


Feature Story
Achieving and sustaining viral suppression among people living with HIV in Trinidad & Tobago
27 April 2026
27 April 2026 27 April 2026Civil society organisations play a critical role in the AIDS response, including facilitating access to HIV prevention and treatment services. The Medical Research Foundation (MRF), based in Trinidad & Tobago, is a perfect example of this. With 5,202 people in care, MRF serves more than 70% of all people living with HIV in the country and has the distinction of being the largest non-governmental HIV treatment and care clinic in the English-speaking Caribbean. It is also increasingly recognised as a model demonstrating excellence in HIV care and service delivery, grounded in strong clinical outcomes, robust data systems, and patient-centered innovation.
Through its coordinated and patient-centered approach to treatment and care, MRF is helping thousands of people living with HIV achieve improved health outcomes, including viral suppression and undetectable status.
At the end of June 2025, its treatment programme reflected strong performance across the continuum of care. Of 5,146 clients retained on treatment, 5,000 received a viral load test in the past 12 months—an extraordinary 97% coverage—and 4,733 were virally suppressed, achieving the global 95% target. By September 2025, there were 5,202 individuals receiving ART at MRF, of whom 4,822 (95%) achieved viral suppression and 4,107 (79%) were undetectable. These outcomes reflect the sustained impact of adherence support, treatment counselling, and continuous clinical follow-up.
Equally notable is the decline in treatment interruptions, a key measure of programme retention. Through community engagement, adherence support, and proactive follow-up strategies, interruptions steadily decreased from 446 to 246 between 2024 and 2025.
MRF credits its dedicated staff and partners, including the Ministry of Health and PEPFAR/CDC, for the success of its treatment and care programme. According to Nyla Lyons, MRF’s Technical and Scientific Director, “MRF’s success is a powerful reminder that coordinated partnerships, patient-focused interventions, and strong monitoring systems can achieve extraordinary health outcomes for people living with HIV. We are demonstrating how data-driven, patient-centred care can turn what was once a public health challenge into a story of hope, resilience, and success.”
These achievements highlight MRF’s critical role as a bridge between government services, civil society, and international partners, ensuring uninterrupted, high-quality care for people living with HIV. The combination of high viral suppression rates, sustained retention, and declining treatment interruptions underscores a model of care that is both effective and scalable. Sustaining and building on these gains will require continued investment, commitment, and innovation, which MRF is well-positioned to lead as it continues to demonstrate excellence in HIV care and service delivery in the Caribbean.
"MRF's partnership with the Ministry of Health is an example of the kinds of collaboration between government and civil society, including communities, that are essential for achieving and sustaining public health outcomes,” said Luisa Cabal, UNAIDs Regional Director for Latin America and the Caribbean. “The Global AIDS Strategy 2026-2031 endorses and places strong emphasis on the important role these partnerships play in the HIV response. UNAIDS commends MRF on the work they have been doing and their impressive achievements last year."
Region/country




Press Statement
UNAIDS congratulates the Bahamas on WHO certification of eliminating mother-to-child transmission of HIV and hepatitis B
23 April 2026 23 April 2026Kingston/Geneva, 23 April 2026—UNAIDS congratulates the Bahamas on eliminating both mother-to-child transmission of HIV and hepatitis B. The certifications, awarded by the World Health Organization (WHO), with the Pan American Health Organization (PAHO), recognize sustained progress to ensure that pregnant women have access to quality antenatal care, get tested on time and start treatment early. The result has been that babies have been born free of preventable infections.
In 2010, countries of the Americas committed to eliminating mother-to-child transmission of HIV and syphilis. They endorsed a regional strategy that was later updated through PAHO’s Plan of Action for the Prevention and Control of HIV and Sexually Transmitted Infections. To reach elimination targets, countries have strengthened HIV prevention and treatment within primary health care and maternal and child health services through wider screening during pregnancy, better follow-up for babies exposed to HIV and faster access to medicines and care.
“The Bahamas are showing that eliminating mother-to-child transmission HIV and other sexually transmitted infections is possible,” said Winnie Byanyima, Executive Director of UNAIDS. “This achievement reflects political will for steady investment in primary health care and the dedication of health teams and people living with and most affected by HIV. When women can test early in pregnancy, start treatment without delay and stay in care, every child has a better chance of being born free of HIV.”
Validation suggests that a country or territory has met the required impact and programme indicators and that it can show results are being sustained.
Across the Caribbean, countries and territories have worked towards the global targets of eliminating mother-to-child transmission of HIV. WHO and PAHO first certified Cuba in 2015 for dual elimination of mother-to-child transmission of HIV and syphilis. In 2017, certifications followed for Anguilla, Antigua and Barbuda, Bermuda, the Cayman Islands, Montserrat, and Saint Kitts and Nevis. More recently, Belize, Dominica, Jamaica, and Saint Vincent and the Grenadines have also been certified.
UNAIDS recognizes PAHO’s leadership in driving the regional elimination agenda and supporting countries through its Elimination Platform. The platform helps bring together ministries of health, communities and partners to speed up action and sustain results. UNAIDS works closely with PAHO across the region, alongside the AIDS Healthcare Foundation, civil society and community-led organizations to strengthen services, improve surveillance and close remaining gaps so elimination gains are protected and expanded.
The certifications come as the world pushes to end AIDS as a public health threat by 2030. Preventing HIV infections among children remains a global priority. Between 2010 and 2024 new HIV infections among children were reduced by 62% from 310 000 in 2010 to 120 000 in 2024.
UNAIDS calls for continued investment to protect these gains. That means stronger, integrated maternal, newborn and child health services; reliable access to quality-assured medicines, diagnostics and supplies; action to tackle stigma and discrimination; and support for community-led responses that help women and families stay connected to care.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Region/country




Feature Story
UNAIDS uses Brazilian funk music to promote HIV prevention among young people in Brazil
22 April 2026
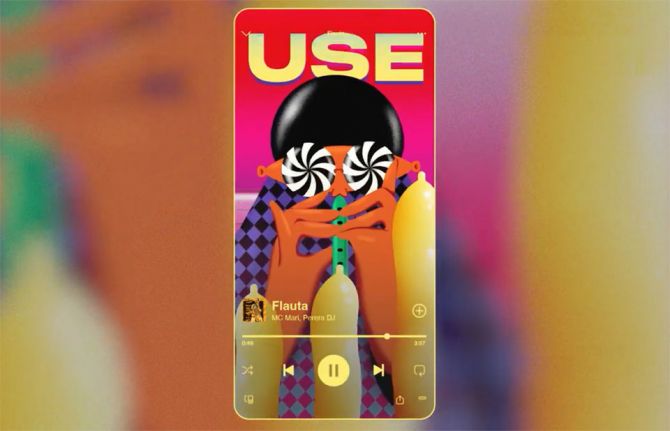
22 April 2026 22 April 2026A new initiative launched by UNAIDS in Brazil uses the popularity of funk music among young people to promote HIV prevention. Called Cover It (Proibidão Protegidão in Brazilian Portuguese), the campaign uses colourful illustrations with messages about condom use and other HIV prevention methods that are displayed when a selected group of songs play on Spotify.
The campaign was designed to reach young people, especially Gen Z, directly through their media consumption channels. Young people are both the prime listeners of Brazilian funk music as well as one of the groups most affected by HIV. According to the Brazilian Ministry of Health, young people aged between 15 to 29 accounted for 49% of all new HIV diagnosis in the country in 2024.
These data are consistent with the results of a survey conducted by the Brazilian Statistic Institute in 2024, which showed that in Brazil the percentage of young people under the age of 18 who reported using condoms during sexual intercourse dropped from 73% in 2009 to 57% in 2024.
Innovation in format: from entertainment to prevention
The campaign uses Spotify Canvas—a tool featuring eight-second looping videos that accompany track playback—as a novel media space. Hits by artists such as MC Livinho, MC Mari, and MC Pikachu had their original visuals replaced with animations promoting condom use. Combined, these tracks reach approximately 300 million views on the platform, significantly increasing the potential to reach adolescents and young people.
The choice of funk as an awareness platform reflects the genre’s massive reach among Gen Z. By occupying the visual space of “proibidão funk” (forbidden funk) tracks, UNAIDS introduces protection into a context where sexuality is already openly discussed, but access to information that promotes autonomy and informed prevention choices is often overlooked.
“Adapting language and promoting HIV prevention communication based on autonomy and choice is part of the necessary shift toward an equitable HIV response that meets the specific needs of different groups—especially young people, who continue to be the most affected by new HIV infections,” says Thainá Kedzierski, UNAIDS Brazil Communication and Advocacy Officer.
Some of the tracks featured in the campaign include “Flauta,” by MC Mari, “Lá no Meu Barraco,” by MC Pikachu and “Fazer Falta,” by MC Livinho. You can access the UNAIDS Brazil Spotify playlist here with the full list of songs and artists participating in the initiative.
In Brazil,the Unified Health System (SUS) offers a range of HIV prevention methods including free access to PrEP, PEP, male and female condoms, lubricants, HIV self-testing, as well as antiretroviral treatment for people living with HIV.
Region/country



Documents
The oligarchic order: How inequality broke multilateralism – and how to rebuild it
22 April 2026
UNAIDS Executive Director plenary talk at the Conference on the Future of Global
Development organised by the Global Development Institute, University of Manchenster.
Documents
PCB58 Information for participants
30 June 2026
Documents
Note Verbale
30 June 2026

Feature Story
Papua New Guinea advances national ownership of HIV response as crisis deepens
17 April 2026
17 April 2026 17 April 2026Papua New Guinea has long relied on international funding for its HIV response. The island country north of Australia covers only 30% of its HIV spending, with the rest funded by international donors. As global HIV financing declines, critical gaps in HIV prevention, testing and treatment have crept in.
A sustained rise in HIV infections — which have doubled since 2010 — combined with increasing strain on the health system and challenges linked to declining funding, led the Government of Papua New Guinea to declare a national HIV crisis in June 2025.
This crisis is increasingly affecting women and children. In 2024, an estimated 2,700 infants acquired HIV—around seven each day—while women account for approximately 60% of adults living with HIV in the country. Only around one quarter of pregnant women living with HIV receive antiretroviral therapy to stay healthy and prevent transmission to their child.
Declaring the crisis, Minister for Health Elias Kapavore described the situation as “deeply concerning” and pledged to mobilise urgent resources to protect “the next generation of Papua New Guineans”.
This year, the Government of Papua New Guinea allocated an emergency fund of US$13.5 million (50 million Papua New Guinean kina) for HIV, tuberculosis and malaria. The funding will support expanded prevention, increased access to testing and treatment, and strengthened services for pregnant women, children, adolescents and key populations.
The National Executive Council under the leadership of Prime Minister James Marape approved the funds.
“UNAIDS welcomes this important step towards a more sustainable AIDS response, while noting that further joint efforts are needed. We are working closely with the Government to implement the emergency response plan, scale up prevention and mobilise urgently needed resources,” said Eamonn Murphy, UNAIDS Regional Director for Asia Pacific and Eastern Europe and Central Asia.
“Behind every number is someone like me—a mother, a woman trying her best,” said Blendi, who found out she was living with HIV three years ago. She had feared that she would not live to see her two children grow up.
Despite being born with a physical disability and facing social stigma, she pursued her education, earned a degree and became the main breadwinner for her family.
“I am very thankful,” she said. “The medication is there. The doctors are there. They helped me continue living for my children.”
“This is a shared public health crisis that demands shared responsibility,” said Manoela Manova, UNAIDS Country Director in Papua New Guinea. “Sustaining services—especially for those most at risk—must remain a priority.”
For families like Blendi’s, the stakes are clear. The systems that made her treatment possible were built over the years and must now be sustained.
As a community health worker and HIV advocate, Blendi cannot imagine it any other way.


