
Feature Story
Landmark report on HIV among Zambia’s young people highlights challenges and charts the way forward
20 April 2012
20 April 2012 20 April 2012
A new report provides an extensive synthesis and analysis of recent data, gaps and challenges in AIDS prevention, treatment, care and support for young people in Zambia.
For Zambia’s young people the AIDS response has seen a number of important successes, with a significant 25% decline in HIV incidence over the last decade. However, according to a groundbreaking new report, the AIDS epidemic continues to have a huge effect on the country’s youth, especially young women, and much more needs to be done to achieve an HIV-free generation.
Situation Assessment of the HIV Response among Young People in Zambia provides an extensive synthesis and analysis of recent data, gaps and challenges in AIDS prevention, treatment, care and support for this key age group. It was launched at a high level meeting held from 17-18 April in Lusaka.
The event was supported by Zambia’s United Nations Joint Team in collaboration with the National HIV/AIDS/STI/TB Council (NAC), and the ministries of Health; Education; Youth and Sport; and Community Development, Mother and Child Health.
“We must reduce the number of new HIV infections among young people if we are to meet the targets set in the 2011 Political Declaration on AIDS,” said Deputy Minister of Youth and Sport Nathaniel Mubukwanu. “We are committed to continue developing high impact interventions using a combination of HIV prevention strategies to effectively respond to the epidemic,” he added.
Good progress but gaps remain
The assessment, focusing on 10 to 24 year olds, shows that HIV incidence decreased between 2001 and 2009 among young people and the proportion of young people having sex before the age of 15 has halved, from about 17% in 2000 to some 8% in 2009. There has also been a rise in the number of young people who were tested and received their HIV test results, from 7% in 2005 to 34% in 2009.
Providing young people with access to HIV testing, condoms, male circumcision and other reproductive health services, including sexuality education, will significantly contribute to Zambia achieving the UNAIDS’ vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths
Helen Frary, UNAIDS Country Coordinator, Zambia
Despite these achievements, HIV prevalence among young people remains high. In 2007 prevalence among those aged 15-19, for example, was 6% for women and 4% for men.
This is attributed to a number of factors. Dr Clement Chela, NAC Director General, citing the report said these factors included, “Poor comprehensive knowledge of HIV; gender inequality, poverty and the combination of transactional and intergenerational sex, early marriage, alcohol use, peer pressure and the negative gatekeeper attitudes towards condom promotion among young people.” Data shows that only 53% of adults expressed support for condom education for HIV prevention among young people.
The report also highlights that there is no comprehensive sexuality education package for pupils in school and a high level of stigma towards young people on treatment from their peers.
Way forward
One of the key recommendations in the report for increasing protection of young people is the promotion of their meaningful involvement in HIV policy and programme design and implementation. This can be facilitated by building their capacity as change agents and service providers and encouraging them to generate demand for HIV-related services.
As Youth Representative Chipasha Mwansa contended, while hoping that her peers’ recommendations would be taken with the seriousness they deserve: “Nothing for young people without meaningful involvement of young people.”
According to the report, bottlenecks that need to be addressed in order to meet young people’s needs are those that affect access to condoms, HIV counseling and testing, male circumcision and behavior change communication among young people in and out of school. Furthermore, youth friendly services should be expanded at the health facility and community level, including those integrating HIV care and treatment and legal protection for adolescents living with the virus.
Helen Frary, UNAIDS Country Coordinator, noted that a multipronged approach was necessary. “Providing young people with access to HIV testing, condoms, male circumcision and other reproductive health services, including sexuality education, will significantly contribute to Zambia achieving the UNAIDS’ vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths.”
To ensure that measurable progress is made in Zambia, the UN has pledged to work with relevant ministries and stakeholders to translate these main recommendations –and others— into a clear, costed and time-bound action plan which puts young people centre-stage.
External links
External links
Partners
Publications


Press Statement
UNAIDS welcomes new guidelines which give an additional HIV prevention option to discordant couples
19 April 2012 19 April 2012New guidelines released for couples HIV testing and counselling and for treatment and prevention in serodiscordant couples
GENEVA, 19 April 2012—New guidelines have been issued encouraging couples to go together for HIV testing in order to know their HIV status. The guidelines, released by the World Health Organization (WHO), also recommend that in couples who are serodiscordant—where one partner is living with HIV and the other not—antiretroviral therapy is offered to the person living with HIV to prevent his or her partner from becoming infected with the virus.
The Joint United Nations Programme on HIV/AIDS (UNAIDS) strongly welcomes the new guidelines and calls on all countries to implement them to reach the targets set in the United Nations 2011 Political Declaration on AIDS.
“Couples can now reap the benefits of antiretroviral therapy, to improve their own health, and to protect their loved ones,” said UNAIDS Executive Director Michel Sidibé. “By encouraging couples to test together, we can provide comprehensive options for HIV prevention and treatment—that they can discuss and manage jointly.”
New evidence now shows that antiretroviral therapy reduces the risk of HIV transmission from a person living with HIV to their sexual partners. WHO recommends that antiretroviral therapy be offered to HIV-positive individuals in discordant relationships even when they do not require it for their own health. The guidance also states that it is possible for couples to stay HIV serodiscordant indefinitely if they consistently practice safer sex using condoms.
“I am excited that with the roll out of these new guidelines, millions of men and women have one additional option to stop new HIV infections,” said Mr Sidibé. “This development begins a new era of HIV prevention dialogue and hope among couples.”
According the new guidelines, “couples who test together and mutually disclose their HIV status are more likely than those testing alone to adopt behaviour to protect their partner. Another potential benefit of couples testing together and sharing their results is that they can support each other, if one or both partners are HIV-positive, to access and adhere to treatment and prevent transmission of HIV to children”.
UNAIDS recommends that HIV testing and counselling should always be confidential and initiation of treatment must always be voluntary and never mandatory or coercive. Couples should have access to the full range of HIV prevention options available including the use of male and female condoms and medical male circumcision. They should also be provided with access to health services such as tuberculosis screening and reproductive health services including family planning with access to effective contraceptives and conception counselling for sero-discordant couples.
According to UNAIDS estimates, around 14 million people are eligible for antiretroviral treatment. At the end of 2011, only 6.6 million people were receiving the life-saving medicines. The guidelines recommend that in situations of limited or inadequate resources, people who require antiretroviral therapy for their own health should always be given priority.
Feature Story
World Bank: Greatly intensified HIV prevention in Africa vital to managing long-term financial impact of AIDS
17 April 2012
17 April 2012 17 April 2012A version of this story was first published at www.worldbank.org

A new World Bank report draws attention to the escalating cost of HIV treatment and the profound effect this is having on already stretched public finances.
Without a dramatic reduction in HIV infections in Africa existing national AIDS treatment programmes could become unsustainable in the future, warns a new World Bank Report. African governments, development partners and donors are urged to strenuously intensify their HIV prevention efforts to stop this becoming a reality.
The Fiscal Dimension of HIV/AIDS in Botswana, South Africa, Swaziland, and Uganda notes the considerable gains in the world’s AIDS response, with six million people now receiving antiretroviral therapy (some 5.1 million in Africa) and the significant increase in global AIDS spending, rising from under US$300 million in 1996 to nearly US$16 billion in 2009. However, the report also draws urgent attention to the escalating cost of HIV treatment and the profound effect this is having on already stretched public finances.
According to the co-author of the report Elizabeth Lule, "Strategic investments in preventing new HIV infections—while also meeting current treatment, care and support needs—can help countries plan for what will otherwise be an unmanageable fiscal burden."
Such strategic investments are critical in an era of global economic uncertainty. Curbing new HIV infections and improving fiscal planning can lead to a considerable drop in the financial commitment needed to fund an effective national AIDS response.
In Botswana—which has an HIV prevalence of some 25%—the report projects that the fiscal costs of AIDS will peak at 3.5% of Gross Domestic Product (GDP) around 2016, slowly falling to 3.3% of GDP by 2030 if new infections decline. However, with mining revenues slowing down relative to GDP, the costs of the epidemic could rise to over 12% of government revenues by 2021, presenting a huge fiscal challenge.
In South Africa, the epidemic has significant implications for public finance and the government's ability to achieve other key social and health policy objectives. An important aspect of the fiscal dimension of HIV in South Africa is the impact on social expenditures.
Strategic investments in preventing new HIV infections—while also meeting current treatment, care and support needs—can help countries plan for what will otherwise be an unmanageable fiscal burden
Elizabeth Lule, report co-author
"By scaling up HIV prevention programmes, South Africa stands to save (US$2,500) per infection," said Ruth Kagia, World Bank Country Director for Botswana, South Africa and Swaziland. "Investing in collecting data on the drivers of the epidemic is key to making the national AIDS response more effective and achieving better health and social outcomes for people."
For Swaziland, HIV has more serious fiscal repercussions given declining government revenues and the macroeconomic situation. With the highest HIV prevalence in the world at an estimated 26%, Swaziland has contributed 60% of the costs of the epidemic from its domestic resources over the past few years. However, costs of the AIDS programme are rising and projected to increase to 7.3% of GDP by 2020. External financing will need to increase substantially to meet the country’s financing gap.
In Uganda, the costs of the national response are estimated to rise to over 3% of GDP. Costs incurred by a single infection are estimated at about 12 times GDP per capita (US$5,900) per new infection as of 2010.
"Frequently, it is not countries with the highest HIV prevalence that face the heaviest burden in financing their HIV programmes, but low-income countries where each infection costs several times more than GDP per capita, and domestic resources are fewer," said Markus Haacker, a co-author of the report.
The report argues that countries can manage both HIV treatment and fiscal sustainability by marrying treatment with HIV prevention and making existing programmes more cost-effective, improving resource allocation and efficiency and examining innovative funding mechanisms.
Publications
Related

Feature Story
Prioritising gender equality in response to AIDS in Liberia
11 April 2012
11 April 2012 11 April 2012
Women returning from a farm with vegetables to be sold in a market on the outskirts of Monrovia, Liberia.
Credit: VII Photo/Marcus Bleasdale
Cynthia Quaqua is a mother, wife, the president of the Liberian Women’s Empowerment Network (LIWEN), and, perhaps most importantly, a survivor. Raped by soldiers during the Liberian civil war, she became pregnant as a young woman. Years later she fell ill and was diagnosed with HIV. Suddenly, she found herself abandoned by her relatives even began discussing where to bury her.
Fortunately, a Lutheran pastor gave her a place to live and directed her to a clinic where she could receive HIV treatment. She then found social support through a women’s group, where members had, like her, experienced sexual violence. Today, Cynthia is a picture of health and a powerful presence, taking her anti-retroviral medications twice daily. “The support from other women showed me that I was not alone and has allowed me to come this far,” she said.
Although Liberia is on the recovery from conflict, sexual violence remains prevalent. Research shows that 29% of ever married women experienced physical or sexual violence from a male intimate partner in the last 12 months.
The support from other women showed me that I was not alone and allowed me to come this far
Cynthia Quaqua. President of the Liberian Women’s Empowerment Network
Violence is both cause and consequence of women’s vulnerability to HIV. In Liberia, women account for 58% of all adults living with HIV. Young women and girls are particularly affected with an HIV prevalence more than double that of their male peers. The stigma associated with HIV and gender based violence is a major barrier to women accessing and adhering to HIV treatment and prevention services.
The President of Liberia and first ever female elected head of government in African, H.E. Ellen Sirleaf Johnson, has put gender equality and the empowerment of women at the centre of Liberia’s post-conflict and development agenda. Liberia was the first country to put into practice the UNAIDS Agenda for Women and Girls, setting strategic priorities for supporting women and girls’ rights, and gender equality through HIV responses.
Equally, the national response to HIV is prioritising gender equality as a smart investment for more effective programmes, under the leadership of the Minister of Gender and Development Julia Duncan Cassell. “We are fully cognizant that if the issues of HIV are to be fully addressed in Liberia, Africa and the rest of the world, we need to empower women living with HIV and get them involved at all levels,” said Mrs Cassell.

Cynthia Quaqua is a mother, wife, the president of the Liberian Women’s Empowerment Network, and, perhaps most importantly, a survivor.
Credit: UNAIDS
A mid-term review of the implementation of the national operational plan took place in Monrovia the first week of April involving partners from government, civil society, faith-based organisations, networks of women living with HIV and the UN system.
The review found that significant progress had been made in generating and maintaining political commitment to address HIV and sexual violence in Liberia. Data collection on sexual and gender based violence has increased and reporting structures have been harmonized, allowing for the routine collection of strategic information to inform national programmes.
Since the launch of the operational plan, government Ministries have put in place HIV and Gender co-ordination offices with domestic resources to champion HIV and gender programming, and HIV, gender and sexual and reproductive health services has been integrated into national polices. A coalition of actors has been established to address gender based violence and HIV, as well as contributing to addressing gender based violence broadly. The coalition meets monthly to monitor progress of activities.
We are fully cognizant that if the issues of HIV are to be fully addressed in Liberia, Africa and the rest of the world, we need to empower women living with HIV and get them involved at all levels
Minister of Gender and Development Julia Duncan Cassell
Other positive developments include the active engagement of associations and networks of women living with HIV in addressing sexual and gender based violence and increasing access to integrated HIV and health services for women.
But challenges remain, including the need to increase access to sufficient domestic financial resources and more effective coordination of different actors to maximise collective impact.
“UNAIDS and its co-sponsors recommit to intensify efforts against HIV and sexual violence by focusing on developing mutual accountability for results, partnerships for country ownership and generating program efficiencies through innovation and integration,” said David Chipanta, UNAIDS Country Co-ordinator for Liberia.
Related



Feature Story
West Indies cricketers support UNAIDS vision of eliminating new HIV infections among children
11 April 2012
11 April 2012 11 April 2012
Members of the West Indies Cricket Team, photographed with children who participated in the Think Wise coaching clinic and Dr Ernest Massiah, Director of the UNAIDS Caribbean Regional Support Team.
Credit: UNAIDS
Hosting a group of local students at the Kensington Oval stadium in Bridgetown, Barbados, the West Indies Cricket Team expressed solidarity with the UNAIDS vision of zero new HIV infections among children. The coaching clinic was held as part of the Think Wise Campaign, a global partnership that uses the power and reach of cricket to address key HIV-related issues.
"We have the medicines, we have the knowledge. There is no need for any Caribbean child to be born with HIV,” said West Indies Captain Darren Sammy, who endorsed the call for preventing mother-to-child transmission (PMTCT) of HIV and ensuring access to life-saving treatment for HIV-positive women. “There is no need to treat anyone any differently because of their HIV status," he added.
The Think Wise Campaign—a partnership between UNAIDS, UNICEF, the International Cricket Council and the Global Media AIDS Initiative—places particular emphasis on HIV prevention as well as on the education and empowerment of children. Engaging young people in the HIV response was the focus of the coaching session in Bridgetown, which included a discussion around HIV.
We have the medicines, we have the knowledge. There is no need for any Caribbean child to be born with HIV
West Indies Captain Darren Sammy
"Through this event, the children have loved meeting their favourite players and learning some new skills. At the same time, they have gained awareness about HIV and the importance of treating all people with equal respect and compassion,” said Dr Ernest Massiah, Director of the UNAIDS Caribbean Regional Support Team. “Like the cricketers, these children can be agents of change in their families, communities and schools."
A regional Elimination Initiative—led by the Pan American Health Organization—aims to end mother-to-child transmission of HIV in Latin America and the Caribbean by 2015. The Eastern Caribbean, with its smaller disease burden, is expected to reach the target far sooner.

West Indies Cricket Captain, Darren Sammy, participates in media interviews with Dr Ernest Massiah, Director of the UNAIDS Caribbean Regional Support Team, at the Kensington Oval stadium in Barbados.
Credit: UNAIDS
At present, mother-to-child transmission of HIV accounts for between 8 and 10 per cent of all HIV infections in the Caribbean. However, some Caribbean countries have either achieved or are close to achieving elimination targets; between 2007 and 2010, for example, there were no new HIV infections recorded among babies in Barbados.
Widespread stigma and discrimination against people living with HIV remains a challenge for PMTCT programmes across the region. Stigma and the fear of unfair treatment prevent some HIV-positive mothers from accessing early antenatal care, abstaining from breastfeeding or making their babies available for follow-up testing and care.
"The Eastern Caribbean can eliminate mother-to-child transmission because we have the means to prevent it," Dr Massiah stressed. "West Indian people can play a part by addressing the negative attitudes and judgments associated with HIV. This would allow mothers across our region to feel safe and confident about accessing life-saving testing, treatment, care and support."
External links
External links
Related

Feature Story
UNAIDS requests Pope Benedict XVI for support in efforts to stop new HIV infections in children
11 April 2012
11 April 2012 11 April 2012
UNAIDS Executive Director Michel Sidibé with the Pope Benedict XVI.
Credit: L'Osservatore Romano
The Executive Director of UNAIDS Michel Sidibé has asked for Pope Benedict XVI’s personal engagement in ending new HIV infections in children. During an audience with the Pope, Mr Sidibé spoke to him about how keeping children free from HIV was an achievable goal and, with concerted efforts, one which can be reached by 2015.
“Millions of people around the world living with and affected by HIV are being supported by catholic health care organizations,” said Mr Sidibé. “The full engagement of the Catholic Church in efforts to achieve zero new HIV infections among children is of paramount importance.”
The Vatican estimates that Catholic Church-related organizations provide approximately 25% of all HIV treatment, care, and support throughout the world. In 2010, the Vatican reported that more than 5,000 hospitals, 18,000 dispensaries, and 9,000 orphanages, many involved in AIDS-related activities, were being supported by the Catholic Church.
To reach the goal of ending new HIV infections in children by 2015, UNAIDS and partners launched a Global Plan towards the elimination of new HIV Infections among children by 2015 and keeping their mothers alive at the 2011 United Nations High Level Meeting on HIV/AIDS. The plan outlines a strategy which focuses particularly on the 22 countries that account for more than 90% of new HIV infections in children world-wide.
Following the audience Mr Sidibé met with Mr Michel Roy, Secretary General of Caritas Internationalis, a confederation of 164 Catholic relief, development and social service organizations operating in over 200 countries and territories worldwide. As a valued partner of UNAIDS, Caritas Internationalis serves as one of the civil society organizations represented on the steering committee of the Global Plan to eliminate new HIV infections in children.
The full engagement of the Catholic Church in efforts to achieve zero new HIV infections among children is of paramount importance
Michel Sidibé, Executive Director of UNAIDS
Faith-based organizations are instrumental in providing HIV related prevention, treatment care and support to people living with and affected by HIV. The World Health Organization has estimated that faith-based groups provide between 30% and 70% of all health care in Africa. During their in depth discussions about the Global Plan and on opportunities for further collaboration and strengthened partnerships in responding to HIV Michel Sidibé said, "No more babies born with HIV is an achievable goal. This is something we can get everyone to agree on as well as the importance of keeping their mothers alive.”
Mr. Michel Roy said: "The worldwide response to HIV has been a priority of Caritas Internationalis for the past 25 years. We will continue our commitment in this area. We strongly support the efforts to eliminate HIV infection among children. The Caritas ‘HAART for Children’ campaign shares a similar goal by promoting greater uptake of prevention of mother-to-child transmission programs and by assuring that children living with HIV, as well as their mothers, have access to early diagnosis and treatment."
Mr Sidibé subsequently met with Cardinal Peter Turkson, President of the Pontifical Council for Justice and Peace. In 2009, the Cardinal, originally from Ghana, served as one of the Co-Presidents of the Second Extraordinary Assembly for Africa or the Synod of Bishops. Under Cardinal Turkson’s leadership the Bishops discussed HIV, and in their final message, encouraged additional commitment from the Church to ending AIDS.
In their discussions Cardinal Turkson and Mr Sidibé talked about the AIDS epidemic in Africa, sustainable financing and HIV as a development issue.
“The response to HIV is a social justice issue,” said Mr Sidibé. “It is about a fairer allocation of resources within countries and especially their more equitable redistribution North-South.”
Speaking on the plan to eliminate new HIV infections in children Cardinal Turkson said, “With the medical technology readily available, making sure that children are born free of HIV-infection is a goal the human family can and should achieve, without delay, and would contribute to the human, economic and social development of the countries involved.”
Recognising the important work of the faith community in the AIDS response, UNAIDS established a strategic framework in 2009––to strengthen partnerships between UNAIDS and faith based organisations. The framework outlines the need for global and national religious leaders to take supportive public action in the AIDS response and strengthen the capacity of faith based organisations to work on HIV issues.
During his visit to Rome, Mr Sidibé also met with Staffan de Mistura, Under-Secretary of State of the Ministry of Foreign Affairs of Italy, with whom he discussed the importance of Italy maintaining its long tradition of leadership in the global AIDS response. Mr de Mistura expressed Italy’s strong support for UNAIDS vision of zero new HIV infection, zero discrimination and zero AIDS-related deaths, and particular interest in the global plan to end new HIV infections among children.



Feature Story
UNAIDS Executive Director urges young people in Morocco to drive a revolution in HIV prevention
05 April 2012
05 April 2012 05 April 2012
UNAIDS Executive Director Michel Sidibé (right) met with a group of young Moroccans on 4 April at the national headquarters of OPALS in Rabat.
Speaking with a group of young Moroccans on 4 April, UNAIDS Executive Director Michel Sidibé urged youth across the country—and region—to break the silence on AIDS and lead a revolution in HIV prevention.
“Young people were at the forefront of revolutions that brought political change to this region. I urge youth to launch a similar movement to stop new HIV infections,” said Mr Sidibé, addressing a group of young people at the national headquarters of OPALS (Organisation Pan Africaine de Lutte contre le sida), a non-profit organization based in Rabat.
Over the past decade, the number of new HIV infections among adults and children in the Middle East and North Africa increased from 43 000 to 59 000, according to UNAIDS estimates. In 2010, there were an estimated 470 000 people in the region living with HIV, up from 320 000 in 2001.
During the meeting, Mr Sidibé expressed concern over widespread stigma and discrimination in the region against people living with HIV and populations at high risk of infection, including sex workers, people who inject drugs and men who have sex with men. He noted that stigma drives vulnerable populations underground and away from HIV and health services.
Young people were at the forefront of revolutions that brought political change to this region. I urge youth to launch a similar movement to stop new HIV infections
UNAIDS Executive Director Michel Sidibé
Across the region, the special needs of youth—particularly sex workers, people who inject drugs, men who have sex with men and people living with HIV—remain inadequately addressed, noted the UNAIDS Executive Director. He underscored the importance of empowering all young people with the knowledge and resources they need to lead a healthy sexual lifestyle.
Through 17 drop-in clinics, OPALS provides health services, access to condoms and HIV testing for young people, women, migrants, sex workers and other vulnerable populations in Morocco. Representatives from OPALS also travel in remote areas, providing door-to-door HIV testing and other prevention services.
In the meeting with Mr Sidibé, several young people highlighted the lack of sexual education in Morocco—both at school and within families. They expressed enthusiasm for UNAIDS’ youth-led policy project CrowdOutAIDS, which leverages new technologies to enable young people to fully participate in the development of the organization’s strategy on HIV and youth. Since the launch of the project in October 2011, some 5000 young people around the world have taken part.
Reaching most-at-risk populations
During his three-day mission to Morocco, Mr Sidibé paid a visit to the Association de Lutte contre le sida (ALCS) in Rabat, the first AIDS association established in the Maghreb region and the Middle East. Mr Sidibé praised Hakima Himmich, President of ALCS, and her staff for the organization’s excellent contribution to the HIV response—particularly its efforts to prevent HIV among populations at high risk of infection.
ALCS was established in 1998 when there were just 30 registered cases of AIDS in Morocco. In 1992, ALCS opened its first voluntary HIV testing and counselling centre, and since 1995, the organization has offered HIV prevention programmes for key populations at high risk of infection.
By 2011, more than 122 000 people at high risk of infection—including vulnerable and bridge populations (for example, clients of sex workers)—were benefiting from HIV prevention programmes in Morocco, largely through ALCS. That same year, an estimated 58 000 people in Morocco were tested for HIV, many of them through ALCS.
According to studies conducted in 2011 by Morocco’s National AIDS Programme, ALCS and UNAIDS, 45% of sex workers and men who have sex with men in the country are currently reached through HIV prevention programmes and the rate of condom use among these key populations is about 50%.
During his visit to ALCS, Mr Sidibé sat in on a group discussion with women focused on HIV prevention. He also met a peer support group for people living with HIV and spoke with health personnel at an HIV testing centre.
Related

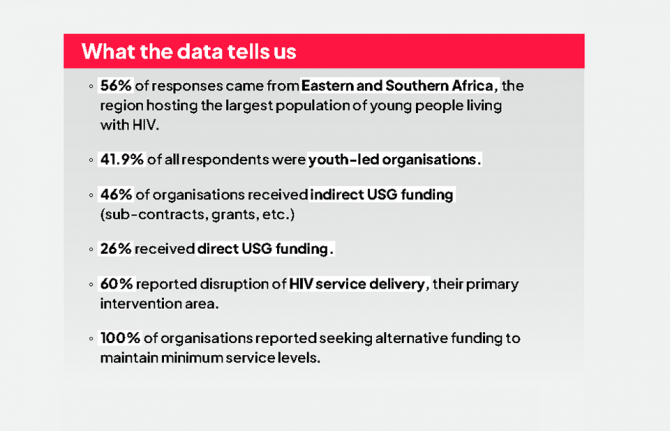
 “Who will protect our young people?”
“Who will protect our young people?”
02 June 2025
Feature Story
Morocco launches new national AIDS strategy
04 April 2012
04 April 2012 04 April 2012
UNAIDS Executive Director Michel Sidibé met with Princess Lalla Salma of Morocco on 4 April in Rabat.
Credit: Le Matin.ma
Morocco has a low national HIV prevalence, estimated at approximately 0.15% of the general population. However, recent data show a concentrated and growing HIV epidemic in the country among key populations.
According to government figures, an estimated 5.1% of men who have sex with men are living with HIV nation-wide. In the south-western city of Agadir, HIV prevalence among sex workers is about 5%. In Nador, a coastal city in the north-east, nearly one in five people who inject drugs is HIV-positive.
Focusing resources on populations at high risk of HIV infection is at the core of a new national AIDS strategy in Morocco. Launched in Rabat on 3 April by the Minister of Health, El Hossaine Louardi, Morocco’s five-year strategy is closely aligned with the targets of the 2011 Political Declaration on AIDS.
Addressing an audience of more than 300 national partners in the AIDS response—including government officials, civil society representatives and people living with HIV—Mr Louardi said that the national plan aims to halve new HIV infections and reduce AIDS-related deaths by 60% by the year 2016. He added the strategy is based on the principles of a right to health, accountability and inclusion of all partners in the HIV response.
Speaking at the launch ceremony, UNAIDS Executive Director Michel Sidibé called Morocco’s HIV response “exemplary,” with people placed squarely at the centre of national development efforts. He praised Morocco as a regional pioneer in protecting the health and human rights of vulnerable populations.
Morocco was the first Arab country to introduce harm reduction programmes for people who inject drugs, including methadone maintenance therapy and needle-syringe programmes. Evidence has shown that such programmes are essential to prevent the spread of HIV among key populations.
A new funding paradigm is needed in Morocco and across the African continent—one that is written and owned by African countries
UNAIDS Executive Director Michel Sidibé
Mr Sidibé recognized in his remarks a new medical assistance scheme for the country’s low-income population called RAMED (Régime d’Assistance MÉdicale des Economiquement Démuni). Under RAMED, 8.5 million Moroccans living below the poverty line, or just under 30% of the population, will benefit from partial or total exemption from treatment costs at public hospitals.
“RAMED is an important reform for social justice and the redistribution of opportunity,” said Mr Sidibé. “Providing vulnerable populations with social protection is a key strategy in the HIV response,” he added.
Recognizing Princess Lalla Salma’s contribution
Earlier in the day, Mr Sidibé met with Princess Lalla Salma of Morocco, wife of King Mohammed VI and President of the Association Lalla Salma de Lutte contre le Cancer, a national non-profit organization. He thanked the Princess for her participation in last year’s UN General Assembly High Level Meeting on AIDS and for her on-going advocacy and support for programmes aimed at improving the health of women and children. In recent years, the Princess has been a leading voice in promoting the importance of integrated services for reproductive health and cervical cancer.
A call for reduced dependency on external HIV aid
In a separate meeting with Morocco’s Minister of Health, Mr Sidibé thanked the Minister for his efforts to push forward the Arab AIDS Initiative at a recent conference in Jordan. The new initiative is expected to accelerate national and regional efforts to achieve the targets of the 2011 Political Declaration on AIDS.
Noting that Morocco relies on external aid to fund 50% of its national AIDS response, Mr Sidibé urged the country’s leadership to assume a greater share of HIV investments. “A new funding paradigm is needed in Morocco and across the African continent—one that is written and owned by African countries,” he said.
Underscoring that a vast majority of HIV drugs prescribed in Africa are imported, Mr Sidibé called for the local production of antiretroviral medicines. He spoke of the need for a single African drug regulatory agency to ensure the faster roll-out of quality-assured medications across continent.
Related


Feature Story
UNAIDS Executive Director praises Algeria as a regional leader and pioneer in the HIV response
03 April 2012
03 April 2012 03 April 2012
UNAIDS Executive Director Michel Sidibé (left) met with the President of the Algerian Senate, Abdelkader Bensalah, at the Council of the Nation headquarters in Algiers on 2 April.
Algeria’s early and swift response to the HIV epidemic has kept national HIV prevalence low, at approximately 0.1% of the population. Since 1998, the government has offered free antiretroviral treatment to all people who are eligible. New HIV infections among children in Algeria have been virtually eliminated.
In a meeting on 2 April with the President of the Algerian Senate, Abdelkader Bensalah, UNAIDS Executive Director Michel Sidibé commended Algeria as a champion in the AIDS response—both at home and across the region.
During his meeting with Mr Bensalah at the Conseil de la Nation headquarters in Algiers, Mr Sidibé acknowledged the critical role that Algeria has played in mobilizing high-level commitment for the AIDS response within the African Union and in the League of Arab States. He noted that Algeria’s Chairmanship of the Group of 77 (G-77) provides an important platform for galvanizing further support for the regional response to HIV.
Touching on a theme from his recent missions in Africa, Mr Sidibé praised Algerian leaders for funding more than 93% of national HIV programmes through domestic sources. “Across Africa, too many countries remain too dependent on external HIV aid. Algeria’s country-owned HIV response is an example for others to follow,” he said.
Speaking on behalf of President Abdelaziz Bouteflika, Mr Bensalah underscored that the Algerian government hopes to finance 100% of its AIDS response in the coming years. He said that Algeria is committed to the targets of the 2011 Political Declaration on AIDS and to the UNAIDS vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths.
A call for a more inclusive society
Religion must play an important role in preventing HIV and addressing questions around drug use and sexuality
Algeria’s Minister of Religious Affairs, Mr Bouabdellah Ghlamallah
Meeting later in the day with Algeria’s Minister of Religious Affairs, Mr Bouabdellah Ghlamallah, Mr Sidibé requested the Minister’s support in ensuring a more inclusive society based on tolerance, compassion and respect for all human beings. He said that people of Islamic faith could promote HIV prevention by serving as a bridge between scientific evidence and social change.
Mr Ghlamallah reaffirmed the Ministry’s support for people living with HIV and populations at high risk of HIV infection. He said that the Ministry would continue to support El Hayet—a non-governmental organization of people living with HIV—in its efforts to reach the goal of zero discrimination.
“Religion must play an important role in preventing HIV and addressing questions around drug use and sexuality,” said the Minister.
Partnership to promote AIDS research

UNAIDS Executive Director Michel Sidibé (left) and the Algerian Minister of Health, Dr Djamel Ould Abbès, signed an agreement on 2 April to create an African AIDS Research Centre in Tamanrasset, Algeria.
During his mission, the UNAIDS Executive Director signed an agreement with the Minister of Health, Dr Djamel Ould Abbès, to establish an African AIDS Research Centre in Tamanrasset, a city in southern Algeria. Scheduled to open in 2013, the Centre will facilitate the regional exchange of scientific knowledge and expertise in the domain of HIV and public health.
“This is a ‘win-win’ partnership between UNAIDS and the Government of Algeria,” said Dr Ould Abbès, noting that the collaboration would marry the technical expertise of UNAIDS with Algeria’s national resources and regional contacts.
Addressing stigma and discrimination
Speaking with key partners in the HIV response on 1 April—including health professionals, government officials, AIDS activists, people living with HIV and representatives of the United Nations—Mr Sidibé underscored the need to intensify national and regional efforts to eliminate stigma and discrimination.
“Stigma drives people living with HIV and populations at high risk of HIV infection underground,” said Mr Sidibé. “It prevents vulnerable populations from accessing the HIV and health services they need.”
Publications
Publications



Feature Story
New initiative launched to deliver better, cheaper medicines to Africa
02 April 2012
02 April 2012 02 April 2012
UNAIDS Deputy Executive Director, Programme Dr Paul De Lay speaking at the launch of the East African Community (EAC) Medicines Registration Harmonization Project in Arusha, Tanzania, on 30 March 2012.
The need to ensure that people in Africa have access to essential, high quality, safe and affordable medicines has just received a major boost with the launch of the East African Community (EAC) Medicines Registration Harmonization Project in Arusha, Tanzania, on 30 March 2012.
The project is a high-level alliance bringing together the New Partnership for Africa’s Development (NEPAD), the World Health Organization (WHO), the Bill & Melinda Gates Foundation, the World Bank, the UK Department for International Development (DfID), and the Clinton Health Access Initiative (CHAI). The Arusha launch marks the starting point in the implementation of the broader African Medicines Regulatory Harmonization Programme across the continent.
The partners hope to strengthen regulatory capacity and systems for medicines in Africa, including antiretroviral drugs, so that fewer lives are lost due to drugs which are unsafe and of poor quality or which are largely unavailable or delivered inefficiently. These existing challenges can be attributed to a range of factors which include lack of human and financial resources, insufficient infrastructure, weak medicine legislation and a lengthy drug approval cycle caused by low regulatory capacity and inefficient processes.
“Access to safe, affordable and quality medicines for the treatment of common diseases remain out of reach to many people in the East African region as a whole,” said Dr Richard Sezibera, Secretary General of the East African Community. “The programme we are launching here today will put in place a uniform and standardized medicines regulatory framework for both good health outcomes and economic gains.”
The programme we are launching here today will put in place a uniform and standardized medicines regulatory framework for both good health outcomes and economic gains
Dr Richard Sezibera, Secretary General of the East African Community
The launch was attended by ministers, representatives from regional and pan-African bodies, international organizations and donors. One of the key arguments endorsed by those at the launch was the critical need to produce creative, African sourced solutions, responsive to the particular needs of African people.
This would encourage local production of medicines—such as antiretroviral therapy for people living with HIV—in partnership with other emerging economies like the BRICS group (Brazil, Russia, India, China, South Africa). In addition it would strengthen African control of development investments through more diversified funding sources which would reduce Africa’s dependence on external factors.
At present, Africa is heavily reliant on imported medicines. 80% of the antiretrovirals keeping more than 5 million African people alive come from abroad. In addition, two thirds of all AIDS expenditures in Africa come from external sources.
According to UNAIDS Deputy Executive Director, Programme Dr Paul De Lay, who attended the launch, creating an African Medicines Regulatory Agency would allow faster roll out of drugs, stronger quality assurance, greater public confidence and the enhancement of African ownership of a sustainable AIDS response.

(L to R) UNAIDS Deputy Executive Director, Programme Dr Paul De Lay, Ambassador Dr Richard Sezibera, Secretary General of the East African Community and UNAIDS representative for African Union.
“Regional regulatory agencies will deliver a range of benefits” said Dr De Lay. “Things will be faster, more efficient and fairer,” he added.
UNAIDS believes that such regional initiatives are an essential component of a successful response to HIV. These initiatives will provide a strong platform for advocacy, coordination and regulation to make high quality drugs more widely available across the continent.
An African Medicines Regulatory Agency would additionally allow a more rapid and far reaching response to reports of possible counterfeit or tainted drugs. It will also enhance capacity to test suspect batches of medicine. Such increased regional pharmacovigilance would protect health and save lives. It is hoped that the African Medicines Regulatory Harmonization Programme can help maintain the considerable progress made in the health sector in recent years.
