

Feature Story
Towards a people-centered approach to the world drug problem
22 October 2015
22 October 2015 22 October 2015Ahead of the United Nations General Assembly Special Session (UNGASS) on the World Drug Problem that will take place in New York in April 2016, senior representatives of several United Nations agencies have taken part in a high-level multi-stakeholder perspective in Geneva, Switzerland. The aim of the event was to explore ways to transform the current drug control system into a measurable response that is people-centered and grounded in respect for public health concerns and human rights.
The meeting, co-hosted and co-chaired by Switzerland and Colombia, covered several key themes that will be further debated during preparatory consultations by the Commission on Narcotic Drugs in Vienna in the run-up to the UNGASS.
Introducing the panel, Switzerland’s Ambassador to the United Nations in Geneva said that stakeholders had already demonstrated their engagement to explore the global drugs issue through the lens of human rights and public health.
“We want to continue to build on this momentum by reiterating our commitment for drugs policies that are people centered and by underscoring the powerful nexus between human rights and public health,” said Ambassador Alexandre Fasel.
In his contribution to the debate, the Executive Director of UNAIDS, Michel Sidibé, said it was crucial for public health to be at the heart of future drug and criminal justice policies.
“The criminalization of people who use drugs is fueling the HIV epidemic,” said Mr Sidibé, “It is an injustice that people who use drugs are being left behind in the AIDS response when we know what works. Investment in harm reduction is a crucial foundation of an efficient drugs policy that not only saves lives but is also cost-effective. Everyone has the right to health.”
Harm reduction strategies such as opioid substitution therapy (OST) and needle-syringe programmes have proved successful in several countries, including Australia, the Netherlands, Portugal and Switzerland. However, less than one third of countries provide needle and syringe programmes for people who inject drugs. People who inject drugs are 28 times more likely to become infected with HIV than the general population. Only 14% of people who inject drugs living with HIV have access to antiretroviral medicines.
Also present on the panel was the Deputy Executive Director of the UNODC, Aldo Lalé-Demoz, who underlined that public health considerations have not been prominent enough in international drug policy and the criminal justice system.
“Public health needs have not been sufficient in international drug policy and the criminal justice system,” he said. “Access to HIV prevention, treatment, and care for people who use drugs is far below what is needed.”
Many panelists stressed that the UNGASS presented an historic opportunity to recast the international response to the world drug problem.
“As we approach next year’s UNGASS, we have a once-in-a-generation opportunity to rebalance international policies on drugs and to increase the focus on public health, on prevention, on ensuring treatment, on care and on harm reduction.” said Marie-Paule Kieny, Assistant Director-General of the World Health Organization.
In a special video message, the United Nations High Commissioner for Human Rights, Zeid Ra’ad Al-Hussein, called on States to consider the decriminalization of the possession and use of drugs and establish stronger public health responses, as recommended by the UN’s Special Rapporteur on the right to health.
“Criminalization of possession and use of drugs causes significant obstacles to the right to health,” said Mr Ra’ad Al-Hussein. “Drug users may justifiably fear that they would be arrested or imprisoned if they seek health care. They may even be discouraged about seeking information about safe practices for drug use.”
Panelists also agreed on the need for alternative development strategies that enabled sustainable livelihoods to reduce dependence on organized crime, drug trafficking and drug production.
Also on the panel were Colombia’s Ambassador to the United Nations in Geneva, Beatriz Londoño Soto, the Chair of the International Drug Policy Consortium, Mike Trace and, appearing via video link from New York, the UN Assistant Secretary-General for Policy Coordination and Inter-Agency Affairs, Thomas Gass.
The high-level panel discussion took place as a group of more than 120 law enforcement officials in the United States called for fewer people to be imprisoned for minor offences including the possession and use of small quantities of drugs.
The Law Enforcement Leaders to Reduce Crime and Incarceration said many inmates jailed for minor offences such as shoplifting and possession of small quantities of drugs were in need of care and treatment unavailable in prisons.
Resources




Feature Story
Twenty-year anniversary of the historic TRIPS Agreement: innovation and access to medicines
02 October 2015
02 October 2015 02 October 2015Twenty years ago, the World Trade Organization (WTO) Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) set international standards to protect intellectual property. The TRIPS Agreement brought about significant changes to intellectual property, with far-reaching implications for the pharmaceutical sector.
During the 2015 WTO Public Forum, on 2 October Trade Works, UNAIDS, Médecins Sans Frontières (MSF), the People’s Health Movement and the Third World Network held a session to discuss developments that have taken place since the TRIPS Agreement was adopted and its impact on accessing medicines in the developing world.
The challenges and opportunities in the public health context were explored during the event. Mariangela Simão, Director of Rights, Gender, Prevention and Community Mobilization at UNAIDS, highlighted the importance of discussing access to medicines under the framework of the recently approved Sustainable Development Goals. “The global community needs to find a balanced intellectual property regimen that works for the achievement of the health targets, including access to innovation, as recommended by the Global Commission on HIV and the Law,” said Ms Simão.
The participants discussed the outcomes of the use of the 2001 WTO Doha Declaration on the TRIPS Agreement and Public Health—a landmark achievement for lessening the impact of intellectual property protection on public health. According to Ellen ‘t Hoen, the use of some mechanisms provided in the Doha Declaration “have helped international agencies like UNICEF and UNITAID to procure affordable generic drugs for least developed countries without any legal impediment, since such countries are benefiting from a TRIPS waiver for pharmaceutical products.”
Preserving the policy spaces paved by the Doha Declaration for the least developed countries will be one of the central issues to be addressed at the upcoming TRIPS Council meeting to be held later this month in Geneva, Switzerland.
Despite the opportunities presented by the flexibilities within the TRIPS Agreement, countries still face difficulties when trying to implement them. New provisions in bilateral and regional free-trade agreements that go beyond what is established under TRIPS are making the policy spaces for the use of such flexibilities even stricter.
The participants also examined intellectual property trends in promoting innovation within the health sector since the adoption of the TRIPS Agreement. Hu Yuanqiong, Legal and Policy Advisor, MSF Access Campaign, noted that the current “patent-centric research and development model is not working to address the health needs, including for people living in the developed world, since the new treatments for hepatitis C and other noncommunicable diseases are simply unaffordable.”




Feature Story
United Nations calls for end of violence and discrimination against LGBTI people
29 September 2015
29 September 2015 29 September 2015Twelve United Nations (UN) entities have released a joint statement calling for an end to violence and discrimination against lesbian, gay, bisexual, transgender and intersex (LGBTI) people. The joint statement highlights the UN’s inter-agency commitment on working with Member States to protect, respect and fulfil the right of LGBTI people to live free from violence, persecution, discrimination and stigma. It also calls on countries to repeal discriminatory laws.
LGBTI people face a wide range of human rights violations. The UN and others have documented widespread physical and psychological violence against LGBTI people in all regions, including murder, assault, kidnapping, rape and sexual violence, as well as torture and ill-treatment in institutional and other settings.
In many countries, the response to these violations is inadequate; in others, human rights defenders challenging these violations are frequently persecuted and face restrictions on their activities. The legislative framework can exacerbate the situation, with 76 countries criminalizing consensual same-sex relationships between adults. These laws expose individuals to the risk of arbitrary arrest, prosecution, imprisonment and even the death penalty in at least five countries.
Punitive environments that marginalize LGBTI people also create significant challenges in responding to HIV. Gay men and other men who have sex with men are 19 times more likely to be living with HIV than the general population, and HIV prevalence among gay men and other men who have sex with men is rising in certain regions, including Asia and the Pacific and Latin America. Transgender women are 49 times more likely to be living with HIV.
In addition to violating the fundamental human rights of LGBTI people, punitive laws severely restrict the ability of LGBTI people to access critical HIV and other health services. Service providers are often forced to stop working, owing to harassment or fear of prosecution.
The UN Secretary-General, Ban Ki-moon, re-affirmed his support for LGBTI rights with a message delivered during last year’s UN General Assembly. “The fight for human rights—and the fight against discrimination—lies at the core of the mission of the United Nations. The fight for equal rights demands global engagement. That is why the United Nations actively works to tackle homophobia and transphobia around the world,” he said.
The UN entities that have signed the joint statement on ending violence and discrimination against LGBTI people are: the International Labour Organization (ILO); the Office of the High Commissioner for Human Rights (OHCHR); the United Nations Development Programme (UNDP); the United Nations Educational, Scientific and Cultural Organization (UNESCO); the United Nations Population Fund (UNFPA); the Office of the United Nations High Commissioner for Refugees (UNHCR); the United Nations Children’s Fund (UNICEF); the United Nations Office on Drugs and Crime (UNODC); the United Nations Entity for Gender Equality and the Empowerment of Women (UN Women); the World Food Programme (WFP); the World Health Organization (WHO); and the Joint United Nations Programme on HIV/AIDS (UNAIDS).





Feature Story
Striving for greater collaboration across health and education in new development agenda
27 September 2015
27 September 2015 27 September 2015Responding to the challenge and opportunity posed by the interconnected Sustainable Development Goals (SDGs), leaders in health and education from across the world came together on the sidelines of the SDG Summit to discuss ways in which the health and education sectors can collaborate and integrate towards joint, people-centered results.
Convened by the Global Partnership for Education, the Global Fund to Fight AIDS, Tuberculosis and malaria, UNICEF and UNAIDS together with the United Nations Foundation and the Global Poverty Project on 26 September 2015, the high-level roundtable stressed the need for adequate financing in health and education to meet the SDGs.
Participants speaking at the event included Julia Gillard, Board Chair of the Global Partnership for Education and former Prime Minister of Australia, Gordon Brown, UN Special Envoy for Global Education, Tedros Adhanom Ghebreyesus, Minister of Foreign Affairs for Ethiopia, Mark Dybul, Executive Director of the Global Fund, and Jan Beagle, UNAIDS Deputy Executive Director. Participants agreed that putting people—particularly women and girls—at the center of the collective health and education efforts will be the key to success in the SDGs.
Adolescent girls, predominantly in sub-Saharan Africa, face higher risks of HIV infection. In 2014, an estimated 60% of all adolescents aged 15-19 years living with HIV were girls. Strong evidence shows that keeping adolescent girls and young women in school reduces the risk of HIV infection. Better educated young women are also more likely to delay sexual debut, to use condoms more frequently, to delay marriage and childbearing and to have better earning potential.
Participants at the event noted that there is significant work to be done to further collaboration between the health and education sectors but that there are good experiences of multisector responses and existing platforms to build on, including those established in the global AIDS response.
Emphasizing how gains in the AIDS response have been proven to maximize impact across other development outcomes, Ms Beagle said: “The AIDS response has shown the value of a multi-sectoral and people-centered approach. From the outset, it was clear HIV was much more than a health issue. It is a development issue, a rights issue, a gender issue that has inclusion of affected communities and evidence and rights-based approaches at its core. Lessons learned from this can be transferred not just to health and education, but across the SDGs.”
Concluding the roundtable, participants committed to continue their engagement, invest in girls’ health and education, focus joint efforts on evidence-based strategies, apply lessons learned through other sectors and monitor success. They stressed the importance of building on the momentum for cross-sectoral collaboration created at the Summit and continuing the dialogue to further advance the integration agenda.












Feature Story
Robert Carr civil society Network Fund receives financial boost at top-level event
29 September 2015
29 September 2015 29 September 2015An active, vibrant and committed civil society has been the mainstay of the global AIDS response for more than three decades and its role is set to become even more critical with the advent of the Sustainable Development Goals and the HIV Fast-Track agenda.
The Robert Carr civil society Network Fund (RCNF) has been committed to strengthening international civil society networks that are active in the challenge to HIV, paying particular attention to underserved and marginalized populations. At a top-level meeting during the 70th session of the UN General Assembly in New York on 29 September, supporters and donors got together to ensure that the fund is replenished and can continue its vital work.
Co-hosts UNAIDS Executive Director, Michel Sidibé and US Global AIDS Coordinator, Ambassador Deborah Birx, joined the Fund’s Chair Michel Kazatchkine and other participants.
Mr Sidibé stressed that community-based organizations were the engine of the AIDS response, engaging in advocacy and research, delivering quality services and reaching people left behind. “Civil society helped break the conspiracy of silence on AIDS. It’s the watchdog, pushing for results,” noted Mr Sidibé. “In this new phase of sustainable development, linking work for healthy people and a healthy planet, we need civil society to advance accountability and ensure shared responsibility. The Robert Carr Fund has shown we can reach all people, and that we can build the political commitment we need.”
The achievements of the RCNF were showcased throughout the meeting, and several participants representing marginalized communities spoke of how they have benefited. These included the AIDS Rights Alliance of Southern Africa’s Felicita Hikuam and Gai Gurung from Thailand’s Youth Lead.
“By working at the regional level we strengthen the capacity of community-based grass roots groups to implement services, to monitor targets, and identify gaps and advocate to address those gaps,” said Ms Hikuam. “Robert Carr was clear about not working in silos. With support of the Fund we are able to work across sectors to build solidarity and move issues forward together,” she added.
Ambassador Birx announced the US Government’s new contribution of USD 10 million to the Fund. “These are the regional organizations that give hope to people at the grass roots. Let’s not underestimate the power of the individual in tackling AIDS. That’s what these community groups are about, standing up to governments and demanding more. Resources from the Fund are about lifting up human beings,” said Ms Birx.
The Fund is named in memory of Jamaica’s Dr Robert Carr who played an integral part in furthering the AIDS response and protecting human rights in inadequately served populations on a national, regional and global level.




Feature Story
Thailand leads the way in the Asia–Pacific region to ensure that all children are born HIV-free
22 September 2015
22 September 2015 22 September 2015“When I was 30 years-old, I was surprised to learn that I was pregnant,” said Prem Paika, who lives in Chiang Mai, Thailand. “My partner, who I had been with for the past eight years, thought he was infertile, so we did not use any birth control.”
Ms Paika was also concerned because she and her partner had been diagnosed with HIV five years earlier. She had been taking antiretroviral medicine for the past few years and went to consult with the doctor overseeing her HIV treatment at a public hospital.
“I was very worried my baby would have HIV, but my doctor reassured me that the antiretroviral medicine would protect my baby,” said Ms Paika.
Untreated, women living with HIV have a 15–45% chance of transmitting the virus to their children during pregnancy, labour, delivery or breastfeeding. However, that risk drops to under 5% if antiretroviral medicines are given to both mother and child through the stages when infection can occur.
Thailand has made the elimination of new HIV infections among children a priority and has consistently adapted its prevention of mother-to-child transmission programme in accordance with the latest research findings. The country is currently following the World Health Organization’s guidelines to provide lifelong antiretroviral medicine to all pregnant women living with HIV. The Ministry of Public Health has implemented measures in its hospitals to ensure that mothers living with HIV receive key services.
“We have developed a system in hospitals where the mother’s confidentiality is guaranteed. Health sector staff have been trained to communicate well with their patients,” said Danai Teewanda, Director from the Bureau of Health Promotion at the Ministry of Public Health in Thailand.
Ms Paika found her regular doctor supportive and she was happy because the hospital provided psychological counselling for her through her pregnancy and until her child was one year old. She could also access her HIV treatment and receive her antenatal check-ups in the same hospital and so did not have to travel from one part of town to another, visiting different specialists.
However, despite efforts by Thailand’s health authorities to create a supportive environment, stigma remains a problem among staff working in other health areas. Ms Paika found that the hospital’s gynaecologist treated her badly and was often misinformed.
“From my first antenatal examination, the gynaecologist encouraged me to have an abortion. He wouldn’t let me see the sonogram as he said in any case there was no point. He told me my baby only had a 2% chance of being born free of HIV.”
Ms Paika turned to her HIV treatment doctor for comfort and her partner complained to the hospital’s director. After this, she found that the gynaecologist treated her better. Finally, the big day arrived: she gave birth to a baby girl.
“They provided her with an antiretroviral prophylaxis and she was tested at one month and then every six months. She was HIV-negative each time. I am so happy she is free of HIV,” said Ms Paika.
Through its efforts, Thailand has achieved remarkable progress in eliminating new HIV infections among children. In 2014, country programme data showed that almost 95% of HIV-positive pregnant women received antiretroviral medicines to reduce the risk of HIV transmission and almost 98% of their babies were born free of HIV.
The country is hoping to further reduce new HIV infections among children. “We have a few weak spots, such as early detection. We are encouraging women to seek antenatal care within the first 12 weeks of their pregnancy,” said Mr Danai.
Since 2013, Thailand has provided free antenatal services to pregnant women at all health centre facilities, promoted HIV counselling and testing for couples and provided antiretroviral medicines to infants as soon as possible after birth. The country hopes by 2016 to have virtually eliminated new HIV infections among children.
Senior government health authorities from Thailand were among representatives from 20 countries who attended the 10th Asia–Pacific United Nations Elimination of Parent-to-Child Transmission of HIV and Syphilis Task Force meeting in Beijing, China, from 15 to 17 September. The meeting examined regional successes, but also roadblocks to stopping new HIV infections among children.
Region/country
Feature Story
Advancing human rights and access to HIV treatment in Argentina
11 September 2015
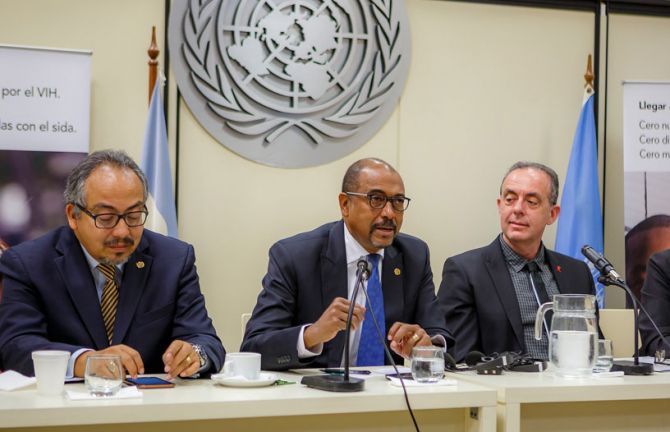
11 September 2015 11 September 2015During an official visit to Argentina from 9 to 11 September, UNAIDS Executive Director Michel Sidibé stressed the importance of keeping human rights issues on the political agenda. He also noted how the AIDS response can be used as a platform to promote social inclusion and the rights of the most marginalized populations.
Mr Sidibé met with government officials, people living with HIV and representatives of civil society and academia. He congratulated Argentina for the results achieved in advancing human rights, especially the rights of lesbian, gay, bisexual, transgender and intersex people (LGBTI).
In 2010, Argentina became the first country in Latin America to allow same-sex marriage, and two years later the National Congress passed a comprehensive Gender Identity Law. Esteban Paulón, President of the LGBTI Federation of Argentina, said that, “In a region with large inequalities, we in Argentina have a moral obligation to work towards advancing the rights and equality we have achieved here beyond our borders.”
The country has also made progress in accelerating access to antiretroviral therapy. Argentina offers treatment free of charge to all people who test positive for HIV, regardless of their CD4 count.
The Minister of Health, Daniel Gollán, expressed the government’s commitment to ensuring that the HIV response is sustainable and medication prices are affordable. “Health is an inalienable and essential human right. There should be no other perspective,” said Mr Gollán. “We are working hard to fight abusive pricing. Companies must be profitable, but prices cannot be impossible to pay, otherwise we deny access.”
According to Pedro Cahn, Director of the Huésped Foundation and former President of the International AIDS Society, access to health services is not enough. More needs to be done to guarantee access to social services and employment opportunities. “HIV is a health problem, but, above all, it is a social problem,” said Mr Cahn.
Patricia Pérez, President of the More Peace Less AIDS Foundation called for the promotion of a culture of peace and respect as “an efficient tool against discrimination, violence in the family and bullying, all of which have an impact on the spread of HIV.”
In Argentina, 130 000 people were living with HIV in 2014, 47% of whom had access to HIV treatment. According to the government, 30% of people living with HIV do not know their status.
Region/country






Feature Story
Photography exhibition aims to reduce HIV stigma and discrimination in Pakistan
07 September 2015
07 September 2015 07 September 2015A photography exhibition portraying the inspirational stories of people living with HIV opened in Islamabad, Pakistan, on 7 September.
A Photo Story on People Living with HIV in Pakistan is a collection of 25 portraits of men and women living with HIV who have taken the decision to share their stories of HIV-related stigma with the public. It is the first exhibition in Pakistan to shine the spotlight on the resilience of people living with HIV. Each photo is accompanied by a short interview in which people express their challenges and concerns, but also their determination to bring about change and eliminate stigma and discrimination.
Nazir Masih, the Chief Executive Officer of the New Lights AIDS Control Society, a non-profit organization dedicated to providing treatment, care and support for people living with HIV, is one of the people portrayed in the exhibition. He said, “HIV is a problem of human beings and it is not an issue of any particular religion or nation. That is why hurdles and threats cannot deter me from the path of helping those in need and will not stop me, come what may, because this is what I have been made for.”
In Pakistan, it has often been difficult to disseminate key HIV information, owing to cultural and social barriers. The aim of this exhibition is to give a human face to the epidemic, with photographs that will have a lasting impact and can be shared on multiple platforms.
“We salute the courage and willingness of the men and women showcased in this exhibition to disclose their status in the hopes of transforming society,” said Steve Kraus, Director of the UNAIDS Regional Support Team for Asia and the Pacific, who inaugurated the exhibition. “Let us embrace our brothers and sisters living with HIV. Only when we reach zero discrimination can we end the AIDS epidemic in Pakistan.”
Stigma and discrimination towards people living with HIV remains a widespread challenge in Pakistan. The country’s People Living with HIV Stigma Index, conducted in 2010, revealed high levels of stigma and exclusion from families and religious activities and discrimination in employment. One third of respondents reported being denied access to health care in the previous 12 months.
Abdul Baseer Khan Achakzai, National Programme Manager, National AIDS Control Programme, said “The Government of Pakistan is committed to scaling up targeted interventions to prevent the rise in HIV prevalence among key and vulnerable populations and to fostering an organized national response to halt new HIV infections, improve the health and quality of life of people with and affected by HIV and initiate community-based HIV testing to bridge the gap between registered and estimated HIV cases.”
The exhibition was produced in collaboration with the National AIDS Control Programme of Pakistan, the United Nations Information Centre and UNAIDS.
Region/country
Related


Feature Story
UNAIDS wins first prize in British Medical Association Book Awards
03 September 2015
03 September 2015 03 September 2015UNAIDS has been awarded first prize in the Popular Medicine category of the British Medical Association (BMA) Book Awards for its book The Bravest Boy I Know.
The prestigious awards were announced at a ceremony on 3 September at BMA House in London. An annual event, the awards aim to encourage and reward excellence in medical publishing, with prizes given out in categories and an overall BMA Medical Book of the Year award made from the category winners.
The Bravest Boy I Know is about two friends, Kendi and Kayla. Kendi is living with HIV. The story is set in Africa and is a heart-warming tale of how the two friends deal with HIV in a positive way. The book conveys the important message that by taking medicine, children living with HIV can live active and healthy lives, while also explaining that the medicines can make children feel unwell and tired.
The judges noted that the book, “Is a unique offering … and is well-presented and engaging. If used appropriately it could be an important public health tool.”
UNAIDS Director of Communications and Global Advocacy Annemarie Hou, accepting the award on behalf of UNAIDS, said, “This is a tremendous honour and recognition that children everywhere need access to high-quality health information.”
The book, which is beautifully illustrated by celebrated artist Sujean Rim, was launched in May 2014 by UNAIDS and the United Nations World Tourism Organization’s Sustainable Tourism for Eliminating Poverty (ST-EP) Foundation at an event attended by the United Nations Secretary-General Ban Ki-moon and Ambassador Dho Young-shim, Chairperson of the ST-EP Foundation. The book is dedicated to Mr Ban for his work in prioritizing education through the Global Education First Initiative, which aims to put every child in school, improve the quality of learning and foster global citizenship.
Speaking at the launch in 2014, Mr Ban said that, “This book, which will be delivered to schools across Africa through ST-EP’s Small Libraries project, will help everyone understand that young people can live normal and fulfilling lives with HIV.”
Ambassador Dho said at the launch in 2014, “As the UN MDGs Advocate for Education, I firmly believe in the power of education to accelerate the achievement of all UN MDGs by 2015, and particularly Goal 6—aimed at HIV. This meaningful collaboration with UNAIDS is creating synergies that will have a powerful impact on the education and the health of children.”
In addition to winning first prize in the Popular Medicine category, UNAIDS was also Highly Commended for The Gap Report in the Public Health category and for The Cities Report in the Health and Social Care category.
Feature Story
More focus on populations and places most in need as United States updates its National HIV/AIDS Strategy
05 August 2015
05 August 2015 05 August 2015The United States of America (US) released an updated AIDS strategy on 30 July which sets the course for its domestic response to HIV over the next five years. The National HIV/AIDS Strategy: Updated to 2020 sets ambitious targets which put particular focus on the people and places most in need.
The US strategy mirrors many of the goals of UNAIDS Fast-Track approach. It calls for 90% of people living with HIV to be aware of their status, aims to increase the percentage of people living with HIV who are retained in medical care to at least 90% and to ensure that 80% of all people diagnosed with HIV have a suppressed viral load which reduces the likelihood of transmitting the virus by around 96%.
Commenting on the new strategy President Obama said that it seized upon rapid shifts in science and policy as more had been learned about the disease. He also said it focused on making sure that every American could get access to life-extending care, no matter who they were, where they lived or how much money they had.
The strategy recommends that efforts be concentrated on people who are being left behind in the response to HIV, namely, gay men and other men who have sex with men, especially African American men, heterosexual African American men and women, young people, people who inject drugs and transgender women. It calls for full access to comprehensive pre-exposure prophylaxis (PrEP) services for those for whom they are appropriate and desired. The strategy also prioritizes certain geographic areas where HIV incidence is high and linkage to, and retention in care is low, including the southern US and specific major metropolitan areas, like Washington, DC.
“I commend President Obama on the bold, new goals set in the updated US strategy which align with the UNAIDS ‘Fast-Track’ approach. The United States joins other nations in pursuit of key prevention, testing and treatment targets that, if met by 2020, put the world on course to end AIDS as a public health threat by 2030,” said Michel Sidibé, Executive Director of UNAIDS.
According to the latest data available from the Centers for Disease Control and Prevention (CDC), there are an estimated 1.2 million people living with HIV in the US, of whom 1 in 8 are unaware of their HIV status. CDC also estimates that 50% of Americans who are diagnosed with HIV are not retained in medical care and that only 37% are accessing life-saving HIV treatment.
At the event to launch the revised strategy, which was held in Atlanta, Georgia, it was also announced that Mayor Kasim Reed had signed the Paris Declaration—Fast-track cities: Ending the AIDS epidemic. In signing the declaration, the mayor has committed to putting Atlanta on the Fast-Track to ending the AIDS epidemic through a set of commitments. Those commitments include achieving the UNAIDS 90–90–90 targets, which will result in 90% of people living with HIV knowing their HIV status, 90% of people who know their HIV-positive status on antiretroviral treatment and 90% of people on treatment with suppressed viral loads, keeping them healthy and reducing the risk of HIV transmission.
The Fast-Track Cities Initiative is supported by its core partners, namely, the City of Paris, the International Association of Providers of AIDS Care (IAPAC), UNAIDS and the United Nations Human Settlements Programme (UN-Habitat).