us about sex and we are embarrassed to talk to them. I couldn’t speak to my sister so I joined Rise and now I can sit with my girls. Some are older than me and they can give me advice.” —Cinga
“My parents taught me that the only way to be knowledgeable is to ask questions. When I joined Rise, we’d ask questions for girls who can’t ask for themselves, making life easier for the girls.” —Okuhle
“I could not speak to anyone at home. And then I became the most talkative person. Rise has helped me deal with low self-esteem.” —Lisa
Adolescent girls and young women in eastern and southern Africa need laws, policies and programmes that meet their needs. These include tailored and focused programmes for sexual and reproductive health services and comprehensive sexuality education and on the prevention of unintended pregnancies, gender-based violence and HIV infection.
They must be informed by the principles of gender equality and human rights and should address other socioeconomic issues, such poverty and unemployment.
Having such policies and programmes will not only result in positive health outcomes but will give adolescent girls and young women the opportunity to live their lives with freedom and dignity.
Region/country








Feature Story
A vision of a reformed United Nations
22 March 2019
22 March 2019 22 March 2019“The Sustainable Development Goals are connected by the idea of leaving no one behind. In each country and every constituency, we need to define who those are and put them at the centre,” said Amina Mohammed, United Nations Deputy Secretary-General, during a visit to UNAIDS headquarters in Geneva, Switzerland, on 22 March. At the meeting she outlined her vision for a reformed United Nations that is fit to deliver against the Sustainable Development Goals.
Ms Mohammed highlighted the importance of young people and of ensuring that the next generation of United Nations staff members builds a strong future for the organization. She also spoke about the game-changing possibilities of gender parity and about United Nations reform and innovative partnerships. She reminded UNAIDS staff that, “We are all here to serve humanity and work to make a difference in people’s lives. We are not just here as professionals, we should bring more of ourselves and thereby more urgency and empathy into our work.”
Michel Sidibé, UNAIDS Executive Director, said in his welcome, “United Nations reform is not easy. It is about implementation and about the needs of countries and people. UNAIDS has been at the forefront of this agenda since the beginning and will continue to be, and we will fight for the people being left behind”.
Ms Mohammed extended her thanks to UNAIDS, stating that, “The Sustainable Development Goals would not have had the ambition to put people at the centre if you had not shown it can be done with the AIDS response. Good things come in small packages and UNAIDS’ role is essential.”
In closing, she said, “Our commodity is hope, it is the hope we give while we try to close the gap between the realities of our challenges and the aspirations of our dreams and those of many millions of people.”
Related







Feature Story
UN and AU working together for sustainable development
27 March 2019
27 March 2019 27 March 2019“We cannot have sustainable development without sustaining peace. Neither can we build a secure future for everyone without addressing the root causes of our conflicts and vulnerabilities,” said Amina Mohammed, the United Nations Deputy Secretary-General.
Ms Mohammed was speaking in Marrakech, Morocco, at the twentieth session of the Regional Coordination Mechanism for Africa (RCM–Africa)―a joint United Nations and African Union body that supports African development.
“The United Nations is working with the Africa Union to try to get the 47% of people of the continent still under the poverty line out of poverty, bring energy to the doorsteps of 500 million people without electricity and garner the US$ 60 billion needed to empower African women,” said Vera Songwe, the Executive Secretary of the United Nations Economic Commission for Africa.
The African Union Commissioner for Human Resources, Science and Technology, Sarah Anyang Agbor, encouraged the participants to, “Live by Ubuntu. It is my, your, our responsibility to strengthen collaboration for the reforms.”
Michel Sidibé, the Executive Director of UNAIDS, co-chaired a panel meeting with Ms Anyang Agbor at the RCM–Africa session. During the panel meeting―entitled “Upscaling durable solutions, including addressing the forced displacement–development nexus”―the participants noted that more than a third of the world’s displaced people are in Africa. The participants agreed on the need to understand and address the root causes of displacement and build on what is known to work to break the cycle of vulnerability. Mr Sidibé emphasized that fostering resilient societies means first addressing the challenge of income inequality.
The RCM–Africa session was held on 23 and 24 March.
Region/country
Related








Feature Story
Helping the forgotten generation
02 April 2019
02 April 2019 02 April 2019Towering over a throng of young people, Christine Kafando peppers the crowd with questions.
“Do you feel pressure from other boys and girls?” “Do you feel abandoned because of poverty?” “Do you have all the information you need regarding your health and HIV? If not, ask me, ask your partners, ask! Okay!”
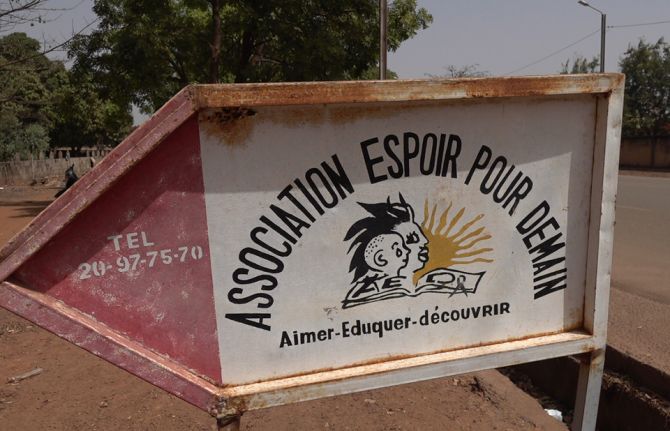
The 40 boys and girls nod and shrug. They have come for a workshop run by the Association Espoir pour Demain (AED) in Bobo-Dioulasso, Burkina Faso, which aims to create a space for young people to learn about sexual health and to train some to become peer educators.
“After having seen a number of young students come to us pregnant, we felt a need to start these workshops,” Ms Kafando, the founder of AED, said.
Issa Diarra said the workshop enabled a dialogue. “In our society, we really don’t talk that much about sex and, I would add, health issues, but here we really had the chance to discuss all that,” he said. Another attendee of the workshop, Roland Sanou, agreed, “Sex today remains taboo for young people, but I don’t want it to stay that way.”
Many of them say times have changed and that the way they think is different from the way their parents thought. “Currently, we young people are aware and we know what we want and we know that being sick can keep us from realizing our dreams, so that’s why we are rallying,” said Baba Coulibaly.
At the beginning, AED helped women living with HIV to access treatment. It then grew to help mothers and their babies born with HIV. Fifteen years later, many of those children are now teenagers and still drop by. Reflecting on her two decades as an HIV advocate, Ms Kafando said, “For so many years, women have been the face of HIV, but it’s key to include men and boys to raise their awareness.”
Jacinta Kienou, a nurse who has been at the association since it was founded, said that there were two big challenges: a number of young people living with HIV no longer take their treatment regularly and many young people are unsure about how to deal with relationships.
“Because they live with HIV, and they are young, lots of problems bubble up concerning affection and acceptance by others with regard to their HIV status,” she said. “Often relationships end because of someone’s HIV status. We council them and their parents at that time,” she added.
In Burkina Faso, young people make up more than 60% of the population and data show that many of them do not know their HIV status. UNAIDS Strategic Information Officer André Kaboré describes two gaps concerning young people. “Despite high-quality treatment being readily available, there are children out there who don’t know they’re living with HIV. Worse, many of those who do know that they are living with HIV aren’t accessing treatment,” he said.
In the country, 94 000 people are living with HIV, 9400 of whom are children under the age of 15 years. While 65% of adults living with HIV are on life-saving antiretroviral therapy, only 28% of children living with HIV whose status is known, about 3500, are on treatment. Ms Kafando calls them the forgotten generation. “They fell through the cracks because until now they had never been sick or needed attention and thus were never tested for HIV,” she said.
The head of the National AIDS Council for Bobo-Dioulasso and the surrounding region, Suzanne Sidibé, said, “We lost sight of children born with HIV. Our aim, with the help of the Association Espoir pour Demain, is to fan out to families through health mediators.”
Hoho Kambiré, who is living with HIV, has four children, two of whom are living with HIV. As an AED health mediator, she speaks about the benefits of knowing one’s status to all who will listen. She visits families, accompanies women to clinics and provides support.
“It is necessary to test all the children to know who is sick and who is not sick and follow up to keep them healthy,” she said. AED has now more than 50 health mediators, mostly women like Ms Kambiré, who originally came to the association seeking health services herself.
The United Nations Children’s Fund (UNICEF) and UNAIDS both support AED financially. Mireille Cissé, a UNICEF HIV specialist, said that the United Nations in Burkina Faso had identified the top priorities for the AIDS response in the country, including working with civil society.
“We agreed that a community link needed to be established, because they are our entry into families,” she said. UNICEF formalized the health mediators’ contribution by providing a stipend for their work and works hand in hand with the regional office of the Ministry of Health.
“A real victory for us was to have the health mediators integrated into the health teams of the districts,” Ms Cissé said. “That buy-in really facilitated the role of the health mediators and has raised their profile.”
UNAIDS has reinforced the capacity of the health mediators to widen their scope of work, which ranges from psychosocial counselling to training on treatment adherence. “To maintain our progress in the HIV response and end AIDS depends a lot on civil society like the Association Espoir pour Demain,” Job Sagbohan, UNAIDS Country Director, said. “We really hope for maximum impact.”
Special page
Region/country












Feature Story
Stepping it up for adolescent girls
15 March 2019
15 March 2019 15 March 2019“Without our voice, you are doing it for you, not for us”, said Winny Obure, a youth leader and women’s rights defender from Kenya, at the United Nations in New York, United States of America.
She was joined by other young women demanding the removal of barriers to their sexual and reproductive rights and for adolescent girls to be empowered. The event—Step It Up!—was a call to action for the most left behind adolescent girls and was convened by UNAIDS, the ATHENA Network, the Governments of Australia and Namibia, and UN Women, with 25 partners from the United Nations and civil society.
Adolescent girls and young women are still disproportionally affected by HIV. One million adolescent girls live with HIV globally and every week 7000 adolescent girls and young women become infected with HIV. Comprehensive sexuality education is so limited that levels of knowledge about HIV prevention among young people have remained flat over the past 20 years.
“We will not reach the Sustainable Development Goals if the voices and aspirations of adolescent girls are oppressed,” said Gunilla Carlsson, UNAIDS Deputy Executive Director, Management and Governance.“Where is the accountability for the millions of adolescent girls being left behind?”
All too often, adolescent girls remain invisible to decision-makers, especially if they belong to groups that are discriminated against, criminalized or stigmatized. As many of the participants pointed out, they are subjected to human rights violations, including violence and harmful practices, and denial of their sexual and reproductive health and rights.
“We need to move away from these meeting rooms and go to communities to talk to adolescent girls and young women. We need to address the uniqueness of specific groups of girls, of their specific needs .We have the solutions, it’s just a matter of including us in the discussion,” said Maximina Jokonya, a young woman from Zimbabwe.
“Teenage girls are often out of sight and out of mind and they are not where the power is, it’s still with men,” said Sharman Stone, Australia’s Ambassador for Women and Girls. She highlighted the barriers that girls face in the Pacific, where they are denied contraception and subjected to high levels of violence. She said that a key priority for Australia during humanitarian crises is to ensure access to sexual and reproductive health services.
The Minister of Gender Equality and Child Welfare of Namibia, Doreen Sioka, spoke about championing the rights of adolescent girls and young women, comprehensive sexuality education and integrated sexual and reproductive health and HIV services. She outlined major achievements in fulfilling international HIV targets. A new law in Namibia enshrines the right of all children to access critical services—at 14 years of age, children can now be tested for HIV without permission from their parents or guardians.
The young women at the event underscored their realities and restricted opportunities, as well as what works to improve their lives. Deneka Thomas, from Trinidad and Tobago, described how she uses art in schools to interact with lesbian, gay, bisexual and transgender young people and girls traumatized by bullying, rape and other forms of violence.
Raouf Kamel of AIDS Algérie spoke about the first-ever initiative in the Middle East and North Africa to hear the voices and experiences of especially marginalized groups of women. They had all experienced violence, pointing to adolescence as a crucial point in life when the risks to their health and safety, and of HIV infection, are especially marked.
The participants concluded that much more needs to be done to address the needs and rights of adolescent. Investing in inclusive, quality education, in HIV, sexual and reproductive health services and in mental health is key. Other important actions include preventing and responding to gender-based violence, promoting women’s rights, engaging boys and investing in youth organizations and community-based initiatives led by, and for, young women.
The event was held on 13 March on the margins of the sixty-third session of the Commission on the Status of Women.
Quotes
“I am not learning anything because teachers cannot communicate with me. If disabled and HIV positive, where are they going to get services?...You are not being given a chance to be a human being.”
“We can now speak freely without being judged…we have transformation for girls, now claiming their rights.”
“For every young girl who got HIV because our policies, governments and agencies were not willing to recognise that there were vulnerable youngsters who desperately needed support. For that, we are culpable. …These SDGs are about them. They will need to live with whatever we do, or what we don’t do, today.”
Video
Programme of the event
UNAIDS International Women’s Day Statement
Women and HIV – a spotlight on adolescent girls and young women
 were unveiled at a special event held in Abuja, Nigeria, on 14 March that was attended by the President of Nigeria, Muhammadu Buhari, and the Executive Director of UNAIDS, Mi")




Feature Story
Nigeria adapts strategy to end the AIDS epidemic
20 March 2019
20 March 2019 20 March 2019Nigeria has adopted its Revised National HIV and AIDS Strategic Framework 2019–2021 to guide the country’s future response to HIV. It follows the results of a new survey that shows that HIV prevalence in the country stands at 1.4%. Previous estimates had indicated Nigeria’s HIV prevalence at 2.8%.
The results of the Nigeria National HIV/AIDS Indicator and Impact Survey (NAISS) were unveiled at a special event held in Abuja, Nigeria, on 14 March that was attended by the President of Nigeria, Muhammadu Buhari, and the Executive Director of UNAIDS, Michel Sidibé. During his speech, Mr Sidibé commended the president’s leadership in guiding the country’s response to the HIV epidemic. Nigeria has tripled the number of people on HIV treatment since 2010 and adopted a test and treat policy in 2016.
The improved understanding of the country’s epidemic based on the survey results will allow for more efficient investments in the response to HIV and a more effective planning for the provision of HIV prevention, care and treatment services. It will permit the adoption of a population–location approach to deliver services to the people in the areas where they are needed the most.
During his three-day visit to Nigeria, Mr Sidibé met the Minister of Health, Isaac F. Adewole, to discuss progress, gaps and challenges in the AIDS response and pledged UNAIDS’ support to Nigeria in the implementation of the new framework. This was further underscored when Nigeria’s Minister of Foreign Affairs, Geoffrey Onyeama, and Mr Sidibé signed a new cooperation agreement to strengthen the relationship between UNAIDS and Nigeria.
Mr Sidibé also paid a courtesy call on the wife of the country’s president, Aisha Buhari, to formalize and extend her appointment as the UNAIDS Special Ambassador for the Elimination of Mother-to-Child Transmission of HIV and the Promotion of Treatment for Children Living with HIV in Nigeria.
Ms Buhari thanked UNAIDS for extending her mandate and reiterated her commitment to achieving an AIDS-free generation of children.
“This will enable me to contribute more towards ensuring that no child is born with HIV in Nigeria,” said Ms Buhari.
Representatives of the Network of People Living with HIV/AIDS in Nigeria also met with Mr Sidibé to voice their concerns about the gaps and challenges in the country’s AIDS response.
The network’s national coordinator, Abdulkadir Ibrahim, said services were too often not reaching the people in the greatest need. He asked for UNAIDS’ help in strengthening community responses to the HIV epidemic and to ensure that people living with HIV, particularly young people, were involved in creating policies and programmes that affected their health and well-being.
Region/country





Feature Story
There is life after HIV, there is love
08 March 2019
08 March 2019 08 March 2019Mandisa Dukashe was nervous before she took an HIV test in 2002. As a nursing student in South Africa, where more than 4 million people were living with HIV at the time, she knew it was possible that she would test positive for the virus. “I was very stressed,” she says. “I kept postponing the test.”
Ms Dukashe had learned about HIV during her university studies, so the staff at the clinic assumed that she was well informed and didn’t need pretest counselling. “They told me I am a nursing student and should know what it entails.”
The test result was positive. Ms Dukashe joined 510 000 other South Africans who became newly infected with HIV in 2002—20% of all new infections worldwide.
When Ms Dukashe was diagnosed with HIV, South Africa had only recently started to roll out treatment and it was five years before she got access to it. It was harder to come by then, with limited medicine formulations that were only prescribed for people falling ill with an AIDS-related illness.
In 2002, South Africa had more than 4 million people living with HIV but fewer than 15 000 people receiving treatment through public facilities. That year the country also recorded more than 190 000 AIDS-related deaths.
The picture today is much improved.
Ms Dukashe and her family featured on the cover of the 2018 UNAIDS World AIDS Day report, Knowledge is power, as living proof that sustained HIV treatment can suppress a person’s viral load and prevent the transmission of HIV to a partner and children. “This can be done by anyone,” she says.
In 2017, there were more than 4.3 million people on HIV treatment and 110 000 AIDS-related deaths in South Africa. Yet there are still miles to go to end the AIDS epidemic by 2030. South Africa continues to rapidly scale up HIV treatment and is determined to reduce annual AIDS-related deaths to 80 000 or fewer by 2020.
Ms Dukashe says it didn’t take long to reconcile herself to her HIV-positive status. She was determined to embrace her status, look after herself and spread the word. She wanted to warn other young people to avoid HIV infection, take a test and seek support if they tested HIV-positive. “After the counselling, I felt so bold and confident and I was ready within a week to go out and tell the world with an intention of raising awareness, in particular among young women and adolescent girls.”
“At first I didn’t want to reveal my HIV status because I knew that it could be an issue, so I focused on my nursing studies. Eventually I fell in love with a guy and I feared he would reject me, but I had to tell him—I cannot live a lie."
But things were not always easy for her. Ms Dukashe was married when she was diagnosed. “Some people say that HIV can bring you closer, but that wasn’t to be.” They eventually divorced and it took time before Ms Dukashe found love again. “At first, I didn’t want to reveal my HIV status because I knew that it could be an issue, so I focused on my nursing studies. Eventually I fell in love with a guy and I feared he would reject me, but I had to tell him—I cannot live a lie. It took me three months to disclose my status, but to my surprise his response was much better than I hoped. He remains HIV-negative and he is the best husband and father of my children that I could ever ask for. When you have got that kind of support you can live healthily and even forget about HIV.”
Despite the love and support of her husband and family, the weight of living with HIV came flooding back to Ms Dukashe when she and her husband started planning to have children. “When the time came for us to talk about preventing HIV transmission to our children, we needed to think carefully, plan and consult medical experts. That brought it all back for me and I got depressed for a while.”
But help was available, she says. “I got counselling and worked through those feelings and it was all worth it. I now have two wonderful children who were born without HIV. It was my responsibility and also my husband’s responsibility. We got great support and advice.
“Being able to give birth to HIV-negative children was a blessing because I believe if I did not test, my kids could have been born with HIV.”
Ending new HIV infections among children is a high priority for South Africa, with a target of virtual elimination by 2020. Yet despite many years of concentrated effort, 13 000 children acquired HIV from their mothers in 2017. “It pains me that I could not breast-feed my babies,” says Ms Dukashe. “Because I wanted so hard to prevent them from getting HIV I fed them with formula milk, which made me sad.”
Thanks to improved treatment options, women living with HIV are now encouraged to take HIV treatment for their own health and to avoid their children becoming infected during pregnancy, birth or breastfeeding. All breastfeeding women in South Africa living with HIV and on HIV treatment are encouraged to exclusively breastfeed until their baby is at least six months old.
Ms Dukashe is now working as a project manager for point-of-care HIV testing and quality assurance. She is also a motivational speaker, creating demand for HIV testing and treatment, including among women of child-bearing age and their partners.
“Being able to give birth to HIV-negative children was a blessing because I believe if I did not test, my kids could have been born with HIV.”
“I want to encourage everybody in our situation: there is life after HIV, there is love. People should not think twice about going for an HIV test. It was the best decision I ever made, since I learned what to do to keep myself healthy and prevent transmission to my spouse and children. Thinking twice is not going to change the result.”
“As a healthcare professional, it is important for me to show that I am living positively with HIV and managing it successfully. My experience should encourage others to protect themselves and get tested regularly. If you test positive for HIV, start treatment and get counselling and support so you can keep yourself healthy and protect others. HIV is, unfortunately, a reality for millions of people, but treatment works and we are stronger than HIV.”
Finally, Ms Dukashe has a message for young women: “HIV is invisible. Always use a condom and be wary of older men. Age-disparate relationships are a risk. If you rely on an older partner and try to please them, you won’t be able to insist on using a condom,” she said. “I speak from experience, as someone who faced the same pressures.”
Region/country






Feature Story
International Women’s Day in Ethiopia
12 March 2019
12 March 2019 12 March 2019The UNAIDS Executive Director, Michel Sidibé, celebrated International Women’s Day in Addis Ababa, Ethiopia, at an event organized by the Ministry for Women, Youth and Children Affairs and supported by UNAIDS. The event brought together female leaders and representatives of women’s associations from all over the country. Addressing the meeting, the Prime Minister of Ethiopia, Abiy Ahmed, emphasized that women are the “pillars of the nation.”
Yalem Tsegaye, the Minister of Women, Children and Youth Affairs, outlined the Jegnit initiative. Jegnit means “heroine” and is an innovative movement led by the Government of Ethiopia to empower and bring more women to leadership positions, both at the community and political levels.
During the event Mr Sidibé congratulated the Prime Minister and the Government of Ethiopia for its bold reforms in addressing the gender gap by appointing women to leadership positions in all sectors. He commended the Prime Minister for ensuring gender parity in his Cabinet.
“It is time to empower women and girls, because ending AIDS is as much about righting power imbalances as it is about health. This means prioritizing girls and young women in true partnership with them. It means providing adolescents girls and young women with more options and real choices,” said Mr Sidibé.
While in Addis Ababa, Mr Sidibé met with Vera Songwe, Executive Secretary of the United Nations Economic Commission for Africa, the first woman to hold the post in 60 years, to discuss ongoing collaboration on sustainable AIDS responses across the African continent.
Mr Sidibé also met with Amira Elfadil of the Department of Social Affairs of the African Union. In 2019, UNAIDS and the African Union are celebrating 20 years of a partnership focused on ending the AIDS epidemic across Africa.

