
, UNAIDS Country Director for Kenya Jantine Jacobi said, “We need to listen to the lived experiences of women living HIV to ensure that services meet their needs.”")
, UNAIDS Country Director for Kenya Jantine Jacobi said, “We need to listen to the lived experiences of women living HIV to ensure that services meet their needs.”")
, UNAIDS Country Director for Kenya Jantine Jacobi said, “We need to listen to the lived experiences of women living HIV to ensure that services meet their needs.”")
Feature Story
Advocating for zero discrimination in health-care settings in Kenya
08 May 2018
08 May 2018 08 May 2018Like many women in sub-Saharan Africa, women in Kenya are disproportionately affected by HIV. In 2016, 34 000 adult women became newly infected with HIV, compared with 22 000 adult men, and adult women accounted for 910 000 of the 1.6 million people living with HIV in the country.
Women also face challenges with sexual and reproductive health issues, such as limited access to family planning, as well as stigma and discrimination when they seek services.
To identify solutions to such challenges facing women in Kenya, the nongovernmental organization Women Fighting AIDS in Kenya (WOFAK) recently held a two-day workshop on 25 and 26 April in Nairobi, Kenya, on advancing the sexual and reproductive health and rights of women living with HIV. More than 30 women living with HIV from across the country met with representatives of the government, civil society and United Nations agencies to take stock and agree a pathway to implement the World Health Organization’s (WHO) Consolidated guideline on sexual and reproductive health and rights of women living with HIV.
“A woman-centered approach must guide a more responsive delivery of services for women living with HIV,” said Dorothy Onyango, co-founder of WOFAK, at the start of the meeting.
To guide effective implementation of the guideline at the country level, the Salamander Trust, with support from WHO, developed a checklist to support women living with HIV to organize and coordinate their own advocacy and ensure their meaningful engagement. The checklist was first used in Kenya and will be rolled out to other countries.
During the meeting, Rukia Ahmed, founder and chairperson of a support network for Kenyan Muslim women living with HIV in north-eastern Kenya, said, “Most women only find out about their HIV status when they are pregnant or very ill. Confidentiality is an issue. When their status is disclosed, some are not accepted by their family afterwards, leading to isolation.”
Ms Ahmed is now going to advocate for discrimination-free health-care settings. “I’m going to visit district hospitals and raise awareness among health-care workers and support groups on the right to stigma-free health care. Change is possible,” she said.
“What stood out for me was the message that as women living with HIV we need to accept ourselves and love ourselves first and as a result we will be able to fight for our rights,” said Joyce Ouma, from Sauti Skika, a network of young people living with HIV.
It is a message Ms Ouma hopes to bring to her peers. “Initially, I did my advocacy out of obligation. Now I want to do it because I have the drive and I know it is important for me first,” she said.
At the conclusion of the meeting, Jantine Jacobi, the UNAIDS Country Director for Kenya, said, “We need to listen to the lived experiences of women living HIV to ensure that services meet their needs.”
Related






Feature Story
UNAIDS ambassadors speak out to stop discrimination
25 April 2018
25 April 2018 25 April 2018Everyone will have experienced stigma and discrimination of some kind during their lives; however, non-discrimination is a human right. As part of UNAIDS' work to achieve zero discrimination, UNAIDS encourages people to speak up and prevent discrimination from standing in the way of achieving ambitions, goals and dreams.
Two UNAIDS ambassadors recently took part in a dialogue with students at Peking University about the need to achieve zero discrimination to end the AIDS epidemic and ensure better health for all.
The First Lady of Panama, Lorena Castillo de Varela, UNAIDS Special Ambassador for AIDS in Latin America, and the famous actor and humanitarian, Huang Xiaoming, UNAIDS Goodwill Ambassador for China, spoke about their commitment to reducing stigma and discrimination at an event on 24 April. The dialogue was opened by the Vice-President of Peking University, Zhan Qimin.
During the lively discussion between the two ambassadors, the First Lady encouraged young people to integrate their antidiscrimination efforts into their everyday actions. “Just that smile, even though it might look very small to you, it can make another humanbeing feel special, not discriminated or different,” said Ms Castillo.
Discrimination has many forms, from racial or religious discrimination to discrimination based on gender, sexual orientation or age, and to bullying at school or at work. In only three out of 10 countries worldwide do equal numbers of girls and boys attend upper secondary school, and people living with disabilities are nearly three times more likely to be denied health care than other people.
Ms Castillo stressed that the important role that the young generation has to play in taking the lead. “I want to use this platform to send messages to all the universities in the world, they should all follow your lead too, and give voices to those who have no voices, be the voice for them, let them know that there’s somebody somewhere sending them love, fighting for them.”
Mr Huang explained what had motivated him to start working on zero discrimination and become a UNAIDS Goodwill Ambassador. “I had seen children who suffered from discrimination related to HIV. Their inner repression, touched me and made me start to think about how I could help them. Of course discrimination is not limited to just children. So when I learned that UNAIDS had the goal of ending AIDS worldwide by 2030, I was very excited and willing to do my best for this goal.”
A piece of advice to young people from Mr Huang moved everyone in the meeting hall: he quoted a line from the film Wonder, "When given the choice of being right and being kind, choose kind—I believe it is important to be kind to everyone, it’s particularly important to keep our minds clear and objective, and to uphold justice and truth".
Ran Wei, a representative of UNAIDS, thanked the two ambassadors for their tireless efforts championing zero discrimination and urged students to follow their lead. “It is not only a responsibility, but also a privilege for youth, to fight for a world that’s healthy, just and free from discrimination,” she said.
Region/country
Related










Feature Story
The injustices faced by transgender women in Peru
26 April 2018
26 April 2018 26 April 2018Tamara, a transgender woman from Lima, Peru, had struggled with her identity since elementary school, where she was bullied so intensely by her peers that she dropped out. When she was 18 years old, with few options for her, she began working on the streets as a sex worker. Tamara often said that she wasn’t going to live past 30. How could she, she asked defiantly, when society treats her as less than human?
Like a self-fulfilling prophecy, Tamara died less than a month after her 30th birthday from an AIDS-related illness and tuberculosis. Her death at such a young age is sadly common, as most transgender women in Latin America die before they reach 35. Latin America leads the world in homicides of transgender people — nearly 80% of global transgender homicides occur in the region. And HIV prevalence among transgender women is as high as 38% — transgender women are 50% times more likely to acquire HIV than the general population, according to a recent study in the Journal of the International AIDS Society.
The human rights violations perpetrated against transgender women throughout Latin America are the result of forces in society. The region’s highly machismo, conservative and transphobic culture ostracizes and stigmatizes transgender people, posing a serious threat to their health, security, life expectancy and employment prospects. With few options or support, many engage in sex work. As sex workers with no legal protections, they are at a greater risk of violence and sexual and substance abuse. And most have little access to health services. Without recognition, many cases of violence and murder go undocumented.
Photojournalist Danielle Villasana has been documenting a community of transgender women in Lima for the past several years, photographing the often dire realities they face, such as complications from HIV, abuse from police, partners and clients, and death. “Because most governments throughout Latin America and the world continuously fail to protect transgender women, I’m determined to show how these largely ignored injustices often lead to deadly consequences,” she said.
As a result, Ms Villasana has launched a Kickstarter campaign to publish these important stories as a bilingual photobook. The aim is to raise awareness among the police, medical institutions and lawmakers — sectors she says that are often ignorant of the abuse against transgender women because of institutional prejudice and lack of understanding. You can support and learn more about her book project at http://bit.ly/a-light-inside.
From a young age, transgender people face stigma, discrimination and social rejection in their homes and communities. Such discrimination, violence and criminalization prevent transgender people from getting the HIV services they need to stay healthy. UNAIDS is working with governments, partners and transgender communities to increase access to health services for transgender people.
All photos by Danielle Villasana
Danielle Villasana
Region/country
Related





Feature Story
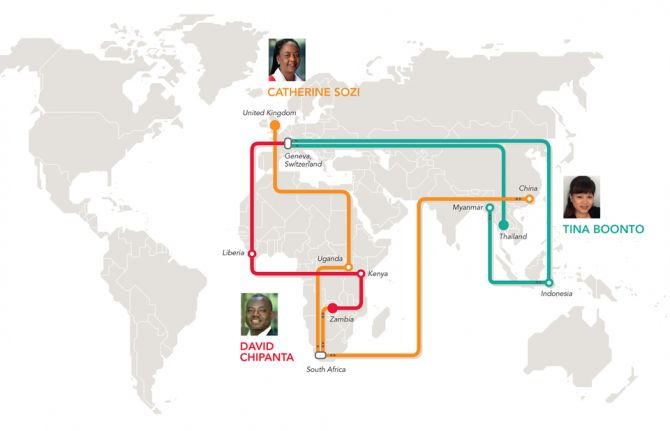
Bringing about change
25 April 2018
25 April 2018 25 April 2018David Chipanta started his UNAIDS career in Liberia as the UNAIDS Country Director, where he helped to strengthen the national AIDS commission and national strategy framework. He is particularly proud of putting gender and ending sexual violence front and centre in the AIDS response in the country and giving the national network of people living with HIV more of a voice.
“What I found exciting was tackling the many barriers that surround access to HIV treatment, prevention, care and support,” he said. By barriers, he means the stigma, discrimination, poverty and inequalities that constrain people from accessing HIV services.
An economist by training, Mr Chipanta remarked, “We cannot forget the importance of all the things that relate to people’s lives—do they feel secure, do they have food, do they have a house, a family, a job?” Giving the example of Zambia, he described some people only taking their HIV medicine during the rainy season because food is more readily available then.
“It hit me that the peripheral stuff is very important, because without it HIV services will have a limited impact,” Mr Chipanta said. His current job as the UNAIDS Social Protection Senior Adviser in Geneva, Switzerland, focuses on just that—connecting people affected by HIV to social safety nets and improving livelihoods, as well as reducing poverty and improving education.
“UNAIDS has created more awareness about social protection services and the hurdles that people living with HIV face,” he said. For example, he explained that in Liberia and Sierra Leone, sex workers said they weren’t accessing social protection services because the administrators often treated them badly; in response, his office set up sensitivity training.
Another issue close to his heart is girls’ education. Keeping girls in school has been shown to lower HIV prevalence and is an important factor in increasing access to HIV treatment. “In low-income settings, we shone the light on the importance of cash transfers to keep girls in school,” Mr Chipanta said. His next challenge is advocating for more synergies with programmes for mentoring, empowerment and social support.
“As a person living with HIV, I never thought I would accomplish so much,” he said. In 1991, when he found out his HIV status in his native Zambia, he assumed that his life was over. “I thought, before I die, let me help others,” he added.
“I was personally motivated to work in the HIV field,” he said. “But I felt like I wanted to become an expert in my own right.”
Krittayawan (Tina) Boonto reflected on her 20 years at UNAIDS by also saying she couldn’t believe how far she had got. Ms Boonto started work in her native Thailand before moving to Geneva.
“It was supposed to be temporary, but I stayed seven years,” she said.
She then went to Indonesia as the Programme Coordination Adviser in 2005. She helped the Ministry of Health with technical support and accessing financial resources from the Global Fund to Fight AIDS, Tuberculosis and Malaria. That experience proved pertinent, because in 2010 she moved to Myanmar as the Senior Investment and Efficiency Adviser.
“The country was opening up at that time, so my field experience in other countries came in handy,” she said. For example, UNAIDS advocated to decentralize the provision of antiretroviral medicines so that people from rural areas could get their treatment at primary health-care centres without traveling to the main cities.
“It was so rewarding to be on the ground and witness the change.” According to Ms Boonto, antiretroviral medicine access shot up to more than 120 000 people accessing the medicines, up from 30 000 people in three years.
“That’s when I realized that it’s not just about money, it’s also about the willingness to change,” she said.
A year ago, she returned to Indonesia, but this time as the UNAIDS Country Director. It’s been challenging for her because despite the scale-up when she was in the country the first time, Indonesia lags behind its neighbours, such as Thailand and Myanmar, in terms of antiretroviral medicine access and reducing new HIV infections. “It ranks third after India and China in the region in terms of new HIV infections,” Ms Boonto said.
Her tactic has been to raise HIV awareness among decision-makers and stress to them that the epidemic is not under control. “We present data and push to keep HIV a priority,” she said. Recently, she has been knocking on doors to raise alarm bells about tuberculosis—a disease that remains one of the leading causes of death among people living with HIV, despite being treatable and preventable.
“It all boils down to political will and getting the autonomous country districts on board once the Ministry of Health approves,” she said. Not flinching, Ms Boonto said, “My job never lets me forget what I am working for: people living with HIV.” She added, “We are still relevant and are still much needed, and that is the greatest satisfaction of all.”
Satisfaction for Catherine Sozi has been observing the shift from, “How can we roll out treatment for so many people, to getting 21 million people on treatment in the space of 10 plus years,” she said. In her third stint in South Africa, she feels UNAIDS’ advocacy work has paid off. Recalling a conversation she had in Zambia with the government when she worked there 15 years ago, many feared that the money and support would not come if countries started to offer antiretroviral medicines. “I made the case that money would come based on the countries’ growing commitment and that we would work to get the prices down,” she said. In 2005, prices for antiretroviral medicines were high. “The governments listened to us and to civil society and, based on solid results in 2015, it suddenly looked feasible to put an end to AIDS,” Ms Sozi said.
As the Regional Director for the eastern and southern Africa region, she is thrilled by the positive energy in the region, despite the many challenges remaining. “A lot still needs to be done to stop new HIV infections, get even more people on treatment and have them stay on treatment, and that includes testing even more adolescents, children and adults for HIV, including key populations,” she said. Another big issue involves tackling rampant sexual violence, which leads in part to higher numbers of new HIV infections among girls and young women, she explained.
“In this case, a biomedical response won’t help. We need to change how we relate to households, the police and the legal system and get faith leaders, women activists, nongovernmental organizations and men involved to turn things around,” Ms Sozi said. Trained as a doctor in Uganda, she admits that her career has propelled her into a much wider arena than she had ever anticipated.
“The UNAIDS women’s leadership programme empowered me to become a leader and reassured me that I could manage a large, diverse staff as well as resources and still be technically strong,” she said.
Her four years as the UNAIDS Country Director in China, before her latest move to South Africa, proved to be very enriching on a personal and professional level. “As a family we had a wonderful time in a country that is in itself so diverse in all aspects,” she said. The commitment by the government and civil society to work on the epidemic was both invigorating and challenging.
One of her biggest accomplishments in Asia was her contribution to the China–Africa health dialogue. “For me, to support the South–South dialogue on China–Africa health cooperation meant a lot,” Ms Sozi said. “I see myself as a facilitator of change.”
MORE IN THIS SERIES
UNAIDS staff share global experience on AIDS through criss-crossing the world
It’s about the people we serve: UNAIDS staff connecting the world
More in this series




Feature Story
An historic opportunity to end AIDS in Africa
20 April 2018
20 April 2018 20 April 2018A decade of progress has inspired the once unthinkable—that the AIDS epidemic can be ended as a public health threat. A decade of transformation has set the stage, and the global community is united behind the goal of ending AIDS by 2030.
Progress in eastern and southern Africa, the world’s most affected region, is driving global optimism. In the region, the number of people living with HIV on antiretroviral therapy has more than doubled since 2010, reaching almost 12.5 million people by June 2017. New HIV infections in eastern and southern Africa have declined by a third in just six years, while AIDS-related deaths in the region plummeted by 42% over the same period.
A new report released by UNAIDS shows that ending the AIDS epidemic in Africa can be reached if investments are secured and plans are in place for long-term sustainability.
The report, Turning point for Africa: An historic opportunity to end AIDS as a public health threat by 2030 and launch a new era of sustainability recommends developing country-tailored sustainability plans to enable transition towards domestic ownership and financing at each country’s own pace. It also highlights that sustainable progress will require changing policies, increasing human resources for health, increasing efficiencies and addressing systemic inequalities.
The Executive Director of UNAIDS Michel Sidibé presented the new report to African Ministers of Finance, multilateral partners and other senior officials at a meeting on optimizing investments and partnerships to end AIDS in Africa organized by the United States Department of Treasury and the United States President’s Emergency Plan for AIDS Relief (PEPFAR).
“We get a remarkable return from investments in HIV programmes—increased life expectancy, stronger economic productivity, and decreasing health care costs over time as people stay healthy,” said Mr Sidibé. “Governments have set ambitious goals and we are closer than ever before to success. We have broken the epidemic’s trajectory. PEPFAR and Global Fund have driven this progress under the leadership of your governments. We can all take pride in what has been achieved.”
The report shows that by adopting UNAIDS Fast-Track Targets instead of continuing business as usual, more than 15 million new HIV infections can be averted and more than 5 million lives saved. Moreover, it will avert US$ 4.7 billion of financial resources needed for treatment in sub-Saharan Africa 2017–2030, from which eastern and southern Africa accounts for US$ 1.7 billion and western and central Africa US$ 3 billion.
In opening remarks, Eric Meyer, Deputy Assistant Secretary for Africa and the Middle East, United States Treasury, underscored the importance of health investments to the productivity of national workforces, long-term strength of economies and the ability of Ministers of Finance to reach their goals for economic growth.
Deborah Birx, United States Global AIDS Coordinator and Special Representative for Global Health Diplomacy, briefed on progress and gaps in the HIV response and the tremendous progress towards epidemic control in many countries.
Peter Sands, Executive Director of the Global Fund to Fight AIDS, Tuberculosis and Malaria, focused on the need to for efficiency and effectiveness and focused programming. “We have the very real prospect of being able to end the epidemic—control it effectively—we know what to do. But it does require more investment in a sustained and highly coordinated fashion.”
The meeting was held in Washington, DC, United States of America, on 19 April, during the annual World Bank Spring Meetings, which bring together finance and development officials, private sector executives and civil society from around the world to discuss issues of global concern.
Turning point for Africa






Feature Story
Mumbai Fast-Tracks AIDS response by spearheading innovations to end epidemic by 2030
19 April 2018
19 April 2018 19 April 2018Population growth and fast urbanization, fuelled by sustained immigration and accelerating mobility, are rapidly changing the socioeconomic and behavioural patterns of people in big cities.
Mumbai, a city of 12 million people, was one of the first cities to sign up to the Fast-Track cities initiative, launched in Paris on World AIDS Day 2014. Since then it has rapidly adopted measures to accelerate progress towards achieving the Fast-Track 90-90-90 treatment targets. However, the challenge today goes beyond scaling-up efforts to attain the 90-90-90 targets. Efforts to end AIDS must also focus on effective use of combination HIV prevention and eliminating the stigma and discrimination that impede universal access to health services.
The Mumbai District AIDS Control Society and UNAIDS brought together more than sixty participants from government, international and civil society organizations from 10 to11 April to identify innovative strategies to expand HIV prevention and treatment service coverage in the megacity.
Participants noted that growing inequalities in the urban environment were forcing people to take risks to survive. Sex workers, people who inject drugs, men who have sex with men and transgender people (Hijras) who are already at higher risk of HIV infection are particularly negatively impacted by these trends.
Urban gentrification is pushing key populations out of areas where they had previously gathered making the task of delivering HIV services more complicated. As populations have become more dispersed and hidden, traditional HIV prevention outreach approaches using peer workers have become less effective.
Reflecting on these challenges, participants noted that with change came opportunity. More systematic compilation of data and granular analysis has helped identify locations and populations where risk and vulnerability are greatest. According to city officials, improved data and understanding is helping to refine their approach to HIV prevention interventions. New packages of services designed through the profiling of newly emerging risk behaviours are being planned.
To further Fast-Track the AIDS response, several new approaches have been introduced. Community-based HIV screening helps to accelerate diagnosis and treatment of people living with HIV. Similarly, in growing slum areas mobile vans offering HIV testing services provide the opportunity to large numbers of people to know their HIV status.
While social media platforms are proving a cost-effective means to improve HIV awareness and connect people to prevention and treatment services, Mumbai authorities are convinced that more innovative communication strategies are also necessary. They plan to use social and mass communication media to mobilize support to ‘normalize’ AIDS as a chronic disease and prevent new HIV infections. HIV champions will target a range of different audiences including adolescents and young people to amplify HIV prevention messages.
All participants agreed that efforts to scale up access to HIV services need to be led at a faster pace as “there is no time to lose” to end AIDS by 2030.
Region/country



Feature Story
Ending the AIDS epidemic among children, adolescents and young women
27 April 2018
27 April 2018 27 April 2018Ending the AIDS epidemic among children, adolescents and young women requires ambitious targets and a Super-Fast-Track approach. Building on the successes of the Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive, UNAIDS, the United States President’s Emergency Plan for AIDS Relief (PEPFAR) and partners* launched Start Free Stay Free AIDS Free in 2016 to provide a framework for the urgent work ahead.
Start Free Stay Free AIDS Free prioritizes action in 23 countries** that account for 87% of new HIV infections among children aged 0–14 years and approximately 87% of all children and adolescents living with HIV globally. In 2016, 2.1 million children were estimated to be living with HIV.
In its first progress report, Start Free Stay Free AIDS Free reflects on the achievements made during the first year of implementation and highlights areas where urgent action is needed.
“The world is on the Fast-Track to eliminating new HIV infections among children and ensuring that their mothers are alive and healthy, but we need to do more to ensure that all children living with HIV have access to treatment immediately,” said Michel Sidibé, Executive Director of UNAIDS.
The report shows that globally in 2016, there were 160 000 new HIV infections among children and that 140 000 occurred in the 23 priority countries. Although there was an overall decline in new HIV infections, the decline was at a much slower rate than in previous years.
The report highlights concerns around new HIV infections among young women and girls. In 2016, around 200 000 adolescents between the ages of 15 and 19 years were newly infected with HIV in the 23 priority countries, 72% of whom were young women.
Most—more than 70%—of all new HIV infections among young people are in sub-Saharan Africa, which also has the fastest growing youth population in the world.
“A high number of new HIV infections among adolescents and a fast-growing population could make for an HIV explosion among young women in Africa,” said Deborah Birx, United States Global AIDS Coordinator and Special Representative for Global Health Diplomacy. “The United States Presidents Emergency Plan for AIDS Relief is driving harder and smarter to prevent HIV infections and ultimately help end AIDS among children, adolescents and young women. Every person deserves the chance to survive, thrive and pursue their dreams.”
Gains seen in access to treatment
The report shows that while important gains have been made in access to antiretroviral therapy for pregnant women living with HIV, much more needs to be done to reach children.
In 2016, around 78% of pregnant women living with HIV had access to antiretroviral therapy in the 23 priority countries.
Start Free targets
Reduce new HIV infections among children to 40 000 by 2018.
Reach and sustain 95% of pregnant women living with HIV with lifelong HIV treatment by 2018.
Stay Free targets
Reduce the number of new HIV infections among adolescents and young women to less than 100 000 by 2020.
Provide voluntary medical male circumcision for HIV prevention to 25 million additional men by 2020 globally, with a focus on young men aged 10–29 years.
AIDS Free targets
Ensure that 1.6 million children (0–14 years) and 1.2 million adolescents (15–19 years) living with HIV have access to antiretroviral therapy by 2018.
The increase in the roll-out and uptake of antiretroviral therapy during pregnancy and throughout breastfeeding is estimated to have averted around 270 000 new HIV infections among children in 2016 alone.
The numbers of children on treatment has also increased, but not on a big enough scale. In 2010, only 17% of children aged 0–14 years had access to treatment. By 2016, that had risen to around 43%, with around 920 000 children accessing antiretroviral therapy. Although this is a marked improvement, access to treatment for children still falls far behind access for adults. In 2016, around 54% of adults living with HIV had access to treatment.
The report cites multiple reasons for the slow growth of access to treatment for children, including poor testing rates. Only nine of the 23 priority countries managed to test and diagnose 50% or more of children who were exposed to HIV in 2016. There are particularly low rates of early infant diagnosis in the first two months of life, when it is most important to test, as HIV-related mortality is at its highest. Without access to testing and treatment, half of all children living with HIV will die before their second birthday.
Ways forward
The report offers a set of important actions countries can take to eliminate new HIV infections among children, to test and diagnose children and young people who may have been exposed to HIV and to ensure that children and young people access HIV prevention, quality medicines and age-appropriate sexual and reproductive education and care and support throughout their lives, free from stigma and discrimination.
Other important actions include accelerating new medicines and diagnostics, promoting community engagement and services, voluntary medical male circumcision, access to information on sexual and reproductive health and access to pre-exposure prophylaxis for young people at a higher risk of HIV.
“The future for children and adolescents depends on actions we take collectively today,” said Mr Sidibé.
The latest estimates, for the end of 2017, will be released in July 2018 and will provide further insight into the progress of Start Free Stay Free AIDS Free.
* United Nations Children’s Fund, World Health Organization and the Elizabeth Glaser Pediatric AIDS Foundation.
**Angola, Botswana, Burundi, Cameroon, Chad, Côte d’Ivoire, Democratic Republic of the Congo, Ethiopia, Ghana, Kenya, Lesotho, Malawi, Mozambique, Namibia, Nigeria, South Africa, Uganda, United Republic of Tanzania, Swaziland, Zambia and Zimbabwe.
Start Free Stay Free AIDS Free



Feature Story
Reaching people who inject drugs with HIV services in Finland
27 April 2018
27 April 2018 27 April 2018The Aurora Day Centre in Helsinki, Finland was founded in December 2000 in response to a sharp increase of new HIV infections among people who inject drugs. The centre had an immediate impact and dramatically increased the number of people linked to treatment and care.
During a visit to Helsinki the Executive Director of UNAIDS, Michel Sidibé, met with staff at the centre to learn how their services are supporting people in the city.
According to Day Centre staff, prior to the opening 53% of people who inject drugs who were living with HIV were retained in care—by 2014, 90% were retained in care and accessing antiretroviral therapy.
The number of people who inject drugs who were newly infected with HIV was reduced by half between 2007 and 2016 in Finland – source ECDC
The main aim of the centre is to prevent new HIV infections among people who inject drugs and to provide harm reduction services including opioid substation therapy. The centre currently has around 77 clients, with an average age of 50 years old. Many became infected with HIV before harm reduction services became available in Finland.
“The good thing for me is that the clinic is always here,” said Leila, who uses the services at the centre.
People over 50 years of age account for more than 20% of new HIV diagnosis in Finland. – source HIV point
The centre provides holistic support including medical treatment, health guidance, food and mental and social support.
“By bringing the services to the community and adopting a multidisciplinary approach we have shown that we can successfully reach people who inject drugs who are living with HIV,” said Matti Ristola, Head of HIV Services at the Aurora Day Centre.
2015 was the first year with no AIDS deaths in Finland – source HIV point
“The Aurora Centre in Helsinki is living proof that it is possible to reach 90-90-90 and zero new infections among people who inject drugs when there is political commitment and community engagement,” said Mr Sidibé.
Finland’s Eastern neighbour, Russia, has the third largest number of annual new HIV infections in the world. The proximity between Helsinki and St. Petersburg means that people move easily between the two cities.
There are less than 200 new HIV diagnoses annually in Finland – source HIV point
The visit to the Aurora Day Centre took place in the context of a series of meetings with Finnish decision-makers and politicians. Earlier in the day, Mr Sidibé met Anne-Mari Virolainen, the Minister of Foreign Trade, Annika Saarikko, the Minister of Family and Social Services, Finnish parliamentarians and civil society organizations.
Region/country



Feature Story
Egyptian medical students meet to address stigma and discrimination in health-care settings
25 April 2018
25 April 2018 25 April 2018Stigma and discrimination and other human rights violations occur in health-care settings worldwide, barring people from accessing health services or enjoying quality health care. Such stigma and discrimination further increases the vulnerability of people living with and affected by HIV.
To discuss this problem, nearly 300 Egyptian medical students, representing 18 universities across Egypt, met with representatives of academia, civil society, the government and the Egyptian Medical Syndicate. With support from UNAIDS, the Egyptian branch of the International Federation of Medical Students’ Associations held a one-day consultation on HIV-related stigma and discrimination in health-care settings on 21 April in Cairo, Egypt.
“People living with HIV should have equal rights and opportunities. Denial of access to health-care services is unacceptable. Through this consultation, we aim to inform our national strategy with new interventions for addressing stigma and discrimination,” said Walid Kamal, the National AIDS Programme Manager for Egypt.
During the consultation, the participants took stock of the progress made in addressing stigma and discrimination and decided to hold an ongoing dialogue to identify actions to address stigma and discrimination in health-care settings.
“We are witnessing an unprecedented opportunity for addressing discrimination in health-care settings with political support and programmatic vision. While resources are scarce, we count on the support of medical students as leaders of tomorrow and the power of volunteerism to address this issue,” said Ahmed Khamis, the UNAIDS Country Manager for Egypt.
The participants agreed that accountability mechanisms need to be in place to monitor and evaluate interventions, ensuring that proper actions are taken by the relevant authorities to address rights violations in health-care settings.
“Medical ethics is a must among health-care providers. The Egyptian Medical Syndicate is organizing workshops and conferences to enforce ethics among health-care providers. I would like to remind you all of the rights of patients,” said Sherine Ghaleb, representative of the Egyptian Medical Syndicate.
The participants agreed to prioritize launching the Ministry of Health and Population’s stigma-free policy and integrating HIV-related stigma and discrimination in the module on ethics taught to all doctors who graduate in Egypt. They also agreed to give access to the accountability and investigation mechanism of the Egyptian Medical Syndicate to civil society organizations and people living with HIV in order to report violations and to roll out information on post-exposure prophylaxis in the curricula of medical schools.
The recommendations made during the consultation were endorsed by the National AIDS Programme and will be included in Egypt’s road map for addressing HIV stigma and discrimination in health-care settings. Progress of the road map will be monitored by a group that includes a strong representation from people living with HIV.
Region/country



Feature Story
Mobile phones provide massive potential to move towards e-health systems
26 April 2018
26 April 2018 26 April 2018Shiv Kumar, from Swasti Health Catalyst in India, decided to build a mobile and web application called Taaras (rapid progress). He had watched peer educators work with sex workers in Bangalore, India, and realized that he could make their jobs a lot simpler and more efficient. The south-east Indian city has become a major hub and, as a result, the population has boomed, as have sex workers.
After seeing outreach workers, mostly former sex workers, lugging notebooks and jotting down information and recalling appointments and treatment pickups, he created an app that helps with data collection. “Icons and swipes allow outreach workers to enter all sorts of stuff and swipe and pick up where they left off,” Mr Kumar said. They can also text multiple recipients with reminders and invitations.
“Outreach can no longer be a one-way street. You have to engage the patient,” he said.
The app rolled out in five Indian states in English as well as four regional languages. Since its debut in March 2016, there are now more than 400 users following about 120 000 sex workers.
Bangalore outreach worker Natranity said that she has a lot less paperwork to deal with. “All the data of a particular person is now in one place, versus five or six registers that I had to consult,” she said. Her colleague, Abdul, agreed, “I see about 10 to 15 people a day and what saves me a lot of time is not asking the same questions over and over again, because I can consult their profile.”
The phones had their limits, they explained. “At the initial stage, it’s important to build trust to avoid any discomfort in case they think we are taking photos or recording them,” Natranity said.
Prachi Patel, a technology developer at Swasti, sees Taaras as a bridge to an overall solution. “The app is a helper; outreach workers still do all the talking,” she said. A by-product of the app has been higher engagement with sex workers and an increase in reporting incidents of violence. For confidentiality, the app has a stress password that scrambles the data in the event that someone tries to access the information.
UNAIDS Senior Adviser Philippe Lepère commends such efforts and believes e-health has a huge potential. Not only can it strengthen health systems, it also empowers people to manage their own care. Referring to the World Health Organization’s Guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach, he said that they advocate using text messages to remind people to take their treatment and encourage newly diagnosed people to seek out services.
For this to work, however, he stressed the importance of confidentiality and respect of the user. “Receiving an HIV-related SMS can have drastic consequences in some communities,” he explained. That's why, he said, the content and the frequency have to be ironed out beforehand. “Most importantly, it’s urgent to shift from pilot studies to a larger implementation of programmes at a sufficient scale that can then be integrated within health systems,” Mr Lepère said.
“In certain countries, digital apps have flooded the market and the government has no way of accessing the data or doing any quality control,” he said.
Hani Eskandar, from the International Telecommunications Union, definitely sees mobile phones as paving the way towards universal health coverage.
But, in his view, e-health systems are far from a reality. “Countries have not yet grasped the benefits of this, because they are still focused on vaccines and building hospitals rather than outreach,” he said. He is pushing for governments to rebuild infrastructures that integrate digital platforms.
“It's simple,” he said. “We need for mentalities to change at all levels and stop thinking that the phone is just a gadget.”