

Feature Story
“When people are asked to isolate themselves, we also need to make sure that they have food and medicine”
26 May 2020
26 May 2020 26 May 2020When non-essential shops and markets were closed in Senegal in response to the COVID-19 outbreak in the country, and movement between regions in the country was stopped, many people working in the informal sector, including people living with HIV, lost their income. Hunger was dangerously near for many.
Within days, the National Network of Associations of People Living with HIV in Senegal (RNP+) mobilized, setting out to its members the food aid options available from the government for 1 million eligible households and offering advice on how people should prevent themselves from becoming infected by the coronavirus.
“When people are asked to isolate themselves, we also need to make sure they have food and medicine. Communities of people living with HIV help each other to take care of themselves, isolate themselves, access medication when needed and take care of each other’s families,” said Soukèye Ndiaye, the Chairperson of RNP+.
Community leaders and nongovernmental organizations are playing an active role in Senegal in giving out clear and accurate information in order to avoid panic and in combating stigma and discrimination, against both HIV and COVID-19. RNP+ is monitoring the response to COVID-19 as it unfolds, mapping how COVID-19 is affecting the most vulnerable and bringing urgent issues to the attention of the government and service providers.
Advocacy with the National Alliance of Communities for Health and ENDA Santé enabled RNP+ to distributed more than 200 food and hygiene packs to the poorest families of people living with HIV. The UNAIDS country office in the country has stepped in by providing a grant to ensure that the One Family–One Kit programme continues to distribute aid to the people most in need.
RNP+ is also advocating for funding for people living with HIV to help them to travel to health centres, since transport costs have increased, and for financial support for the scaling up of the work of community health workers, who are active in the delivery of antiretroviral therapy.
During the COVID-19 pandemic, ensuring continuity of HIV treatment by distributing multimonth supplies of antiretroviral therapy is vital. Although RNP+ has called on the government for all people living with HIV to get multimonth refills, weaknesses in the supply chain, including inadequate assessments of the needs at some clinics for supplies of antiretroviral therapy and irregular supplies centrally, has meant that not all people who need such supplies are getting them. UNAIDS is supporting the government in tracking orders of antiretroviral medicines and in strengthening the supply chain.
The role of communities, especially communities of the most vulnerable, is critical in the time of COVID-19. “The history of the HIV epidemic has made it clear that the response to an epidemic is only effective if affected communities are fully involved in the response, from its planning through to its implementation and monitoring. Only then can a response be based on the realities and needs of all,” said Demba Kona, the UNAIDS Country Director for Senegal.
Region/country




Feature Story
“We are in this together”: Uganda Young Positives respond to COVID-19
25 May 2020
25 May 2020 25 May 2020Kuraish Mubiru wakes up at dawn every day to get refills of antiretroviral therapy from different health facilities before making deliveries to his peers and other members of the community living with HIV. This has been his routine for the past seven weeks.
Mr Mubiru is the Executive Director of Uganda Young Positives (UYP), a community-based organization that brings together young people living with HIV, mainly from the informal sector. With more than 50 000 registered members, UYP focuses on scaling up HIV prevention, care and support services for its members.
When Yoweri Museveni, the President of Uganda, first addressed the nation on 18 March on the global COVID-19 pandemic, among the measures put in place were restrictions on mass gatherings, the closure of most businesses and the cessation of public transport. Since then, people living with HIV and tuberculosis have found it difficult to access their routine medical care or essential medicine refills.
Following the measures, Mr Mubiru started receiving calls from young people whose livelihoods and HIV treatment were dependent on facilities that had been closed. The impact of the restrictions was beginning to be felt. Young people were no longer able to move to their respective health facilities to access care and treatment nor afford a meal.
Although there have been efforts by health centres and civil society organizations to transport antiretroviral medicines closer to the people, a good number, as reported by the community support groups and health centres, have not received their antiretroviral medicines owing to fear of stigma and discrimination by the community and family members.
“This was a trying time for the community and a huge test of our resilience because our peers needed us more than ever,” said Mr Mubiru. “We had to come out of our comfort zone, act and think fast not to lose all our gains in the national HIV response in the wake of COVID-19.”
Mr Mubiru volunteered to support his fellow peers to access HIV treatment using his own car. In the beginning, he used his own resources to fuel his car and purchase food, but he soon ran out of money.
Initially, one of his biggest challenges was being able to fuel his car to continue with the daily refills, but the further tightening of restrictions on private transport meant that Mr Mubiru could not continue with deliveries. Through the support of UNAIDS, the Infectious Disease Institute and the Ministry of Health, he obtained a permit granting him permission to enable him to continue supporting his community.
During one of his routine deliveries, Mr Mubiru’s car was impounded by the police for more than four hours and he was made to wait. It took the involvement of the police leadership to have the car and Mr Mubiru released. On many occasions, he has been stopped by the police, demanding to know where he is going—those delays at times force him to get home past the curfew time of 19:00.
Mr Mubiru’s resolve to support his community is unwavering. He knows that not everybody would be comfortable visiting the nearest health facility for their antiretroviral refills, disclosing the reason to the local authorities for them to be granted movement or have a community organization’s branded car parked outside their home.
“Instances like these propel me to get out of bed every morning. We are still in this together. COVID-19 will end, and life will continue,” he says.
On average, he delivers eight antiretroviral refills per day to his peers. Besides the long distances and hard-to-reach places he has to go to, food is one of the biggest challenges, since hunger compromises people’s adherence to their medication. Stigma and non-disclosure also pose a great challenge for people to access HIV treatment from a nearby facility.
“The COVID-19 outbreak is having a major impact on people living with HIV,” said Karusa Kiragu, UNAIDS Country Director for Uganda. “We must ensure that adherence to HIV treatment is not compromised. This can be achieved through multimonth dispensing of antiretroviral therapy, supported by a strong community-led response,” she said.
More on COVID-19
Region/country
Related




Feature Story
Modelling the extreme—COVID-19 and AIDS-related deaths
25 May 2020
25 May 2020 25 May 2020Kimberly Marsh, a senior adviser on modelling and epidemiology, has worked for UNAIDS for six years. She supports countries in estimating the impact of the HIV epidemic globally and regionally.
Can you tell me more about the latest modelling report that you are a co-author of, which examines the potential for HIV service disruption in times of COVID-19 in sub-Saharan Africa?
This work looks at potential disruptions in sub-Saharan Africa owing to the COVID-19 pandemic on HIV services that might have an impact on HIV incidence—the number of new HIV infections—and on the number of AIDS-related deaths in excess to those we might have observed if we hadn’t had the COVID-19 pandemic.
We are particularly interested in those question because we know that more than two thirds of all people living with HIV worldwide are living in sub-Saharan Africa. That’s 25.7 million people living with HIV, 1.1 million new HIV infections and around 470 000 deaths from AIDS-related causes in 2018. Among all people living with HIV in the region, 64% of people are on life-saving antiretroviral therapy, which also prevents further new HIV infections.
It is really important that we’re able to ensure they will have access to services. In the models, we looked at service disruptions—a complete disruption of any HIV-related services over a three-month and a six-month period of time. And we looked at the impact after one year and five years. Now remember, these are just scenarios, and extreme ones. We don’t expect this to happen, but it helps us to answer two questions: what HIV-related services are most important to prevent additional deaths and new HIV infections and what might happen if we don’t mitigate or address those disruptions.
From this huge amount of work, what are the two key takeaways?
The modelling work predicted that with a six-month disruption in HIV treatment there could be an excess of 500 000 deaths in sub-Saharan Africa. So, when you look at UNAIDS estimates of AIDS-related deaths over time, that would take us back to about 2008, when we had nearly a million deaths.
There is no doubt about it, HIV treatment is critical. Ensuring that HIV treatment is available to people who need it during the three- to six-month periods is the most important thing that countries can do to prevent excess deaths and HIV incidence. All countries should work to ensure that supply chains are providing them with enough medicines to distribute and that people have sufficient medicines so that they can take them over the coming months.
The second thing to say is that these are projections and that there is still time to ensure that people get the HIV treatment services they need.
Let’s prevent what this model potentially predicts and let’s get HIV medicines to the people who are living with HIV.
What about HIV prevention? Does condom availability have an impact?
The models showed that when you look at prevention services, condom availability impacted the results. I think it is important to say that this is a treatment lesson primarily, but things like access to condoms is really important. We saw around a 20–30% relative increase in HIV incidence over one year if condoms were not available for six months. This is definitely something that we should be focusing on.
Can you tell us a little bit more about the impact on mother-to-child transmission of HIV in these scenarios?
In the scenarios, we looked at the potential for HIV testing services to be disrupted as well as for women to not get medicine to prevent transmission of HIV to their children. And what the various models found was that by removing those medicines—which have had an extremely important impact in terms of reducing new child HIV infections over the past five to 10 years—you could see rises in new child HIV infections in selected countries anywhere up to 162%. It really is critical to maintain prevention of mother-to-child transmission of HIV services.
You have said this was an extreme scenario, not a prophecy, but yet you still believe in modelling?
Models are very important for exploring questions that countries routinely pose to UNAIDS and the World Health Organization in terms of thinking of strategic approaches to responding to HIV in their countries. Models aren’t perfect, but they have a lot to tell us and I think in this instance it really highlights some of the strategies that will be important over the coming months as COVID-19 impacts or potentially impacts sub-Saharan Africa.
Related






Feature Story
UNAIDS and civil society helping stranded people living with HIV
22 May 2020
22 May 2020 22 May 2020A day before Deepak Sing (not his real name) planned to return to India, all international travel ground to a halt—he was stuck in Luanda.
Because of his frequent travel, he had extra HIV medicine, but his supplies started to run low.
“I visited more than 10 pharmacies and explored options of delivery of antiretroviral medicines from India to Angola, but without success,” he said.
He decided that reaching out to Indian colleagues would be his best bet.
“I contacted the Humsafar Trust in Mumbai, and they in turn contacted the UNAIDS India office,” he explained.
Bilali Camara, the UNAIDS Country Director for India, immediately followed up with his peer in Angola. The UNAIDS Country Director for Angola, Michel Kouakou, guided Mr Sing towards the national AIDS institute, which organized a conference call with a medical doctor because one of the medicines that Mr Sing took is not yet in use in Angola. The doctor proposed a substitute and in less than 24 hours he picked up his medication. “Due to the change of one medicine, Mr Sing received only a one-month supply, which will be renewed at his discretion,” explained Mr Kouakou, who has helped two other stranded foreigners in the past month.
“I now believe that humanity exists!" Mr Sing said with great relief.
Since the COVID-19 pandemic hit, UNAIDS has helped stranded people to obtain HIV medicine in countries as diverse as Canada, China, Latvia, Myanmar and Ukraine. Mr Camara said that UNAIDS set up a system so that 700 people from India who were living in Myanmar could access their medicine, since they could no longer access it in India because of the COVID-19 lockdown.
Jacek Tyszko, Senior Programme Adviser at UNAIDS’ Geneva headquarters, has never seen anything like this. So far, he has helped 100 people, mostly in eastern Europe, because of his experience in the region.
“Either I connect people to the local AIDS authority or ideally we link them up to civil society, because they usually have readily available treatment,” he explained. Because of demand, some grass-roots organizations have run out of supplies, which meant some readjusting.
“Overall, the response from local partners has been immediate,” Mr Tyszko said. In certain cases, if stranded people could not get treatment locally, UNAIDS helped them to get supplies from the person’s native country.
He cannot believe how people have had to overcome so many hurdles to obtain HIV medicine despite a clear need.
“In times of crisis like COVID-19 or other public emergencies, governments should waive restrictions to make it easier for people to obtain refills and life-saving care, regardless of their legal status, residency or citizenship,” he said.
UNAIDS has been advocating for the right to health and universal health coverage to alleviate problems like this. A better integration of HIV and other health services could help some of the gaps in the AIDS response to be addressed, which will ultimately make it easier for people to access life-saving medicines, care and support.
For now, Mr Tyszko feels that helping people is very satisfying. “It’s been such a boost to do something so concrete with immediate effect,” he said.
Our work



Feature Story
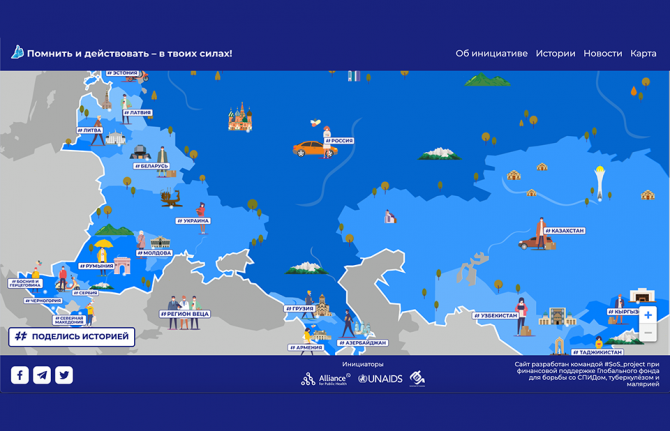
Mapping community responses to COVID-19 and HIV in eastern Europe and central Asia
21 May 2020
21 May 2020 21 May 2020During the COVID-19 crisis, activists and community organizations from across eastern Europe and central Asia are continuing to provide vital HIV prevention, treatment, care and support services.
To map that support, an interactive platform, the Community Initiates Map, has been launched. The website shows how communities are supporting people living with HIV and saving lives during the COVID-19 outbreak in the region, with stories about the services that community organizations are providing. People can learn from the examples of the services developed for key populations and people living with HIV and the impact that they are having on the HIV epidemic and on people’s lives. The map is constantly being updated and people can share their stories on the site.
Vera Brezhneva, UNAIDS Goodwill Ambassador for Eastern Europe and Central Asia, thanked activists for their commitment during the COVID-19 outbreak. “Thank you to every one of you, from all of us. It is in our power to remember and take action. I am with you!” she said.
The experience in eastern Europe and central Asia in the fight against COVID-19 shows that investments made in civil society are good investments. “Communities and nongovernmental organizations have not only come to the forefront of the fight against the new threat, but also in collaboration with medical practitioners and governments continue to provide HIV and tuberculosis services,” said Andrei Klepikov, Executive Director of the Alliance for Public Health.
Nurali Amanzholov, the President of the Central Asian Association of People Living with HIV, said that the coronavirus outbreak and lockdowns had resulted in some people having difficulties in accessing antiretroviral therapy and opioid substitution therapy, and that many people had lost their incomes. “But this situation is also an exam, a test of the strength of our community. And our strength was always in solidarity, the ability to assert our rights, to seek the right solution together,” he said.
Lyubov Vorontsova, of the Central Asian Association of People Living with HIV, said that women living with HIV, especially those in key populations, faced increased gender-based violence and limited access to protection and social services owing to the closure of crisis centres. “We must keep our unity now, so that after the end of the state of emergency, the needs of women remain a priority for the state and civil society,” she said.
“The nearly 40 years of experience in the response to HIV shows that civil society organizations, including communities of people living with HIV, play a crucial role. Today, it is clear that the role of community organizations in emergencies is vital. Countries in the region must recognize those organizations as partners and providers of services for the responses to both HIV and COVID-19,” said Alexander Goliusov, Director, a.i., UNAIDS Regional Support Team for Eastern Europe and Central Asia.
The website was developed by the Alliance for Public Health and the Central Asian Association of People Living with HIV and supported by the UNAIDS Regional Support Team for Eastern Europe and Central Asia.
Interactive platform
Learn more
Region/country
- Eastern Europe and Central Asia
- Albania
- Armenia
- Azerbaijan
- Belarus
- Bosnia and Herzegovina
- Bulgaria
- Croatia
- Cyprus
- Czechia
- Estonia
- Georgia
- Hungary
- Kazakhstan
- Kyrgyzstan
- Latvia
- Lithuania
- Montenegro
- Poland
- Republic of Moldova
- Romania
- Russian Federation
- Serbia
- Slovakia
- Slovenia
- Tajikistan
- North Macedonia
- Türkiye
- Turkmenistan
- Ukraine
- Uzbekistan
Related


 Women, HIV, and war: a triple burden
Women, HIV, and war: a triple burden
12 September 2025

Feature Story
Communities strengthening the AIDS response in Nepal
21 May 2020
21 May 2020 21 May 2020From the very beginning, communities were in the vanguard of the AIDS response in Nepal. Still playing a vital role in the response to HIV in the country, communities are making good-quality services more accessible for people living with HIV and key populations and standing up to HIV-related stigma and discrimination.
“Nepal made antiretroviral medicines accessible to all people living with HIV as a result of advocacy efforts led by communities, human rights activists and other national stakeholders,” said Gopal Shrestha, a prominent community leader living with HIV.
Discrimination towards key populations is still deeply rooted in Nepalese society. “Finding people who need services is difficult due to a lack of trust. We work with those communities that fear coming out because of discrimination,” said Simran Sherchan, Operation Head of the Federation of Sexual and Gender Minorities in Nepal (FSGMN).
Although antiretroviral medicines are available to everyone living with HIV in Nepal, a survey conducted in 2018 reveals that more than 30% of transgender people avoid seeking health care because of fear of stigma and discrimination—something that FSGMN is determined to end.
“Community-based organizations play an intricate role in reaching out to those hard to reach,” said Anjay Kumar KC, a community leader who advocates for harm-reduction in Nepal. Recovering Nepal, a community network of people who use drugs, is supporting harm reduction programmes and HIV prevention among young people who use drugs, including a peer-to-peer programme that provides sterile needles and syringes and a campaign that promotes HIV testing. It has also played a key role in advocating with the government to initiate opioid substitution therapy, which is now offered at 12 sites in five provinces in the country.
Community-based organizations mobilize communities to demand services and advocate for their right to health. Recently, the National Association of People Living with HIV/AIDS (NAP+N) successfully advocated to include people living with HIV in the country’s Health Insurance Programme in 57 districts across the country. “NAP+N also entered into an agreement with Prime Life Insurance Limited to guarantee people living with HIV can access life insurance services,” said Rajesh Didiya, President of NAP+N.
Despite these achievements, community-based organizations face challenges. “When I reach out to sex workers, I have to hide my identity, because sex work is still stigmatized by my family and society. That is why it is difficult to publicly raise awareness about sex workers’ rights,” said Bijaya Dhakal, Coordinator of the Nepal Federation of Female Sex Workers.
Parina Limbu, a community leader who advocates for engagement in decision-making by women who use drugs, said, “Being labelled as women who use drugs, women living with HIV and hepatitis and sex workers, we are not within the reach of programmes. Our needs should not be looked at through the lens of males who use drugs. Women who use drugs need more decision-making spaces to make sure that our voices are heard.”
Those challenges can be overcome through partnerships and joint efforts, however. The Right to Health Women’s Group, Right Here Right Now and FSGMN have created a platform to collect and monitor cases of human rights violations against people living with HIV, key populations and young people. They use the evidence that they collect to advocate for programmes on stigma and discrimination reduction in health facilities and raise awareness about the human rights of key populations with law enforcement officers.
UNAIDS in Nepal has played a key role in empowering communities. “The important role that the community plays in the country’s response to HIV should not be underestimated. The gains made are because communities are taking the initiative and acting in ways that ensure that people who need treatment, prevention and related HIV services can access them,” said Masauso Nzima, UNAIDS Country Director for Nepal and Bhutan.
Video
Region/country
Related




Feature Story
Gender-based violence and COVID-19—“When we are silent, we allow these crimes to multiply”
19 May 2020
19 May 2020 19 May 2020UN Women estimates that globally in the past 12 months 243 million women and girls aged 15–49 years were subjected to sexual and/or physical violence perpetrated by an intimate partner. As a result of the lockdowns imposed to stop the spread of COVID-19, emerging data show that such violence has intensified. In France, for example, reports of domestic violence have increased by 30% since the lockdown started on 17 March, and in Argentina emergency calls about domestic violence have increased by 25% since its lockdown started on 20 March. Many other countries have reported such increases.
Recently, the Odnoklassniki social network, known as OK, hosted a broadcast for experts and others to discuss how to survive lockdown and avoid family conflict and gender-based violence. The broadcast was seen by 1.7 million OK network users across eastern Europe and central Asia.
“I live in Kyrgyzstan,” Ulzisuren Jamstran, a representative of UN Women in Kyrgyzstan, said. “Here, according to the government, the level of domestic violence increased by 65%. We see an increase in aggression against women and children in Kyrgyzstan, we see an increase in suicides among children, even young children.”
Lyudmila Petranovskaya, a Russian psychologist, explained how isolation made good relationships become better and problematic relationships become more problematic. She emphasized that people need to be aware of the options if they are locked down with an abuser. “People have to look for contacts, a hotline, call friends, try to find another place to survive isolation. Staying with the abuser is dangerous. This threat is more serious than coronavirus,” she said.
Julia Godunova, Deputy Head of the Board of the Eurasian Women’s Network on AIDS, spoke about studies in eastern Europe and central Asia that show that more than 70% of women who survived violence do not seek help because of the perceived shame.
Dina Smailova, the founder of the #DontBeSilentKZ nongovernmental organization, addressed female survivors of violence. “When we are silent, we allow these crimes to multiply. I urge women not to be silent. Our movement is expanding, we are active not only in Kazakhstan, but also in other countries of central Asia and beyond.”
The broadcast highlighted successful experiences around the world in responding to gender-based violence. The example in Spain, where women in danger can visit pharmacies and use a code word to alert staff that they need help, was praised. The role of the private sector was also shown to be important—since many shelters are not open at present, hotels are stepping in and providing shelter, either for free or at a minimal cost.
The broadcast was part of a joint initiative of the UNAIDS regional office for eastern Europe and central Asia, the UNESCO Institute for Information Technologies in Education and OK, in partnership with the regional office of UN Women for eastern Europe and central Asia.
When will men stop thinking that women’s bodies are their property?
Related

Feature Story
Kenyan sex workers abandoned and vulnerable during COVID-19
20 May 2020
20 May 2020 20 May 2020During the more than a decade that Carolyne Njoroge worked as a sex worker, she never saw such violence against her peers. Now working full time for the Kenya Sex Workers Alliance (KESWA), she said that the COVID-19 lockdown threw everyone into disarray.
“At the outbreak, no one was prepared for the coronavirus,” she said. “It’s not like the rains that we know and can prepare for.”
The government’s lockdown measures to limit the spread of the virus—a dusk-to-dawn curfew and shutting of bars and nightclubs—have left sex workers in Kenya to either work during the day and be very visible or to break the curfew at night.
So far, KESWA has reported that more than 50 sex workers have been forcefully quarantined during the early days of the pandemic, and women have been arrested for not adhering to the social distancing rules and obligatory mask-wearing.
“How do you expect women to adhere to these measures when they cannot feed themselves and their families and many of them don’t even have homes?” Ms Njoroge asked.
Kenya does not criminalize sex work. However, the law forbids “living on the earnings of sex work” and “soliciting or importuning for immoral purposes,” which Ms Njoroge said means that the women work in a grey area. “It’s a very hostile work environment and sex workers are the first to be violated because they say our work is not work,” she said.
Phelister Abdalla, a sex worker living with HIV and KESWA’s National Coordinator, said, “Sex workers need to be protected, but if we are told to stay at home we need to be given food.”
The government has not released funds or directed aid to sex workers, so KESWA started a fundraiser to dispatch hygiene packs, which include hand sanitizer, masks and menstrual pads, as well as food baskets.
Ms Njoroje said that 100 sex workers from the informal settlements had benefitted. “Our challenge is keeping up with demand, so we are reaching out to others for help,” she said.
Ms Abdalla said that fighting the pandemic together is key. “If we want to end COVID-19, we should not be judged by the type of job we do,” she said. “We are first and foremost Kenyans, so treat all of us equally.”
Fifty-seven Kenyan civil society and nongovernmental organizations, including KESWA, drafted an advisory note to the Kenyan Government to urge it to put in place safety nets to cushion the communities and people who cannot afford to not work. They also urged them to stop security forces from enforcing measures around social distancing and curfews. The note adds, “We cannot use a “one size fits all” approach for COVID-19” and calls upon the United Nations leadership to help safeguard the progress.
The Kenyan Government, through the National AIDS and STI Control Programme (NASCOP), in partnership with county governments, implementing partners and donors continues to work to ensure the continuity of KP service delivery during the confinement measures. NASCOP issued technical guidance to all services including information, education and communication materials e.g. posters, setting up virtual coordination platforms, capacity building of service providers on HIV in the context of COVID-19 and they have instituted advocacy efforts to raise resources to ensure that service providers, including outreach teams, and Key Population led groups have personal protective equipment (PPE) and sanitizers. Mobile dispensing services for people who use drugs and tailored outreaches have been established to enhance service delivery along with the formation of virtual psychosocial support groups distribution of food baskets to the very vulnerable and help/hotlines for violence response have been sustained.
UNAIDS collaborates with governments to ensure that international human rights law are respected, protected and fulfilled, without discrimination, in line with state obligations, including in times of emergency.
Our work
Region/country
Related




Feature Story
COVID-19 community support for Trinidadians on the margins
18 May 2020
18 May 2020 18 May 2020Delores Robinson’s days are usually busy. She heads GROOTS Trinidad and Tobago, a civil society organization that provides psychosocial care for people living with HIV. It also manages a transition house that provides shelter and services for displaced members of key populations.
But since the first COVID-19 case in the country was confirmed, on 12 March, Ms Robinson’s workdays have become a whirlwind. The government’s containment measures—a stay-at-home order and a shutdown of all non-essential business—have thrust the most vulnerable people further into the margins.
GROOTS Trinidad and Tobago is an example of how civil society organizations can move quickly to identify and respond to the needs of the voiceless. Ms Robinson, a Jamaican, has lived in Trinidad and Tobago for the past 34 years. During conversation she alternates between wide, open smiles and a furrowed brow. These days there’s lots to worry about.
Every day she prepares meals for 30 families. She then personally delivers them. There is no structured funding for this effort—just money and other contributions from HIV response stakeholders.
There’s a unique story at each drop-off point. Today she manoeuvres through the narrow roads of Sea Lots, a low-income community in the shadow of the capital city, Port of Spain. The men on the block recognize her car. One offers to deliver her parcel. She laughs. Ms Robinson has come to visit the seven children of a single mother living with HIV who is currently hospitalized.
The Government of Trinidad and Tobago has provided a range of COVID-19 relief options. These include salary relief, rental assistance grants and nutrition support. Sometimes, Ms Robinson’s role is to help clients navigate government systems. For example, one illiterate mother living with HIV lost her food card and needs help getting it replaced.
“The forms are complicated for many people, plus they don’t have an Internet service,” Ms Robinson explained. “Now that we are all being encouraged to conduct business online, many have no access.”
Since the stay-at-home orders went into effect, she’s been asked by the police to accommodate women and children at the transitional home. The combination of income loss and constant contact has exacerbated abusive situations, leading to a spike in reports of domestic violence.
Ms Robinson reports that her clients living with HIV have so far had no problem accessing their treatment. Before COVID-19, it was standard practice for Trinidad and Tobago clinics to dispense two- to three-month supplies of HIV medicines at a time. HIV treatment facilities and sexually transmitted infection clinics remain open, although they have altered hours.
“They have their meds,” she said. “What they need most now is nutritional support to be able to stay healthy and take their treatment.” And they need masks.
UNAIDS Caribbean is advocating for governments in the region to ensure that community organizations like GROOTS are included in decision-making and planning around meeting the needs of vulnerable populations during the COVID-19 crisis. They are an essential service, ensuring that people’s most basic needs are met. These organizations should be included in contingency plans for connecting people living with HIV to services. And they should be resourced.
“We think we’re all in this together, but there are many people who don’t have the things we take for granted—a safe home, healthy food and the ability to speak out. It’s tiring work but it’s needed now more than ever,” Ms Robinson said.
Our work
Region/country
Related


Feature Story
New videos highlight LGBTI issues in Brazil
16 May 2020
16 May 2020 16 May 2020Two new videos released ahead of the International Day against Homophobia, Transphobia and Biphobia, celebrated on 17 May, highlight different aspects of what it means to be part of the lesbian, gay, bisexual, transgender and intersex (LGBTI) community in Brazil.
‘What is the impact of diversity at the workplace? created by the Free & Equal Campaign, in partnership with the UNAIDS, seeks to inspire people by sharing examples of companies committed to tackling discrimination against transgender people in the workplace, in the formal labour market and in the community.
The second video features Brazilian LGBTI people and members of the electronic music scene raising awareness on COVID-19 and its impact on the LGBTI community. In just four days, the video reached more than 100 000 people with a message on the importance of staying at home.
